
Abstract
Objective. To describe the onset, clinical features, prognostic factors, and treatment of adult-onset Still’s disease (AOSD) in cases from China.
Methods. Sixty-one Chinese patients with AOSD were analyzed retrospectively.
Results. Common clinical features were fever (100.0%), rash (88.5%), and arthritis (82.0%). The laboratory findings were as follows: leukocytosis (83.6%), increased erythrocyte sedimentation rate (100.0%), elevated transaminase concentrations (23.0%), elevated ferritin levels (79.6%), negative antinuclear antibody (88.5%), and negative rheumatoid factor (88.5%). Of the 61 patients, 44.3% exhibited a monocyclic disease pattern, 29.5% experienced disease relapse at least once, 16.4% exhibited chronic articular course, and 9.8% died; most deaths were due to pulmonary infection and respiratory failure. Based on the disease course, we divided the 61 patients into 2 groups: those with favorable outcome (cyclic disease course, n = 45) and unfavorable outcome (chronic disease course or death, n = 16). We analyzed the prognostic factors for the 2 groups, and found that pleuritis, interstitial pneumonia, elevated ferritin levels, and failure of fever to subside after 3 days of prednisolone at 1 mg/kg/day were unfavorable prognostic factors for patients with AOSD.
Conclusion. Patients with AOSD had complex symptoms with no specific laboratory findings. Our results indicate that AOSD is not a relatively benign disease, especially in cases that are refractory to high doses of prednisone.
- ADULT-ONSET STILL’S DISEASE
- REFRACTORY
- PROGNOSIS
Adult-onset Still’s disease (AOSD) is an inflammatory disease of unknown etiology. AOSD is characterized by a typical spiking fever, arthritis, rashes, leukocytosis, and involvement of various organs1,2. Since it was first described by Bywaters3 in 1971, cases of AOSD have been reported worldwide4–20.
Treatment of AOSD remains empirical. Nonsteroidal anti-inflammatory drugs (NSAID), steroids, and antirheumatic agents have been used to control fever, arthritis, and systemic disease. About 80% of patients with AOSD require glucocorticoid therapy, particularly when the disease manifestations are severe1. Glucocorticoid therapy can be administered as oral prednisone in daily doses of 0.5–2 mg/kg, in doses as high as 3 mg/kg, or as methylprednisolone pulses21. For the prognosis of AOSD, many studies have claimed that the outcome of AOSD is favorable11,18,22. However, some studies report that some patients had a “chronic disease course” or a “poor prognosis,” and some patients have died of infection, liver involvement, amyloidosis, adult respiratory distress syndrome, heart failure, and macrophage activation syndrome4,23–25.
Determining whether the clinical features, laboratory tests, and response to therapy can predict or are related to the outcome of AOSD would be of value to clinicians. We describe the clinical features of 61 patients with AOSD treated in our hospital, and analyze the prognostic and risk factors associated with unfavorable outcomes in these patients.
MATERIALS AND METHODS
We retrospectively evaluated 61 AOSD patients [45 women, 16 men ages 37.5 ± 14.8 years (range 21–63 yrs)] who had been under regular medical super-vision at the Department of Rheumatology at Renji Hospital affiliated to Shanghai Jiaotong University. The study was approved by the Institutional Review Board of Shanghai Jiaotong University.
All the patients fulfilled the preliminary criteria of AOSD proposed by Yamaguchi, et al7. Investigations to exclude infections, malignancies, and other autoimmune disorders were carried out for all patients. Microbiology investigations, imaging studies, and bone marrow and lymph node biopsies were performed when indicated. Antinuclear antibody (ANA), anti-dsDNA antibody, and antineutrophil cytoplasmic antibody were routinely investigated to exclude other autoimmune diseases. The mean number of major and minor Yamaguchi criteria fulfilled by the patients was 3.5 and 2.4, respectively.
Remission was defined as the absence of articular, systemic, and laboratory evidence of disease activity for at least 2 consecutive months. Recurrence was characterized by recurrent systemic or articular flares occurring after complete remission and requiring therapy16. With respect to the disease course, the patients were classified into 4 groups as described by Cush, et al4. Monocyclic systemic pattern was defined as a single episode lasting < 1 year followed by a prolonged remission throughout the entire followup period. Polycyclic systemic pattern was characterized by recurrent systemic flares with or without articular manifestation; the episode usually persisted < 1 year; there was complete remission between flares. Chronic articular disease was defined as the persistence of articular symptoms for > 1 year in the absence of systemic features. According to the systemic findings noted during the initial or recurrent attacks, chronic articular disease was subdivided into 2 categories, namely, chronic articular monocyclic systemic pattern and chronic articular polycyclic systemic pattern.
The following clinical information was recorded: demographic data, relevant clinical details, and the laboratory tests and medicines used in the course of the disease. A patient having a monocyclic or polycyclic systemic disease course was assigned to the favorable outcome group, and a patient having a chronic articular disease course or death was assigned to the unfavorable outcome group. Some of the demographic and relevant clinical data and the laboratory tests and medicines were used to analyze the prognostic and risk factors associated with an unfavorable outcome.
In statistical analysis for the ultimate outcome of AOSD, failure of fever to subside after 3 days of prednisolone 1 mg/kg/day (i.e., patient had persistent fever with no evident infection despite administration of prednisone 1 mg/kg/day for at least 3 days) was used as a prognostic factor for survival analysis.
Statistical analyses were performed using the SPSS software. Descriptive statistics are represented as mean ± standard deviation. Logistic multiple regression analyses have been used for determining the prognostic risk factors. A p value < 0.05 was considered statistically significant.
RESULTS
Clinical manifestations
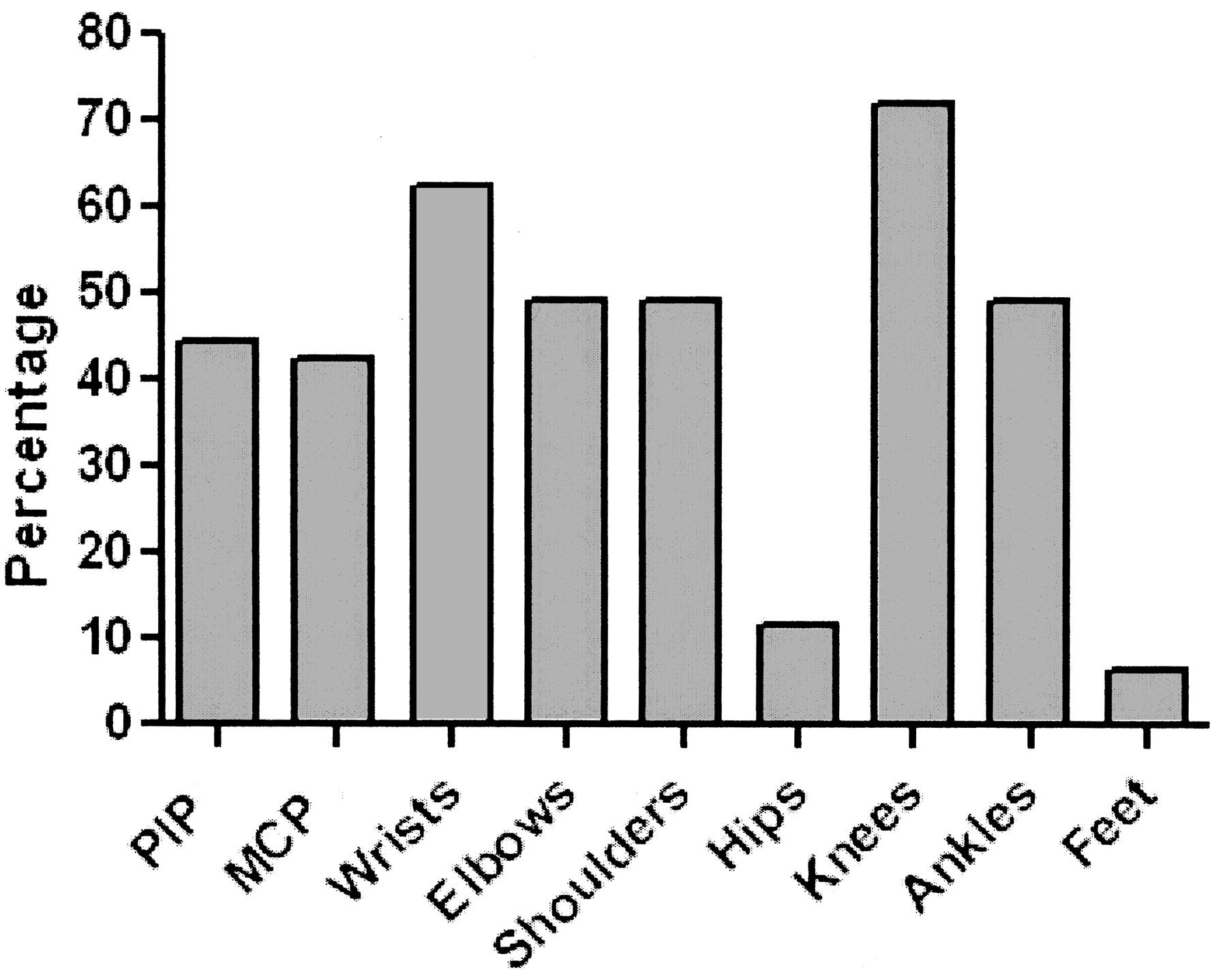
Clinical data are shown in Table 1. All patients had fever with body temperature ≥ 39°C for more than 2 weeks; the fever was remitting or irregular in most patients, and no patient had continuous fever. A typical salmon-pink macular or maculopapular rash was observed in 54 (88.5%) patients, mostly involving the trunk and the upper and lower extremities. Arthritis was noted in 50 (82.0%) patients. Figure 1 presents the distribution of arthritis among the patients.

The distribution of arthritis among 61 AOSD cases. PIP: proximal interphalangeal joints; MCP: metacarpophalangeal joints.
Comparison of clinical features of patients with AOSD between our series and previous series. Data are no. (%).
A total of 44 (72.1%) patients complained of sore throat that usually coincided with the fever spike and subsided when the body temperature returned to normal. The throat was diffusely red but without exudates. Lymphadenopathy was observed in 32 (52.5%) patients, and the cervical region was frequently involved. Lymph node biopsy was performed in 9 patients, and revealed reactive hyperplasia in 7 patients, chronic lymphadenitis in 1 patient, and inflammatory hyperplasia in 1 patient.
Laboratory test results
Laboratory results are shown in Table 2. ANA and rheumatoid factor (RF) were negative in 54 (88.5%) patients; the ANA titer in the ANA-positive cases was < 1:320, and the RF level in the RF-positive cases was 20.8–106 IU/ml (reference value < 20 IU/ml). For ANA-positive patients, the diagnosis of systemic lupus erythematosus could be excluded according to American College of Rheumatology criteria26. All patients had negative blood cultures on more than 1 occasion. Interstitial pneumonia was revealed by thoracic computed tomography (CT) in 7 (11.5%) patients.
Comparison of laboratory results of patients with AOSD between our series and previous series. Data are no. (%).
Disease course and followup
The mean followup period was 3.6 ± 2.9 years (range 6 months–14 years). Table 3 presents the comparison of the disease course and followup findings of AOSD between our series and other reports. The manifestation pattern of the recurrence was similar to that of the first episode. In our series, 6 (9.8%) patients died: 4 of severe pneumonia and respiratory failure, 1 of liver failure, and 1 of hemophagocytic syndrome.
Disease course and followup findings of patients with AOSD in this and other reports. Data are no. (%).
During the disease course, except for 2 patients who had good response to a combination of NSAID and methotrexate (MTX), almost all patients received corticosteroids due to insufficient response to NSAID. Of the 61 AOSD patients, 30 (49.2%) received a maximal dose of prednisolone (0.5–1 mg/kg/day) and 27 (44.3%) received a high dose of methylprednisolone (range 80–500 mg/day). MTX was administered to 47 (77.0%) patients: chloroquine/hydroxychloroquine to 19 (31.4%), leflunomide to 7 (11.5%), and thalidomide to 3 (4.9%). Different combination therapies with NSAID, steroids, and disease-modifying antirheumatic drugs (DMARD) were administered to 38 (62.3%) patients.
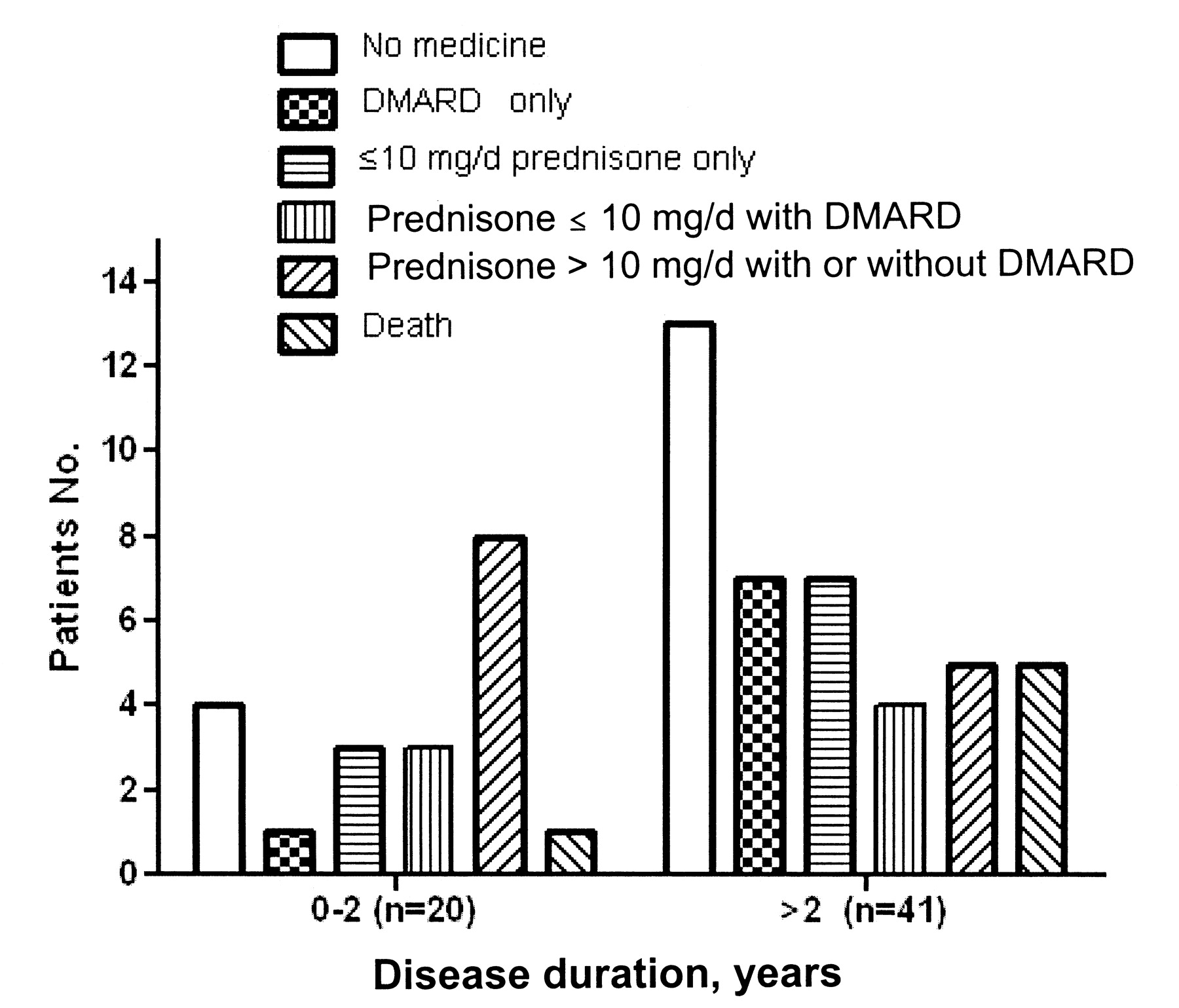
We also analyzed the medications based on the last followup; these are represented in Figure 2. Sixty-one patients were divided into 2 groups based on the duration of the disease, i.e., < 2 years (n = 20) and ≥ 2 years (n = 41). The medications were analyzed as follows: no medicine; DMARD only; ≤ 10 mg/day prednisone only; ≤ 10 mg/day prednisone with DMARD; > 10 mg/day prednisone with/without DMARD; and death.

{kind=link}
{kind=link}
Medications based on last followup of the 61 patients with AOSD charted by disease duration: < 2 and ≥ 2 years.
Interestingly, 20.0% of patients with < 2 years’ and 31.7% with ≥ 2 years’ disease duration were in drug-free remission.
Prognosis
Based on the disease course, we divided the 61 patients into 2 groups: those with favorable outcome (n = 45) and unfavorable outcome (n = 16). Subsequently, we analyzed prognostic factors for the 2 groups (Table 4), and found that pleuritis, interstitial pneumonia, elevated ferritin levels, and failure of fever to subside after 3 days of prednisolone at 1 mg/kg/day were unfavorable prognostic factors for patients with AOSD.
Prognostic factors for unfavorable outcome of 61 AOSD cases.
DISCUSSION
We describe a series of 61 patients with AOSD and compare the clinical and laboratory features observed in our series with previous reports. Although AOSD is prevalent worldwide4–20, some visible differences are noted. Persistent fever, evanescent rash, arthritis, and sore throat were the most prevalent symptoms in our series, similar to other reports presented in Table 1 and the report from Hong Kong9. The incidences of myalgia, hepatomegaly, pericarditis, pleuritis, and weight loss were lower than those reported in Caucasian cohorts6. This difference could be attributed to racial differences or the different diagnostic criteria used in each study.
Leukocytosis and elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels were the most outstanding laboratory findings of acute-phase AOSD. The frequency of liver dysfunction was lower in our series than in other series4–19.
Treatment of AOSD is exclusively empirical: NSAID, steroids, DMARD, and biologic agents are used to control fever, arthritis, and systemic diseases27. With the exception of 2 patients who responded to NSAID and MTX, almost all patients required steroids. MTX, chloroquine, thalidomide, and leflunomide were also used for controlling the disease activity of AOSD. We also analyzed the medications based on different disease durations at last visit. It is notable that 20.0% and 31.7% of patients having < 2 years’ and ≥ 2 years’ disease duration, respectively, were in drug-free remission. Roughly 40% of the patients required > 10 mg/day prednisone with or without DMARD to control their disease for the initial 2 years, while 12.2% of patients with ≥ 2 years’ disease duration needed the above-mentioned therapy. The proportion of patients requiring high-dose prednisone decreased with the increase in disease duration. About half of our patients required low dosage prednisone ≤ 10 mg/day only, DMARD only, or both to control disease activity. This result is consistent with some reports in which about one-third to three-quarters of patients attained complete disease remission after 1 or several episodes; most of these patients were free of disease for a long time under medication with low-dose prednisone or MTX or even with no medication28.
The mortality rate in our series (10%) was higher than that in other reports. Four patients died of infection, with persistent fever, cough, and expectoration during the hospital stay. Sputum cultures and CT scans indicated pulmonary infection. Severe pneumonia and respiratory failure were the main causes of death. As well, 1 patient died of liver failure and 1 of hemophagocytic syndrome.
It would be valuable to determinine the prognostic risk factors of AOSD. However, the literature regarding the predictors of outcome is limited. Still’s rash, polyarthritis, and root-joint arthritis were reported to be significantly associated with an unfavorable outcome4,6. In our study, analyzing the prognostic risk factors of 61 patients with AOSD, we found that interstitial pneumonia, pneumonia, elevated ferritin levels, and failure of fever to subside after 3 days of prednisolone 1 mg/kg/day were unfavorable prognostic factors. Still’s rash, polyarthritis, and root-joint arthritis were not observed to be significantly associated with unfavorable outcome in our study.
AOSD is a rare, poorly understood, systemic inflammatory disease; patients in different ethnic groups can present with variable clinical features and laboratory findings. Although the prognosis of AOSD is generally favorable, some studies, including ours, reveal that death may be caused in some patients due to overwhelming infection, hepatic failure, amyloidosis, adult respiratory distress syndrome, heart failure, and macrophage activation syndrome4,23–25. With regard to patients who are refractory to corticosteroids, combined immunosuppressive agents are usually recommended29–31. It is notable that biologic agents, including anakinra, infliximab, tocilizumab, etanercept, and rituximab, have displayed promising efficacy in refractory AOSD32–37. The prognosis of AOSD could be further improved by therapy with these emerging interventions.
Footnotes
-
Supported by research grants 30772009, 07JC14070, and T0203 from the National Natural Science Foundation of China and Shanghai Science and Technical Committee.
- Accepted for publication November 27, 2008.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.