

Abstract
Objective. To assess the efficacy and safety of gout-specific medications in gout patients with a comorbidity and/or comedication.
Methods. A systematic literature search for gout, its medication, and the most common comorbidities and comedications, using serum uric acid (SUA) levels as the primary, and adverse events as the secondary outcomes.
Results. Eight trials met inclusion criteria. Trials covered treatment with allopurinol, benzbromarone, rasburicase, or febuxostat in a gout population with mild or moderate renal insufficiency. High risk of bias (5/8 trials) and heterogeneity precluded formal metaanalysis. The trials showed the following hierarchy in efficacy (lowering the SUA below 6.0 mg/dl): febuxostat 80 mg (44%–71%) > febuxostat 40 mg (43%–52%) > allopurinol 100 mg or 200 mg (0–46%) after 6 months of therapy; rasburicase (46%) > allopurinol 300 mg (16%) after 7 days of therapy; benzbromarone 100–200 mg (93%) > allopurinol 100–200 mg (63%) after 9–24 months of therapy. The combination of allopurinol and benzbromarone seemed to be effective, with a significant reduction in the SUA from 7.8 to 5.7 mg/dl (p < 0.05) after 1 month. One study showed that 89% achieved the target SUA using higher doses of allopurinol than usually recommended for patients with renal impairment without an apparent increase in adverse events. In addition, allopurinol and benzbromarone significantly improved renal function.
Conclusion. In gout patients with renal insufficiency febuxostat, rasburicase, benzbromarone, and allopurinol + benzbromarone seemed to be effective and safe; allopurinol may be cautiously titrated until the target uric acid level has been reached, and may improve renal function.
Gout is among the most common causes of inflammatory arthritis in most industrialized countries1. Gout is a disorder of purine metabolism that results from urate crystal depositions. Uric acid-lowering therapy is advised when there are recurrent attacks, tophaceous disease, or polyarticular disease.
The complexity of gout is often underestimated. One aspect of the complexity is that patients with gout often experience high rates of comorbidities, raising many challenges2,3. A recent study by Phillinger, et al showed that gout patients on average have 4 comorbidities, and 5%–10% of the patients have 7 or more comorbidities4. The most common comorbidities are hypertension, lipid disorders, and diabetes mellitus2,5. The most commonly used comedications are antihypertensive drugs, statins, and nonsteroidal antiinflammatory drugs (NSAID)2. These comorbidities and comedications in many patients pose challenges to the management of gout.
Common treatments for acute gout are colchicine, NSAID, corticosteroids, and interleukin 1 (IL-1) inhibitors. Common uric acid-lowering therapies include allopurinol, benzbromarone, probenecid, and febuxostat. Less common uric acid-lowering drugs are rasburicase, pegloticase, and sulfinpyrazone.
This article is part of the 3e (Evidence, Expertise, Exchange) Initiative on Diagnosis and Management of Gout6. The objective of the current work was to systematically review the available literature concerning 1 of 10 selected questions as an evidence base for generating the recommendations. The question was: How do common comorbidities (such as metabolic syndrome, cardiovascular, gastrointestinal, and renal disease) influence the choice of gout-specific drugs (such as colchicine, allopurinol, and other urate-lowering therapies) in an acute gout flare, in gout, and in prophylaxis of an acute flare?
MATERIALS AND METHODS
This systematic review used the methodology proposed by the Cochrane Collaboration.
The clinical question, as formulated by the group of clinicians, was first rephrased in epidemiological terms: What is the efficacy and safety of gout-specific drugs in gout patients with at least 1 of the following comorbidities or comedications: renal disease, hematologic malignancy, ischemic heart disease, cardiac failure, hypertension, dyspepsia, ulcer-related disorders, metabolic syndrome, and diabetes mellitus? Comedication may relate to the use of aspirin, statins, coumarins, diuretics, azathioprine, or 6-mercaptopurine, and many other agents; for this reason we rephrased this part of the question to “gout patients, in whom an interaction of medications may be present.” We then structured the search details according to the PICO format (Patients, Interventions, Comparisons and Outcomes7). Patients were defined as adults at least 18 years of age with gout and at least 1 of the defined comorbidities or comedications. The intervention was defined as gout-specific drugs (colchicine, IL-1 inhibitor, allopurinol, benzbromarone, probenecid, febuxostat, rasburicase, pegloticase, and sulfinpyrazone). The comparator was defined as a patient with gout with no comorbidity or comedication. The outcomes were divided into efficacy and safety according to the guidelines for outcome measurement in gout for acute and chronic gout as decided by OMERACT (Outcome Measures in Rheumatology)8.
The types of studies considered for inclusion were randomized controlled trials (RCT) and quasirandomized controlled trials (CCT; i.e., where allocation was not truly at random), cohort studies, and case series with more than 20 patients. The Website of the US Food and Drug Administration and European Medicines Agency were also searched. There was a restriction for language, defined as languages spoken by 1 of the 3e international members (English, German, Dutch, French, Spanish). Only trials that were published as full text or were available as a full trial report were included.
Search strategy
The following computerized bibliographical databases were searched: Medline (1948 to October 2011), Embase (Embase classic 1947 to 1979 and Embase 1980 to October 2011), The Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library Issue 2, 2010) without language restrictions, using the highly sensitive Cochrane Collaboration search strategy, which aims to identify all RCT9. Specific MeSH (US National Library of Medicine) subject headings and additional keywords for gout, gout-specific drugs, defined comorbidities, and interaction terms were used to identify all relevant trials, observational studies, and case series. We addressed comedication by using interaction terms such as “synergism,” “antagonism,” “contraindication,” or similar, instead of all possible substance names, to keep the search strategy practical. References from all relevant articles found in the search were screened to identify additional studies. Finally, conference proceedings for the American College of Rheumatology (ACR) and the European League Against Rheumatism for 2010 and 2011 were also hand-searched to identify unpublished studies. The complete search strategy is provided online as part of supplementary material, available from www.3egout.com
Selection of studies, data extraction, and assessment of risk of bias
Two reviewers (IvE, CvD) independently assessed each title and abstract for suitability for inclusion in the review, according to predetermined selection criteria, followed by full-text article review where necessary. For included trials, they independently extracted data regarding study design, study duration, characteristics of study population, interventions, outcome measures, and timing of outcome assessment, cointerventions, adverse effects, and loss to followup using a standardized data extraction form.
In order to assess efficacy, raw data for outcomes of interest (means and standard deviations for continuous outcomes and number of events for dichotomous outcomes), as well as number of participants, were extracted if available from the published reports.
To assess the risk of bias we used the Cochrane tool for RCT10, which includes the following items: random sequence generation; allocation concealment; blinding of participants, care provider, and outcome assessor for each outcome measure; incomplete outcome data; selective outcome reporting; and other potential sources of bias; each criterion was rated as “Yes” (low risk of bias), “No” (high risk of bias), or “Unclear” (either lack of information or uncertainty over potential for bias). For all these steps, disagreements among reviewers were discussed and resolved in a consensus meeting or involving a third reviewer (RL), if necessary. For cohort and case-controlled studies we used the Hayden tool11, and for the retrospective cohort studies, the Newcastle Ottawa scale12.
Data analysis
In cases where individuals were missing from the reported results, we assumed the missing values to have a poor outcome. For dichotomous outcomes (e.g., number of withdrawals due to adverse events), the withdrawal rate was calculated using the number of patients randomized in the group as the denominator (worst-case scenario).
The results of each trial were planned to be plotted as point estimates with 95% confidence intervals. Point estimates were planned to be measured as relative risk for dichotomous outcomes, and mean difference and standard deviation for continuous outcomes. If data obtained had a sufficient level of clinical and statistical homogeneity, we planned to pool the results using a fixed-effects model, and in case of clinical homogeneity but statistical heterogeneity, a random-effects model. Subgroup and sensitivity analyses were planned to assess the effects of several variables on the efficacy of combination therapy and to explore the robustness of the conclusions, respectively.
RESULTS
Results of the search
The electronic database search yielded a total of 5644 articles, and an additional 67 meeting abstracts were obtained from the conference proceedings. After removal of duplicates and screening of titles and abstracts, 5530 full studies and 66 meeting abstracts were excluded. During detailed review of the 114 full articles most studies were excluded because of wrong population, wrong design, or wrong outcome, leaving 7 articles in the end. One article was included after hand search. Together with the single remaining abstract, a total of 9 articles were included (Figure 1). Among these, 1 article was a subgroup analysis of another article, resulting in a final number of 8 distinct studies.

Procedure of the systematic literature reviews.
Included studies
We included 5 RCT, 1 CCT, 1 observational retrospective study, and 1 observational prospective cohort study. Six smaller studies included a total of 395 patients; in the larger studies of Becker, et al13 (n = 2269) and Schumacher, et al14 (n = 1072) the subgroups of patients with renal impairment were 1483 and 40, respectively. All articles were in English, and had been published between 1991 and 2011.
The 8 included articles were all very heterogeneous, impeding pooling of their results. They included studies of allopurinol, benzbromarone, rasburicase, and febuxostat in patients with renal impairment or renal insufficiency. All studies were done in patients with mild to moderate renal impairment (creatinine clearance > 30 ml/min), except 2 studies of De Angelis and Hosoya15,16 that included a small subgroup of patients with severe renal insufficiency (creatinine clearance < 30 ml/min). Six trials compared a specific medication between a population with and one without renal impairment13,14,16,17,18,19. Two trials compared 2 different medications in patients with renal impairment15,20.
All studies included patients with gout as defined by the ACR criteria or the clinical specialist. The most commonly used outcomes were SUA or percentage of patients with SUA < 6.0 ml/dl and adverse events. Three studies included serum creatinine as outcome17,18,20.
In all the trials that included patients with renal impairment allopurinol dose was adjusted to renal function as suggested by Hande in 198421 (see Appendix 2 in online supplementary data, available from www.3egout.com).
Risk of bias in included studies
Five of the 8 included studies were considered to be at high risk of bias, 1 at low risk, 1 at moderate risk, and 1 at unclear risk of bias.
The main issues were inadequate (4 trials) or unclear (2 trials) sequence generation method; inadequate (4 trials) or unclear (2 trials) allocation concealment; and high (7 trials) risk of attrition bias.
Comparative efficacy and safety
Due to multiple sources of heterogeneity, a metaanalysis could not be performed and we present a summary of pertinent findings from the individual trials.
Febuxostat versus allopurinol versus placebo in a renal-impaired population
In their trial, Schumacher, et al reported a higher percentage of patients reaching SUA level < 6 mg/dl with febuxostat 80 mg than with allopurinol 100 mg in a population with impaired renal function [serum creatinine levels 132–170 mmol/l (= 1.5–2.0 mg/dl), 44% vs 0%]. With allopurinol 100 mg or placebo, no patients with an impaired renal function reached the target SUA < 6.0 mg/dl compared to 23% of patients with normal renal function14. For all doses of febuxostat the effect in reducing SUA was only slightly lower in patients with impairment of renal function (Figure 2).

Efficacy of febuxostat 240 mg, febuxostat 120 mg, febuxostat 80 mg, allopurinol 100–300 mg, and placebo in reducing the serum uric acid (SUA) below 6.0 mg/dl in a population with impaired renal function14.
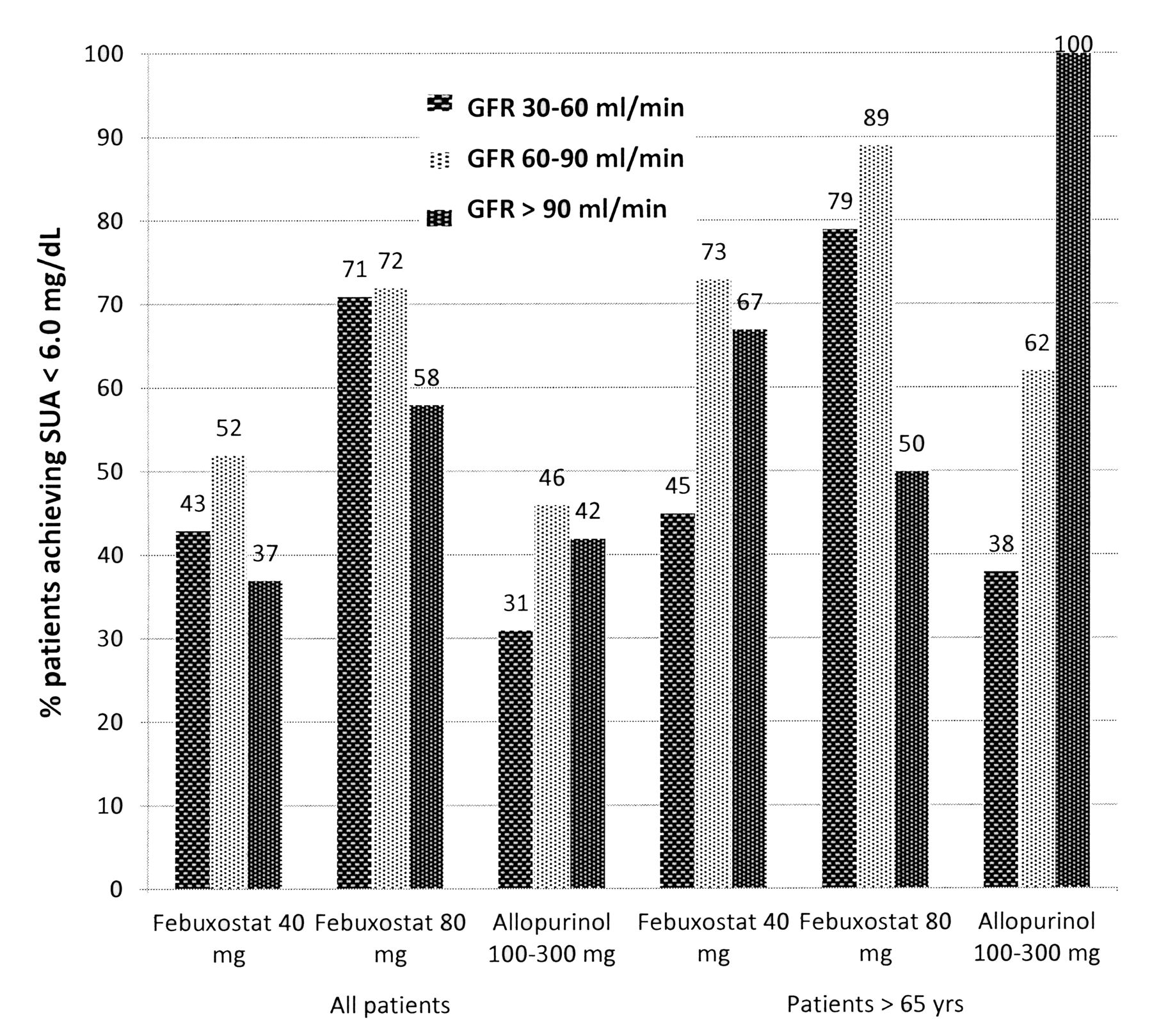
In the trial by Becker, et al studying patients with mild and moderate renal insufficiency (estimated creatinine clearance of 60–90 ml/min or 30–60 ml/min, respectively), febuxostat 80 mg was more effective in reaching SUA < 6.0 mg/dl than febuxostat 40 mg (72% vs 52% in mild insufficiency, and 71% vs 43% in moderate insufficiency), and febuxostat 40 mg was more effective than allopurinol 100–300 mg per day (52% vs 46% and 43% vs 31%)13. Interestingly, in a small subgroup analysis of patients aged > 65 years who had several comorbidities and mild-to-moderate renal impairment, allopurinol and febuxostat were at least as effective in lowering SUA as in the patient group of all ages and mild to moderate renal impairment (Figure 3).
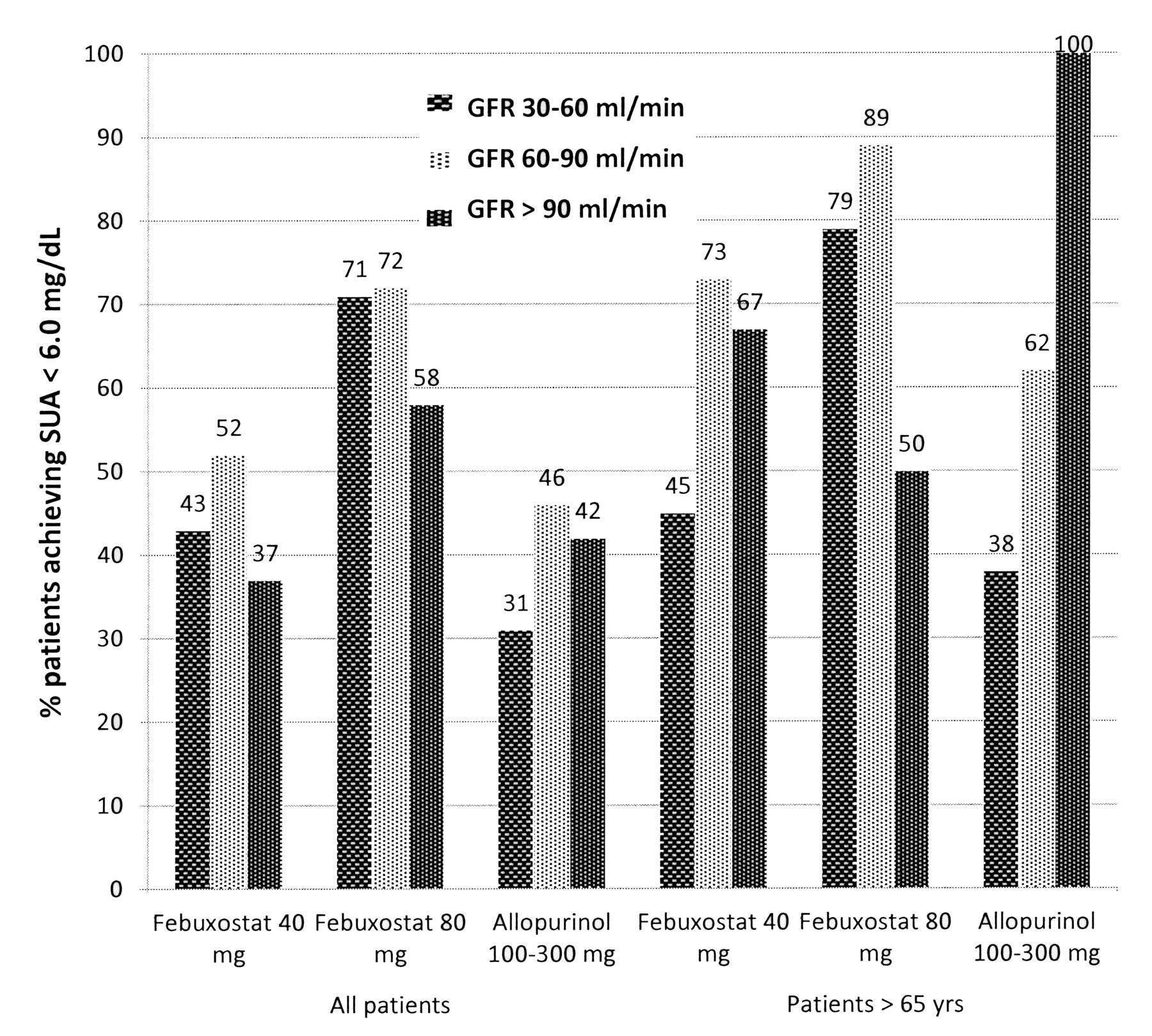
Efficacy of febuxostat 80 mg, febuxostat 40 mg, and allopurinol 100–300 mg in reducing the serum uric acid to < 6.0 mg/dl in a population with normal renal function (GFR > 90 ml/min), mild renal impairment (GFR 60–90 ml/min), and moderate renal impairment (GFR 30–60 ml/min)13. GFR: glomerular filtration rate.
In both trials there were no differences in adverse events between the patient group with normal and those with impaired renal function. There were also no differences between the patient groups receiving febuxostat in different doses and allopurinol in different doses.
Rasburicase versus allopurinol in patients with renal impairment
Rasburicase 0.02 mg/kg/day during 3 to 7 days was more effective in lowering SUA after 7 days than allopurinol 300 mg (46% vs 16% reached a SUA < 5.5 mg/dl), although the renal function was much worse than in the allopurinol group [serum creatinine 398 μmol/l (4.5 mg/dl) vs 239 μmol/l (2.7 mg/dl)] and the baseline SUA much higher (10.7 mg/dl vs 7.6 mg/dl, respectively)15.
Allopurinol versus benzbromarone in a renal-impaired population
Perez-Ruiz, et al concluded that, in a population with moderate renal impairment (mean creatinine clearance 54 ml/min), benzbromarone titrated to effectiveness was more effective than a clearance-adjusted (reduced) dose of allopurinol (93% vs 63% of patients reached SUA < 6.0 mg/dl)20.
Allopurinol and benzbromarone in a renal impaired population
Allopurinol in combination with benzbromarone was effective in lowering the SUA in a population with mild renal impairment (mean estimated creatinine clearance 47 ml/min, SUA 7.8 mg/dl → 5.7 mg/dl). The combination of allopurinol and benzbromarone had no significant effect in cases of renal failure when estimated creatinine clearance was < 30 ml/min (SUA 9.8 mg/dl → 8.2 mg/dl)16.
Effects of allopurinol and benzbromarone on renal function
Two trials investigated changes in creatinine clearance in patients with renal impairment. One trial found improvement in renal function in patients with mild renal impairment after 2 years with allopurinol 200 mg (baseline creatinine clearance of 73 improved to 80 ml/min) and benzbromarone 50 mg (78 ml/min → 88 ml/min). In patients with moderate renal impairment there was also improvement of renal function with allopurinol 200 mg (49 ml/min → 77 ml/min) and benzbromarone 50 mg (53 ml/min → 88 ml/min)17. This effect was more pronounced in patients with more severe impairment of renal function, while it was not significant in normal renal function. The other trial found a slight improvement, not statistically significant, of renal function after 2 years with allopurinol 100–300 mg (creatinine clearance 53 → 55 ml/min) and benzbromarone 100–200 mg (creatinine clearance 54 → 64 ml/min)20. Numerically, the effect of benzbromarone on creatinine clearance was slightly greater than the effect of allopurinol.
Allopurinol dosing in renal insufficiency
Two studies, a prospective cohort study and a retrospective cohort study18,19, have applied allopurinol dosages above the dose recommended by Hande in 198421 for a population with renal impairment. These studies show that, in the presence of close monitoring of liver function, renal function, and full blood count, higher than recommended doses of allopurinol can be employed. Both studies, however, were observational designs, and are therefore only hypothesis-generating.
Recommendations by the FDA and EMA (“grey literature”)
A hand search of sites of the US Food and Drug Administration and the European Medicines Agency22,23 revealed the following information.
Colchicine
Do not use P-glycoprotein (P-gp) or strong CYP3A4 inhibitors (clarithromycin, ketoconazole, grapefruit juice, etc) in patients with renal or hepatic impairment who are currently taking colchicine; consider a dose reduction or interruption of colchicine treatment in patients with normal renal and hepatic function if treatment with a P-gp inhibitor or a strong CYP3A4 inhibitor is required.
Anakinra
In patients with endstage renal disease dose must be tapered. In combination with tumor necrosis factor-α blockers the risk of infection is higher.
Febuxostat
Febuxostat in combination with azathioprine or mercaptopurine can increase plasma concentrations so it should not be prescribed.
Pegloticase
A higher risk for exacerbation of preexisting heart failure, so extra caution is necessary.
Allopurinol
Coadministration with cyclosporine needs possible dose adjustment and monitoring
DISCUSSION
Data to provide answers for the question posed in this systematic literature review were scarce and of poor methodological quality. From all comorbidities and possible comedications that one would expect in a patient with gout, only data for individuals with mild to moderate renal impairment were available. With these limited data and given the heterogeneity of the studies found, no general conclusions can be drawn, but several findings can be used for optimization of treatment in this specific population.
One finding was that allopurinol is likely frequently underdosed if adapted to the degree of renal impairment as suggested by Hande in 1984; moreover, titration of allopurinol based on efficacy, i.e., achievement of target uric acid levels, is more successful than applying a strict rule based on creatinine clearance or serum creatinine. The authors also concluded that such an approach was safe in the presence of adequate monitoring of complete blood count and liver and kidney function. Along these lines, it would be interesting to explore the effect of allopurinol in a dose higher than 100 mg compared to febuxostat, as current studies in the population of patients with impairment of renal function have concluded that febuxostat is more effective than allopurinol13,14. Although patients with mild to moderate renal impairment are frequently seen in clinical routine, and their treatment thus often constitutes a clinical challenge, it is important to realize that there are scarcely any data about patients with endstage renal disease. This makes it difficult to extend the conclusion to all patients with partial or complete renal dysfunction. This also applies to the finding of a potential renoprotective effect of allopurinol.
Conclusions for other comorbidities or comedications cannot be made since we found no data in the literature. The fact that there are hardly any data about gout-specific medication in people with comorbidities and comedications is a consequence of the standard design of clinical trials, which exclude patients with comorbidities — and thus likely also those with significant comedication. These trials often serve the purpose of establishing the efficacy of an investigational compound, and the interest in the specific real-life treatment challenges is usually not adequately addressed. In the recent past, the call for more pragmatic trials has increasingly been made14,24, and it gives rise to the hope that such studies will also reach the field of gout treatment or prevention. Particularly in this disease where the balance between the need for effective drugs on the one hand and the cautiousness about potential adverse events of drug treatment on the other might be more delicate than in other diseases.
More randomized controlled trials investigating the effects and safety of gout-specific medications in patients who also suffer additional metabolic problems or liver disease are needed to safely treat this highly prevalent disease in the complete clinical context.
In summary, with adequate monitoring for adverse events the dose of allopurinol may safely be titrated beyond currently recommended doses for impairment of renal function, until the target uric acid level has been reached. Febuxostat, rasburicase, benzbromarone, and the combination of allopurinol and benzbromarone all seem to be effective in gout patients with impairment of renal function. Allopurinol and benzbromarone may even contribute to improvement of renal function at the same time. There are currently insufficient data to draw further conclusions about the efficacy and safety of gout-specific medications in gout patients with other comorbidities or patients with comedication. Clearly, more evidence from well designed studies is needed and will be well received by the clinical community.
Footnotes
-
The authors acknowledge the work of all members of the 3e scientific committees and all participants in the national meetings. This article is derived from the 3e Gout program, which was sponsored by AbbVie Inc. Margaux Orange, Paris, France, provided logistical and administrative support for the 3e Gout meetings; this work was funded by AbbVie Inc. AbbVie employees were present during the 3e meetings, but did not influence the scientific discussions. AbbVie did not review the content or have influence on this report.








{kind=link}
{kind=link}
{kind=link}