
Abstract
Objective. To analyze the relationship between clinical benefits and immunological changes in patients with systemic sclerosis (SSc) treated with autologous hematopoietic stem cell transplantation (HSCT).
Methods. Ten patients with SSc were treated with high-dose cyclophosphamide followed by highly purified CD34+ cells (n = 5) or unpurified grafts (n = 5). Two groups of patients were retrospectively constituted based on their clinical response (good responders, n = 7; and poor responders, n = 3). As well as clinical findings, immunological reconstitution through autologous HSCT was assessed by fluorescence-activated cell sorter analysis, quantification of signal joint T cell receptor rearrangement excision circles (sjTREC), reflecting the thymic function, and foxp3, a key gene of regulatory T cells, mRNA levels.
Results. Patients’ clinical and immunological findings were similar between good and poor responders, or CD34-purified and unpurified groups at inclusion. The sjTREC values were significantly suppressed at 3 months after autologous HSCT in good responders compared with poor responders (p = 0.0152). Reconstitution of CD4+CD45RO− naive T cells was delayed in good responders compared with poor responders. The phenotype of other lymphocytes, cytokine production in T cells, and foxp3 gene expression levels after autologous HSCT did not correlate with clinical response in good or poor responders. Clinical and immunological findings after autologous HSCT were similar between CD34-purified and unpurified groups.
Conclusion. Our results suggest that immunosuppression intensity, sufficient to induce transient suppression of thymic function, is attributable to the feasible clinical response in patients with SSc treated with autologous HSCT. Appropriate monitoring of sjTREC values may predict clinical benefits in transplanted SSc patients after autologous HSCT.
- SYSTEMIC SCLEROSIS
- HEMATOPOIETIC STEM CELL TRANSPLANTATION
- IMMUNOLOGICAL RECONSTITUTION
Systemic sclerosis (SSc) is an autoimmune disease characterized by the presence of skin sclerosis, organ fibrosis, and autoantibodies1. Despite extensive research on autoimmunology and endotheliology, its pathophysiology has been far from conclusive2,3. The skin and organ manifestations of SSc are, in general, slowly progressive and chronically disabling. In some patients, however, they can be rapidly progressive and fatal due to organ involvements such as interstitial pneumonia, arrhythmia, and renal failure. Severe organ involvement frequently occurs within the first 3 years of disease1. These clinical features affect daily living activity and life expectancy in patients with SSc.
Autologous hematopoietic stem cell transplantation (HSCT) has been indicated for patients with autoimmune diseases, resulting in great success particularly in patients with SSc4–10. Autologous HSCT is one of the treatments in patients suffering from hematological malignant diseases. For the practice of autologous HSCT against those malignant diseases, graft manipulation using antibody specific for CD34, a marker of human hematopoietic stem cells, is usually essential to deplete malignant cells from the graft. On the other hand, patients treated with CD34+-selected autologous HSCT (CD34-HSCT) may have infectious complications during hematological recovery more frequently than patients treated with unselected autologous HSCT (unselected-HSCT)11. The graft manipulation was performed in many patients with severe autoimmune diseases treated by autologous HSCT in consideration of depleting autoreactive lymphocytes and inducing profound clinical remission. Meanwhile, it has been debated whether CD34+ cell selection in the graft is necessary or not9,12.
The difference in conditioning regimens is not related to the clinical benefits, and about one-third of transplanted patients do not benefit from these intensive immunosuppressive treatment9,13. Clinical response may depend on profound qualitative immunological changes obtained by autologous HSCT in patients with systemic lupus erythematosus or multiple sclerosis14,15. Little is known as to why and how patients with SSc have clinical benefits of autologous HSCT. The aim of our study was to elucidate the relationship between clinical effect and alteration of immunological profiles in patients with SSc treated with autologous HSCT.
MATERIALS AND METHODS
Patients
Our study was approved by the ethical committee of Hokkaido University and written informed consent was obtained from all participants. Thirty-one patients with SSc, all of whom met the American College of Rheumatology preliminary criteria16, were screened for our study. All patients developing SSc within the last 3 years onset fulfilled at least 1 of the following: early rapidly progressive diffuse skin sclerosis despite continuing treatment, refractory skin ulcers, interstitial lung disease confirmed by lung computed tomography (CT), reversible cardiac involvement such as arrhythmia and cardiomegaly, renal involvement with hypertension, persistent urinalysis abnormalities, and microangiopathic hemolytic anemia. Patients were excluded from the study when they were over 60 years old, or had uncontrolled arrhythmia, left ventricular ejection fraction on echocardiography below 45%, carbon dioxide diffusion lung capacity (DLCO) below 45% predicted, serum creatinine above 176.8 μmol/L (2.0 mg/dl) and glomerular filtration rate (GFR) below 40 ml/min/m2. All enrolled patients were evaluated clinically at the time of diagnosis and on regular visits for followup.
Thirty-five healthy controls were also enrolled in the study.
Transplantation procedure and followup
The mobilization regimen comprised recombinant human granulocyte colony-stimulating factor (rhG-CSF) and intravenous cyclophosphamide (4 g/m2). In 5 patients treated with CD34-HSCT, enriched CD34+ graft, prepared using CliniMACS® system (Miltenyi Biotec, Germany) was stored in liquid nitrate until use for transplant. Graft manipulation was not performed in the next 5 patients treated with unselected-HSCT.
We treated all SSc patients with intravenous cyclophosphamide (200 mg/kg, divided into 4 days) followed by autologous HSCT. rhG-CSF was administered from the second day of transplantation of frozen-thawed autologous enriched CD34+ grafts or frozen-thawed autologous unselected grafts. T cell depleting antibodies such as antithymocyte globulin, antilymphocyte globulin and anti-CD52 antibodies (Campath) were not administered in our patients.
We assessed the improvement of skin sclerosis by the modified Rodnan total thickness skin score (mRTSS). Electrocardiogram and echocardiography were used to evaluate the cardiac function, chest radiograph, chest high resolution CT, and spirometry to evaluate pulmonary function, renogram to evaluate renal function, and serological tests to assess other organ involvement and the presence of autoantibodies.
Lymphocyte phenotyping
Peripheral blood mononuclear cells (PBMC) were prepared from heparinized venous blood by Ficoll-Paque Plus® (Amersham Biosciences Corp., NJ, USA).
We assessed the subpopulation of peripheral lymphocytes by immuno-fluorescence staining of PBMC with anti-human CD3-Cy-Chrome, CD4-fluorescein isothiocyanate (FITC), CD8-FITC, CD19-FITC, TCRγδ-FITC, CD3-phycoerythrin (PE), CD8-PE, CD45RO-PE, CD25-PE, HLA-DR-PE, and CD69-PE (BD Biosciences Pharmingen, San Diego, CA).
The expression levels of interferon (IFN)-γ and interleukin (IL)-4 were studied in the cytoplasm of peripheral CD4+ or CD8+ T cells. Briefly, we stimulated PBMC with phorbol myristate acetate (50 ng/ml) and ionomycin (250 ng/ml) for 6 h in RPMI 1640 containing 10% heat-inactivated fetal bovine serum and monensin (2 μM) at 37°C in 5% carbon dioxide. We evaluated the IFN-γ or IL-4 expression on T cells by staining with anti-CD3-Cy-Chrome, anti-CD8-FITC and -PE, anti-IFN-γ-FITC, and anti-IL-4-PE using Cytofix/Cytoperm Plus® (BD Biosciences Pharmingen) according to the manufacturer’s instructions. Immunostained cells were analyzed using a FACSCalibur™ flow cytometer (Becton Dickinson Immunocytometry Systems, San Jose, CA).
Quantification of thymic signal joint T cell receptor rearrangement excision circles (sjTREC)
Thymic sjTREC on genomic DNA from PBMC was quantified by real-time quantitative polymerase chain reaction (PCR) (ABI PRISM® 7000; Applied Biosystems, Foster City, CA) according to the method of Douek, et al17. The sjTREC values were corrected by the percentage of CD3+ cells in the sample and were then expressed as numbers of sjTREC/μg of CD3+ cells DNA according to the method of Farge, et al18. Values were measured before autologous HSCT, then at 3, 6, and 12 months after autologous HSCT.
Quantification of foxp3 gene expression levels
Total RNA were isolated from PBMC using TRIzol® reagent (Invitrogen, Carlsbad, CA) according to the manufacturer’s instructions. Total RNA (1 μg) was reverse transcribed by ReverTraAce (Toyobo, Osaka, Japan), in the presence of oligo(dT)12–18 primers (Invitrogen) according to the manufacturer’s instructions. We performed real-time PCR using the ABI PRISM® 7000 Sequence Detection System and specific primers for foxp3 and gapdh from TaqMan® Gene Expression Assays (Applied Biosystems).
Statistical analysis
We used the Mann-Whitney U-test to analyze the difference among each value otherwise indicated. The changes in mRTSS and phenotype of lymphocytes after the autologous HSCT were compared with values at inclusion using the Wilcoxon signed rank test. Female-male ratio in each group was assessed using Fisher’s exact probability test. The sjTREC values in healthy individuals were assessed using the Spearman’s correlation test. Calculations were performed using the statistical software package JMP version 5.0 (SAS Institute Inc., Cary, NC). P values less than 0.05 were considered significant.
RESULTS
Between November 2000 and July 2006, 11 consecutive patients meeting the criteria in our study were enrolled and 10 patients were transplanted out of 31 screened patients with SSc for autologous HSCT treatment. One patient was not transplanted because of her mobilization failure. First 5 patients were treated with CD34-HSCT. Subsequent 5 patients were treated with unselected-HSCT. The characteristics of patients treated with autologous HSCT are shown in Table 1. Mean age at inclusion, mean mRTSS before mobilization and mean durations from SSc onset to the treatment were similar between patients treated with CD34-HSCT and unselected-HSCT. Several treatments such as D-penicillamine, prostaglandin derivatives, and corticosteroids were not feasible for our patients. All patients were followed up until July 2007 (40.7 ± 25.6 mos).
Patients’ profile at study inclusion and clinical findings at autologous hematopoietic stem cell transplantation (HSCT).
Mean number of infused CD34+ cells was not different between CD34-HSCT and unselected-HSCT groups. Mean time needed to achieve a neutrophil count greater than 0.5 × 109/l and a platelet count greater than 50 × 109/l were not different between 2 groups. Cytomegalovirus antigenemia were shown in 3 patients out of all transplanted patients. Patient 2 had hemophagocytic syndrome on day 6. Patient 3 had adenoviral hemorrhagic cystitis on day 14 and engraftment syndrome on day 15. Patient 7 had engraftment syndrome on day 12. Hemophagocytic syndrome and engraftment syndrome responded to corticosteroid administration. Hemorrhagic cystitis was refractory to acyclovir, vidarabine, ganciclovir, or ribavirin. Patient 3 had the second autologous HSCT using unselected grafts at 3 months after first autologous HSCT using selected CD34+ cells due to recurrent infectious diseases.
Four out of 5 transplanted patients have more than a 25% fall in the skin score compared with baseline values in both groups (Figure 1). Dermal thickness assessed by skin biopsy was also improved in these patients with clinical benefits (data not shown). Additional unselected-HSCT at 3 months after CD34-HSCT did not affect Patient 3’s skin manifestation. Cardiac and pulmonary functions were not altered significantly through the treatment in all patients (data not shown). Their serum level of γ-globulin almost remained normal range through autologous HSCT (data not shown). Their serum level of anti-Scl70 antibodies reduced except Patient 2 treated with CD34-HSCT (data not shown). Transplantation related complications during hospitalization are shown in Table 1. There was no significant difference in the incidence of adverse events between both groups and no transplantation related mortality.

Evaluation of modified Rodnan total thickness skin score (mRTSS) in patients with systemic sclerosis. A. Changes of mRTSS in patients treated with CD34-HSCT. B. Changes of mRTSS in patients treated with unselected-HSCT. Proportional change from baseline measurement was calculated for each patient at each available timepoint. * p < 0.05.
We compared immunological reconstitution profile over time between good and poor response groups, and between CD34-HSCT and unselected-HSCT groups. First, we analyzed immunological reconstitution between good and poor response groups. Clinical response to therapy was categorized into major, partial, or no response, or disease progression or relapse according to the method of Farge, et al13. According to the observed clinical response compared to these criteria, 2 groups of patients were retrospectively constituted: good response group, consisting of 7 patients with sustained major or partial response, and poor response group, consisting of 3 patients (Patient 5, 6, and 7) with no response or with relapse of disease (Table 2). Our patients were evaluated by functional evaluation (performance status and/or health assessment questionnaire) and mRTSS with skin improvement assessed by skin biopsy. Each organ function was not altered significantly through the treatment in all patients. Mean age at inclusion, mean mRTSS before mobilization, and mean durations from onset scleroderma to treatment were similar between both groups. At inclusion, the ratio of CD4/CD8, the percentage of CD4+CD45RO+, CD4+CD45RO−, CD19+, CD4+CD25+, CD56+, CD3+TCRγδ+, IFN-γ- and IL-4-producing CD4+ and CD8+ cells were in the normal range for all patients and were not different between good and poor response groups (Table 3). After autologous HSCT, shortened CD4/CD8 ratio was sustained due to delayed CD4+ cell recovery and prompt CD8+ cell recovery in both groups. CD4+CD45RO−naive T cells remained low at 6 months after autologous HSCT in good response group, and CD4+CD45RO− cells reconstituted faster in poor response group (p < 0.05). CD19+ and CD56+ cells returned into the normal range at 3 months in both groups. The kinetics of other cells through autologous HSCT was not statistically different between good and poor response group in the study. To evaluate the T cell response against mitogen stimulation after autologous HSCT, mean fluorescence intensity of CD69 on CD3+ cells was investigated. CD69 expression levels on CD3+CD8+ and CD3+CD8− cells against mitogen were not different between healthy controls and patients with SSc before autologous HSCT, and its kinetics through autologous HSCT were similar in both groups (Table 3). Cytokine production in CD3+CD8− and CD3+CD8+ T cells was assessed by intracellular staining of IFN-γ and IL-4. Levels of cytokine production in CD3+CD8− and CD3+CD8+ cells were not different between both groups. IFN-γ producing CD8+ T cells increased after autologous HSCT in both groups (Table 3).
Patients’ profile between good and poor response groups at autologous HSCT.
Phenotype analysis of lymphocyte population through autologous HSCT between patients with good and poor clinical response. Value are mean ± SD.
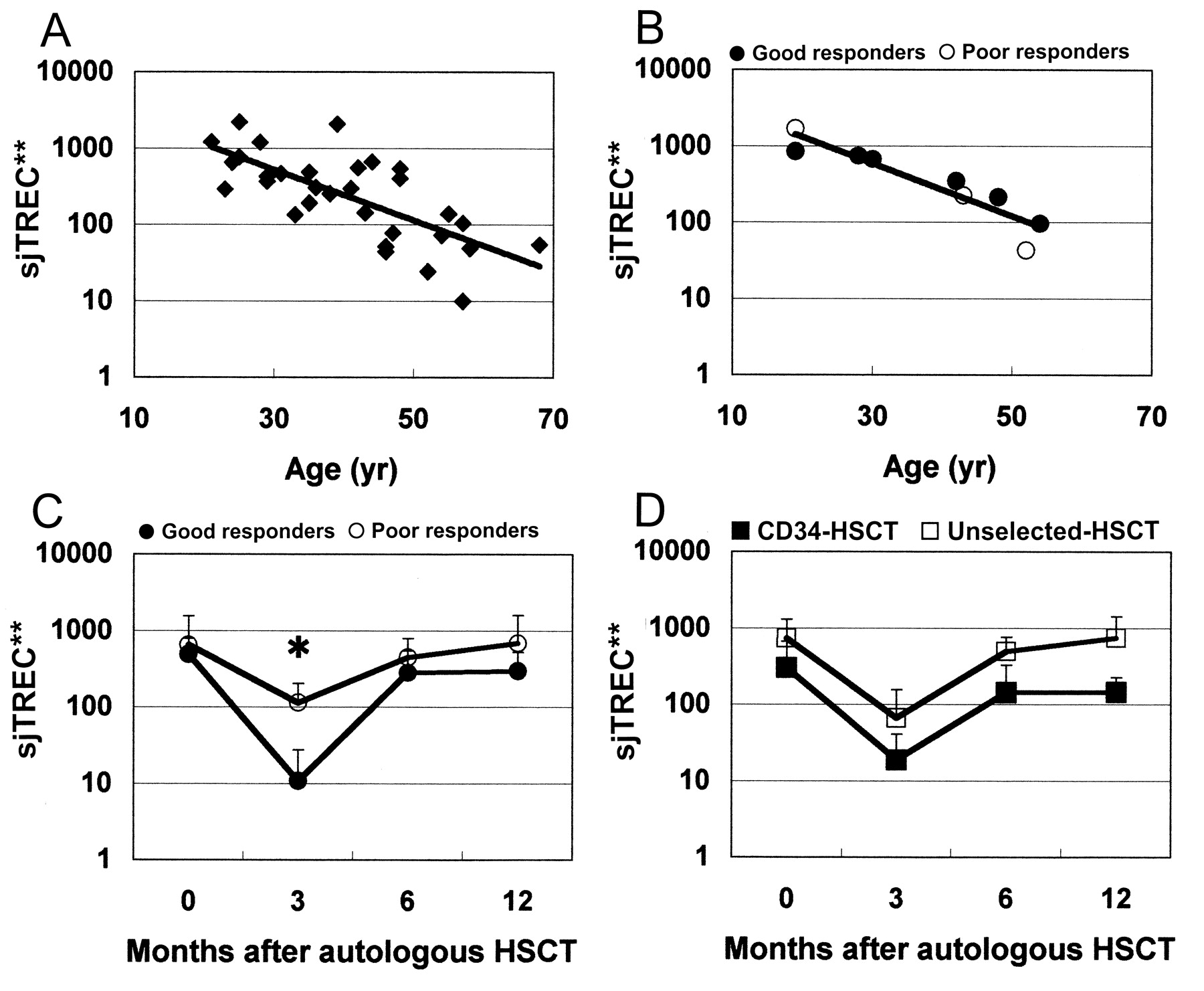
Thymic output assessed by sjTREC was analyzed to evaluate the mechanism of peripheral CD4+CD45RO− and CD4+CD25+ proliferation. In healthy controls, the sjTREC values negatively correlated with their age (Figure 2A, p < 0.0001, r2 = 0.44). Nine out of 10 transplanted patients could be analyzed in the study. Their sjTREC values also negatively correlated with their age at inclusion of autologous HSCT (Figure 2B, p = 0.002, r2 = 0.80). The sjTREC values were not significantly different between patients with SSc before autologous HSCT and age- and sex-matched healthy controls (p = 0.8253). The sjTREC values were significantly suppressed at 3 months after autologous HSCT in the good response group compared with poor responders (Figure 2C, p = 0.0152), although the values were not different at inclusion, 6 and 12 months after autologous HSCT between both groups.

{kind=link}
{kind=link}
sjTREC values in CD3+ cells in healthy individuals and its kinetics through autologous HSCT. A. Relation between age and numbers of sjTRECs in healthy controls. B. Relation between age and numbers of sjTREC in SSc patients treated with autologous HSCT. C. sjTREC between good and poor response groups. D. sjTREC between patients treated with CD34-HSCT and unselected-HSCT. Logarithmic scales were used for y-axes to compress the figure. * p = 0.0152. **copies/μg in CD3+ cells DNA.
Foxp3 is a key regulatory gene for the development of regulatory T cells19. Foxp3 gene expressions in PBMC were analyzed to assess the relationship between the recovery of CD4+CD25+ cells including regulatory T cells and clinical benefits in transplanted SSc patients. Foxp3 gene expressions in PBMC were within the normal range through autologous HSCT and were not different in the 2 groups (Table 3).
Next, immunological reconstitution was analyzed between CD34-HSCT and unselected-HSCT groups to assess how graft manipulation affected immune system and clinical response. At inclusion, the ratio of CD4/CD8, the percentage of CD4+CD45RO−, CD4+CD45RO+, CD19+, CD4+CD25+, CD56+, CD3+TCRγδ+, IFN-γ, and IL-4 producing CD4+ and CD8+ cells were in the normal range for all patients and did not differ between CD34-HSCT and unselected-HSCT. After autologous HSCT, CD4/CD8 ratio remained low in both groups. In CD4+ subsets, CD4+CD45RO−, CD4+HLA-DR+, and CD4+CD25+ cells increased rapidly in unselected-HSCT compared with CD34-HSCT at 12 months (p < 0.05, Table 4). CD19+ and CD56+ cells returned into the normal range at 3 months in both groups. CD69 expression levels on CD3+CD8+ and CD3+CD8− cells against mitogen were not different between healthy controls and patients with SSc before autologous HSCT, and its kinetics through autologous HSCT were similar in both groups (Table 4). Levels of cytokine production in CD3+CD8− and CD3+CD8+ cells were not different between both groups. IFN-γ-producing CD3+CD8+ T cells increased after autologous HSCT in both groups (Table 4).
Phenotype analysis of lymphocyte population through autologous HSCT between patients with CD34-HSCT and unselected-HSCT. Values are mean ± SD.
Cytokine production in CD8− and CD8+ T cells was assessed by intracellular IFN-γ and IL-4. Cytokine production in CD8− cells was not different between both groups. IFN-γ- and IL-4-producing CD8+ T cells increased after autologous HSCT in both groups (Table 4).
The sjTREC values recovered to the levels at inclusion between 6 to 12 months after CD34-HSCT or unselected-HSCT. There was no statistical significance through their clinical course in both groups (Figure 2D).
Foxp3 gene expressions in PBMC were within the normal range through autologous HSCT and not different in the 2 groups (Table 4).
DISCUSSION
We described the efficacy and the safety in patients with SSc treated with autologous HSCT. More than a 25% decrease in the skin score, which correlates with patient’s survival20, was achieved in 8 out of 10 transplanted SSc patients. Skin improvement was not significantly different between CD34-HSCT and unselected-HSCT groups. In addition, additional unselected-HSCT did not lead to recurrence or adverse effect on skin manifestation in Patient 3. These results suggest that graft condition did not affect the clinical outcome on skin involvement up to 12 months after autologous HSCT in our series.
Few data on thymic function and lymphocyte phenotypes after autologous HSCT have been reported in transplanted SSc patients13,18,21. The TREC values might be related to clinical response in our transplanted patients. In the last decade, basic and clinical scientists have focused a role of sjTREC as a marker of human thymic function22. Values of sjTREC can also reflect the pathophysiology in patients with autoimmune diseases. The sjTREC values may be affected by disease activity in patients with systemic lupus erythematosus23. Age-inappropriate T cell senescence confirmed by decreased frequency of sjTREC may also contribute to the development of juvenile idiopathic arthritis24. There was no evidence to prove an age-inappropriate T cell senescence and a correlation between the sjTREC values and disease condition in our patients with SSc. Thymic function assessed by sjTREC values is significantly suppressed at engraftment, recovers within 3 months after autologous HSCT, and is age-dependent in adults17,25. In our series, the lower level of sjTREC at 3 months after autologous HSCT was shown in the good response group without dependence on their age and graft condition. Longterm defects of CD3+CD4+ cells, especially CD4+CD45RO−naïve T cells, after autologous HSCT might also reflect profound suppression of thymopoiesis in the good response group. Thymus-dependent immunological reconstitution leads to the T cell precursor reeducation and renewal of the T cell repertoire, and may induce remission of autoimmunity26,27. Our results suggest that transient, profound suppression of thymic function might alter immune condition, leading to clinical response in patients with SSc.
Peripheral immunological reconstitution after autologous CD34-HSCT or unselected-HSCT has been well documented in patients with hematological disorders28–30. While CD56+ cells, followed by CD19+ cells, recover promptly after autologous HSCT, CD3+ cells, especially CD4+CD45RO− cells, remain low after autologous HSCT in CD34-HSCT and unselected-HSCT29,30. After the initial 2 months of autologous HSCT, IFN-γ-producing CD8+ or CD8− T cells remain normal or increased11,30. In our series, kinetics of lymphocytes recovery is similar to these previous results. In patients with SSc, peripheral blood T cells show a predominantly type 2 T-helper profile, and can induce fibrosis through the production of cytokines, especially IL-42. Cytokine production in T cells at inclusion was not significantly different between our transplanted patients with SSc and healthy controls. The kinetics of IFN-γ- and IL-4-producing T cells after autologous HSCT was not different between CD34-HSCT and unselected-HSCT, or good and poor response groups. Therefore, the significance of cytokine production in T cells after autologous HSCT was not conclusive. In good response group with sustained major or partial response, phenotype or function of peripheral lymphocytes was not significantly different from that of poor response group through autologous HSCT. These results suggest that changes in peripheral immunity were not correlated with clinical response.
CD4+CD25+FOXP3+ regulatory T cells may play a role in the immunological reconstitution leading to the improvement of autoimmune disease or prevention of graft-versus-host disease after autologous or allogeneic HSCT31,32. Although CD4+CD25+ population increased at 12 months after autologous HSCT in unselected-HSCT compared with that in CD34-HSCT, it is noted that there was no difference between good and poor response groups, and foxp3 gene expression levels did not correlate with the clinical response or with graft condition. CD4+CD25+ populations include non-regulatory activated T cells as well as regulatory T cells32. Increased CD4+CD25+ population might reflect the activation of CD4+ T cells because CD4+HLA-DR+ population also increased at 12 months in unselected-HSCT group. Therefore, the role of CD4+CD25+ regulatory T cells on clinical response was not evident in our study.
Although the importance of graft manipulation in autologous HSCT for autoimmune diseases has been debated, clinical outcome may not necessarily correlate with the autoreactive clone survival after CD34-HSCT33. In patients with rheumatoid arthritis, a pilot study showed that clinical response and laboratory findings were also similar between CD34-HSCT and unselected-HSCT12. In addition, autoimmunity after autologous HSCT may result from the type of conditioning regimen rather than graft condition (i.e., CD34-HSCT or unselected-HSCT)34. Although peripheral immunity after autologous HSCT does not have a decisive impact on disease control in our transplanted SSc patients, further study will reveal the role of peripheral immunity after autologous HSCT. Our results suggest the relationship between clinical benefits and immunosuppression intensity sufficient to suppress thymic output by the treatment.
The results of our study suggest that immunosuppression sufficient to downregulate thymic function, rather than the graft manipulation, can lead to clinical benefits in patients with SSc. Additionally, appropriately monitoring the sjTREC values after autologous HSCT may serve to identify patients who would not achieve clinical remission by autologous HSCT and additional treatment in a more timely way.
Acknowledgments
We thank Drs. Masaya Mukai (Sapporo City General Hospital), Satoshi Jodo (Tomakomai City Hospital), Katsunori Onishi (Sapporo Social Insurance General Hospital), Hideki Kasahara (NTT East Corporation Sapporo Hospital), and Noriyuki Sakurai (Minami Sapporo Hospital) for clinical procedures.
Footnotes
-
Supported by a grant from the Japanese Ministry of Health, Labor and Welfare.
- Accepted for publication January 8, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.