
To the Editor:
Biologics directed against tumor necrosis factor-α (TNF-α) are highly effective in patients with rheumatoid arthritis (RA)1. There are significant concerns, however, surrounding opportunistic infections including reactivation of Mycobacterium tuberculosis2. Infection with atypical mycobacteria has also been reported3. Mycobacterium heckeshornense is a recently described non-tuberculous mycobacterium species first identified in 20004. There are limited reports of its isolation as a pathogen in immunocompetent patients causing cavitary lung disease, recurrent lung infection, and tenosynovitis4–6. We describe the first reported case of lumbar spondylodiskitis with M. heckeshornense infection in a patient with RA treated with etanercept.
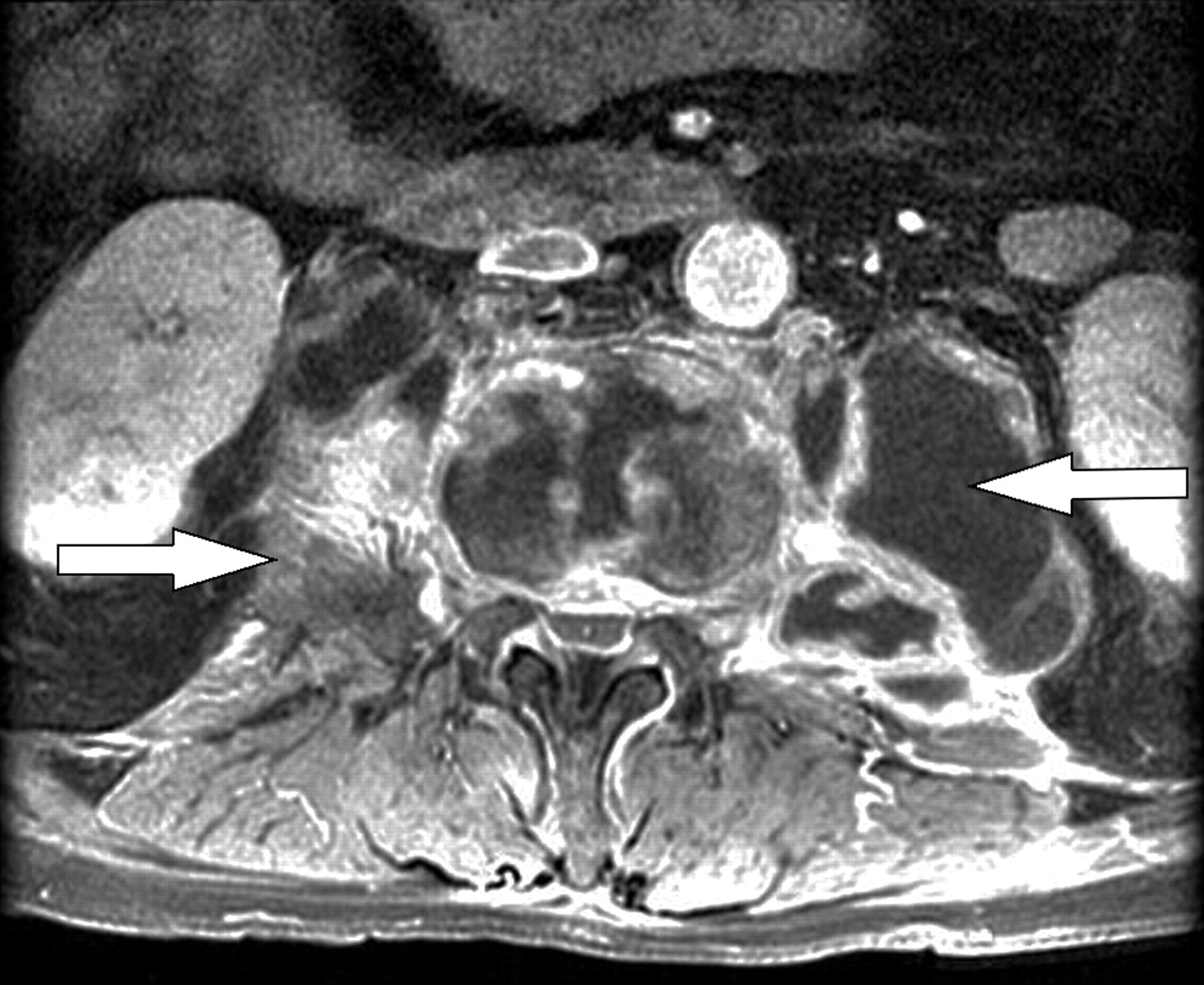
A 51-year-old Caucasian man presented with a 3-month history of lumbar pain with radicular symptoms down the right leg. He had a 5-year history of RA with a right total knee arthroplasty and had been resistant to or intolerant of several disease modifying drugs. He had been treated with etanercept for 3 years with good effect. Chest radiography and tuberculin skin testing were negative prior to starting etanercept. At presentation to hospital he was on etanercept, and corticosteroids had been tapered several months prior. On initial examination, he was in severe pain and guarding his spine when sitting and standing. He was afebrile. Characteristic changes of peripheral joint damage were present without signs of acute inflammation. Neurological examination was unremarkable. His peripheral white cell count was 6.8 × 106/l, erythrocyte sedimentation rate 102 mm/h, and C-reactive protein 168 mg/l. Computed tomography (CT) of the lumbar spine (L) showed spondylodiskitis at L1-2 and L2-3 with kyphotic deformity (Figure 1). Magnetic resonance imaging (MRI) of the lumbar spine revealed bilateral cystic collections tracking into both psoas muscles, suggestive of paravertebral abscesses (Figure 2).
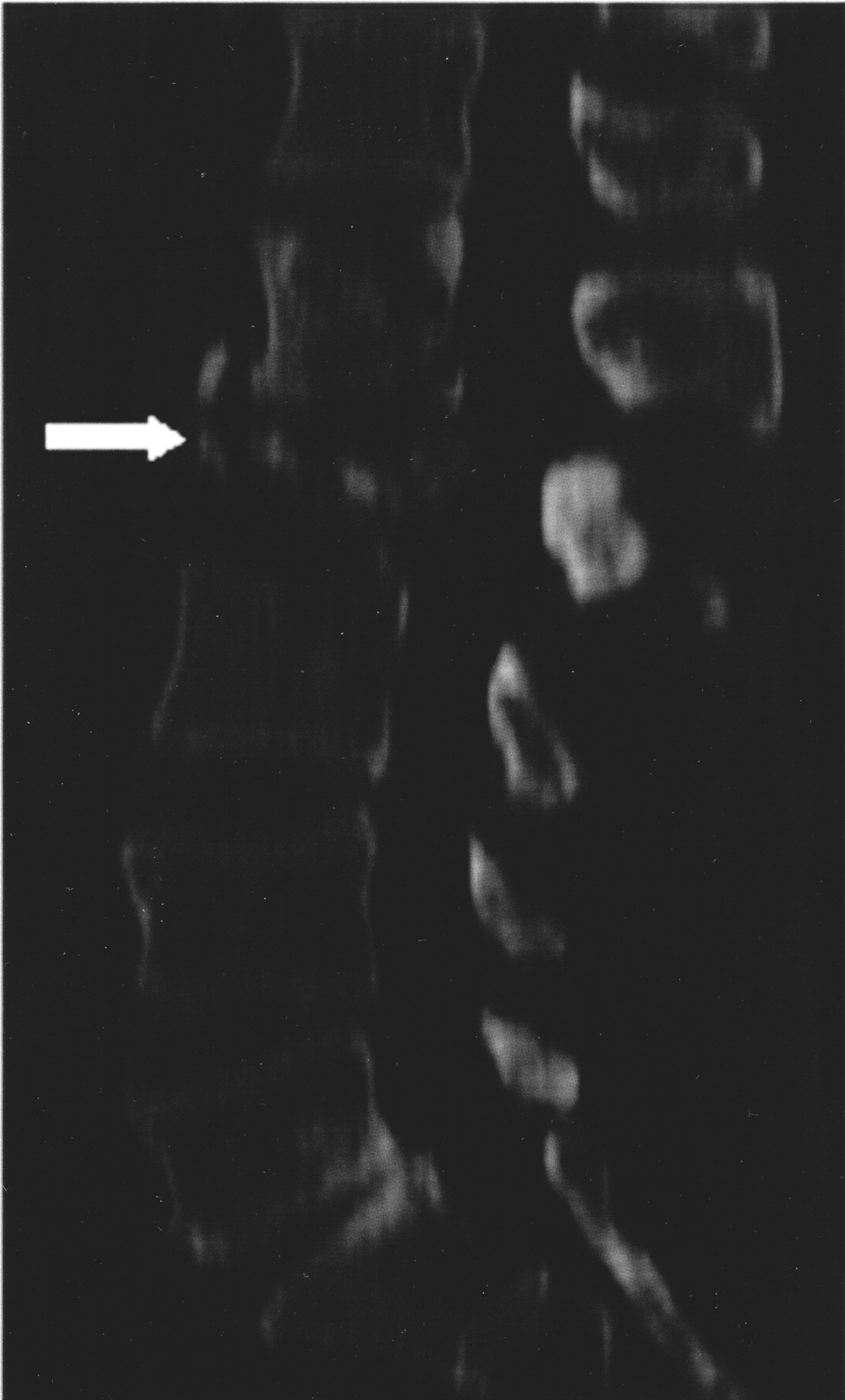
Initial lumbar spine CT scan (sagittal view). Arrow: area of L2 bony destruction and spondylodiskitis at L1-2 and L2.
{kind=link}
{kind=link}
MRI axial imaging of the lumbar spine. Arrows: bilateral paraspinal abscesses.
The patient underwent irrigation and debridment for the paravertebral abscesses. L2 vertebrectomy with insertion of bone graft and T12-L4 instrumented vertebral fusion were performed. The aspirated fluid showed a positive acid-fast bacilli stain. The culture from L2 tissue showed propionibacterium species. Etanercept was discontinued.
A repeated chest radiograph and the tuberculin skin testing (one-step) were negative. Four-drug treatments for presumed reactivation of M. tuberculosis were initiated. Subsequent cultures from the aspirate grew M. heckeshornense identified by 16S RNA sequencing. A prolonged course of clarithromycin, moxifloxicin, and rifampin was prescribed.
M. heckeshornense is a recently described atypical mycobacterium closely related to M. xenopi and differentiated on the basis of 16S rRNA sequencing7. Only a handful of cases of infection have been reported with this organism, most often in immunocompetent patients4–7; most have been pulmonary infections, although there is one report of tenosynovitis5.
On initial presentation of our patient there was appropriate concern regarding the possibility of reactivation of M. tuberculosis. This was in spite of a negative chest radiograph and tuberculin skin test prior to initiating etanercept therapy. It is unknown when or how the M. heckeshornense was acquired in this case. Repeat tuberculin skin testing was negative due to either anergy or failure of the skin test to reflect exposure to M. heckeshornense. To our knowledge this is the first report of this organism causing spondylodiskitis and paraspinal abscesses. This is also the first report of M. heckeshornense in a patient treated with an anti-TNF agent.
Footnotes
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.