

Abstract
As in many countries in Western Europe, in Italy tuberculosis (TB) is a relatively rare disease. In the last decade its incidence has remained constant at under 10 cases/100,000 inhabitants, the threshold considered to define a country as low prevalence. The epidemiological picture, however, is very different in the countries of Eastern Europe and in Africa, Asia, and Latin America, where the incidence of TB continues to increase and in some cases is accompanied by the emergence and spread of multidrug-resistant TB. The present review describes the epidemiology of TB in Italy. In 2008, the incidence rate was 3.8 cases per 100,000 for people born in Italy, and 50–60 cases per 100,000 for those born abroad. There was an increase in cases from Eastern Europe. The crude mortality rate for TB in 2006 was 0.7 deaths per 100,000 residents. Although TB is a low-prevalence disease in Italy, its epidemiology is changing. Since 1955, more than 160,000 people in Italy have died from this potentially preventable and curable disease.
The trend in the epidemiology of tuberculosis (TB) over the last 60 years can be described as follows: from 1950 to the early 1980s cases of TB slowly decreased and then remained steady for the last 20 years. Currently the rate of TB in Italy is low and most cases occur in groups at risk and in specific age groups. Multidrug-resistant cases are starting to be reported.
Italy is classified among the low-incidence countries for TB (fewer than 10 cases per 100,000 population) based on the number of reported cases: The incidence decreased from 7 cases per 100,000 population in 2007 to 5.8 per 100,000 population in 20111.
TB Incidence Rates by Sex and Age
The incidence rate by age is higher in males than in females, as is the case worldwide. The incidence rates of pulmonary TB and extrapulmonary TB showed the same trends in the period between 1995 and 2008: the rate of pulmonary TB decreased from 7 cases per 100,000 population in 1995 to 6 cases per 100,000 population in 2008; the rate of extrapulmonary TB decreased from 2.5 cases per 100,000 population in 1995 to 2 cases per 100,000 population in 20082 (Figure 1).
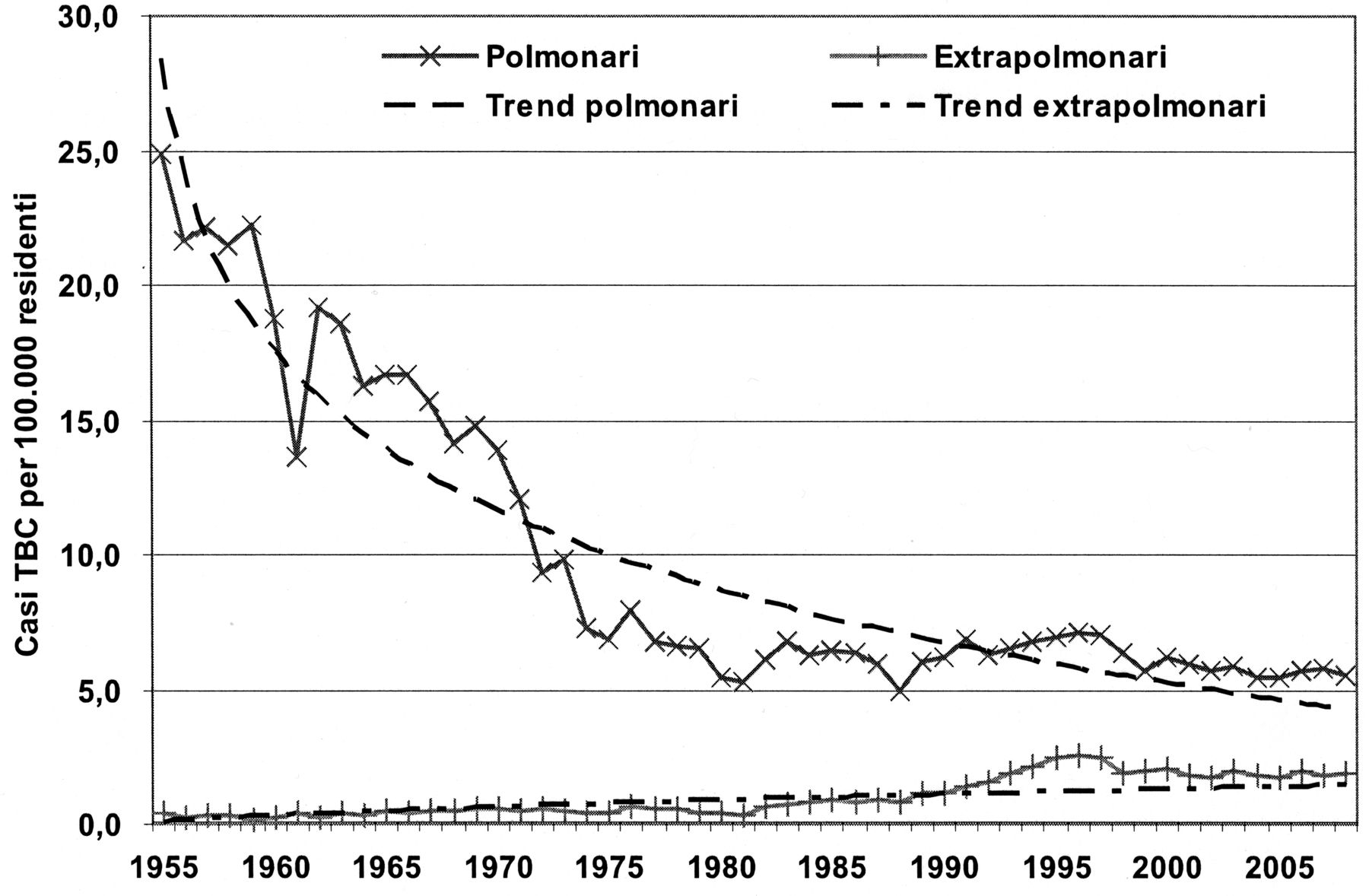
Incidence rates of pulmonary and extrapulmonary tuberculosis from 1995 to 2008, Italy2. Y axis: Cases of TB per 100,000 inhabitants. Polmonari: Pulmonary; Extrapolmonari: Extrapulmonary; Trend polmonari: Trend pulmonary; Trend extrapolmonari: Trend extrapulmonary. From the Italian Ministry of Health, Directorate-General of Prevention, Office V Communicable Diseases and Global Prophylaxis; with permission.
Over the period considered, an average of 72% of the cases of TB had a pulmonary localization; the proportion of extrapulmonary TB was 28% in 2008 instead of the 2% reported 50 years ago. The increase in extrapulmonary TB was probably due to a change in the TB surveillance system in Italy in the 1980s. From 1987 all different types of extrapulmonary TB had to be reported, not only the cases of contagious pulmonary TB, as happened previously. Further, since 1999 the TB surveillance system has included TB relapse, which accounted for 11% of all reported cases in the period between 1999 and 2008. The highest proportion of TB relapse was 13.4% reported in 2001; the percentage of relapse decreased to 9.2% in 20082.
Considering that 64% of cases of pulmonary TB are in males, the incidence rates are, respectively, 8 cases per 100,000 in the male population and 4 cases per 100,000 in the female population. The incidence rate of extrapulmonary TB by sex is the same in the 2 groups, amounting to 2 cases per 100,000 population2.
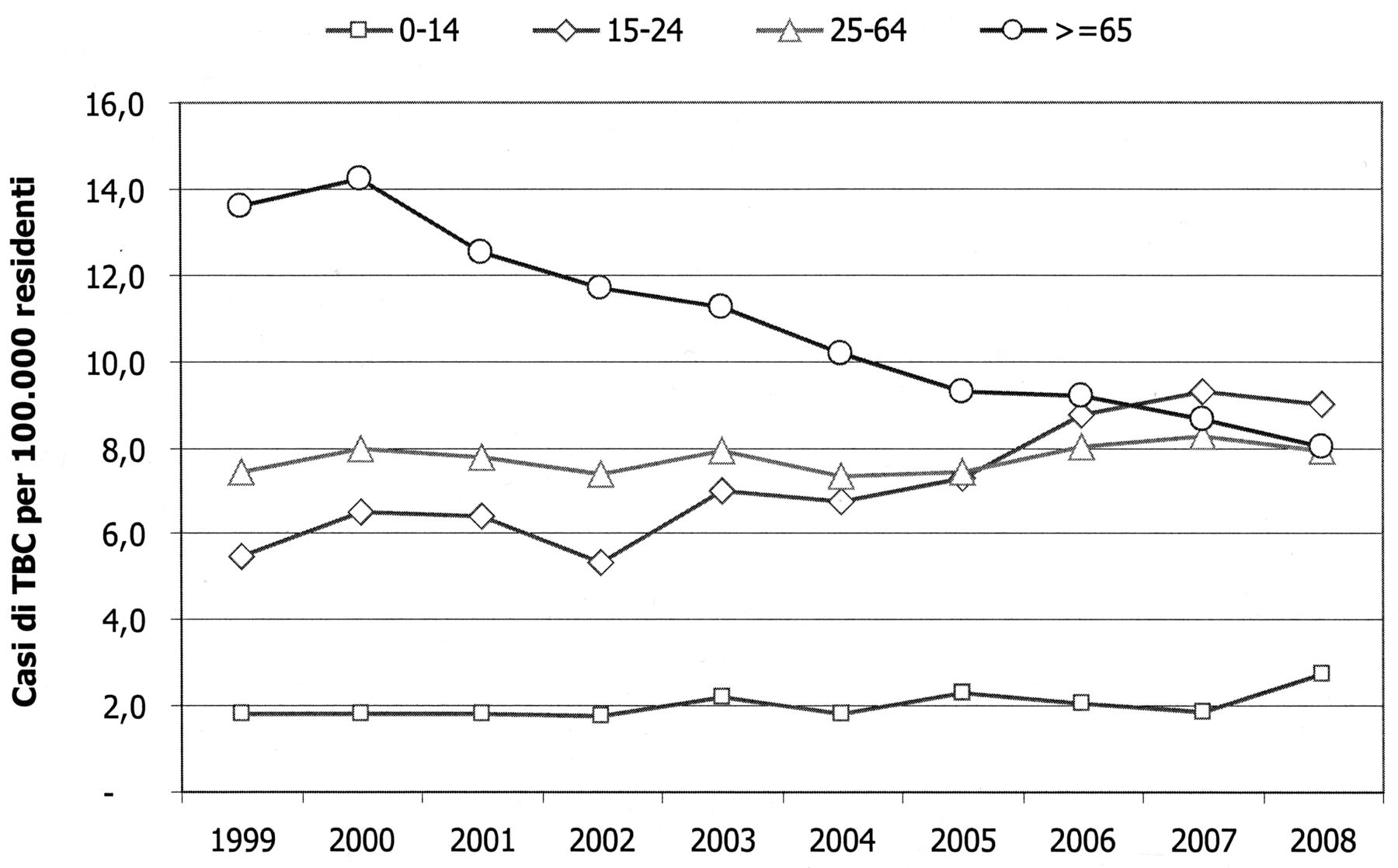
The incidence by age in the period 1999 to 2008 was highest among the older population but showed a decreasing trend (14 cases per 100,000 population in 1999 to 8 cases per 100,000 population in 2008). The average incidence rate was 11 cases per 100,000 in the population over 65 years old2. The incidence rate of TB among those 15 to 24 years old increased by 40% from 1999 to 2008 when it amounted to 9 cases per 100,000 population. A slight increase of incidence rate among the youngest age group (0 to 14 years) was also reported in 2008 (from 2 to 2.7 cases per 100,000 population; Figure 2)2.
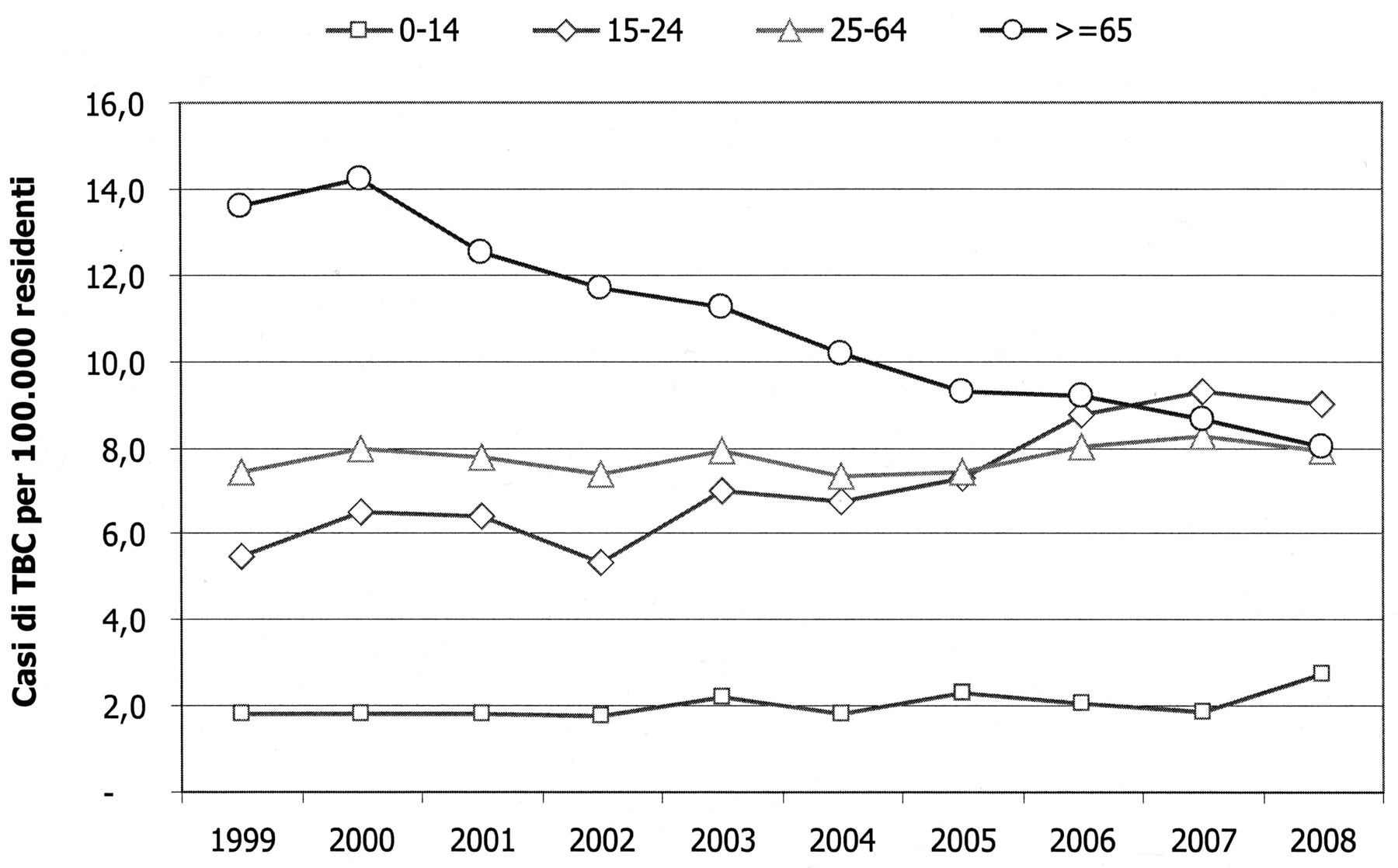
Incidence rate of tuberculosis (TB) by age group, 1999 to 2008, Italy2. Y axis: Cases of TB per 100,000 inhabitants. From the Italian Ministry of Health, Directorate-General of Prevention, Office V Communicable Diseases and Global Prophylaxis; with permission.
TB Incidence Rates by Geographic Area
An analysis of TB incidence over the decade from 1999 to 2008 in the different areas of the country shows a slight rise in the north of Italy, while the rate remained steady in the center and decreased in southern Italy and the Islands (Figure 3). More than half of all cases (59%) were reported in northern Italy, with an average incidence over the decade of 10.2 cases per 100,000 population and 11.4 in 2008; 24% of the cases reported occurred in inhabitants of the center of Italy with an average incidence over the decade of 9.5 cases per 100,000 population and 9.2 in 2008. Seventeen percent of cases were reported in southern Italy (15%) and the Islands (2%) with an average incidence over the decade of 3.8 cases per 100,000 population and 2.6 in 2008 in the southern regions and an average incidence over the decade of 3.2 cases per 100,000 population and 1.3 in 2008 in the Islands.
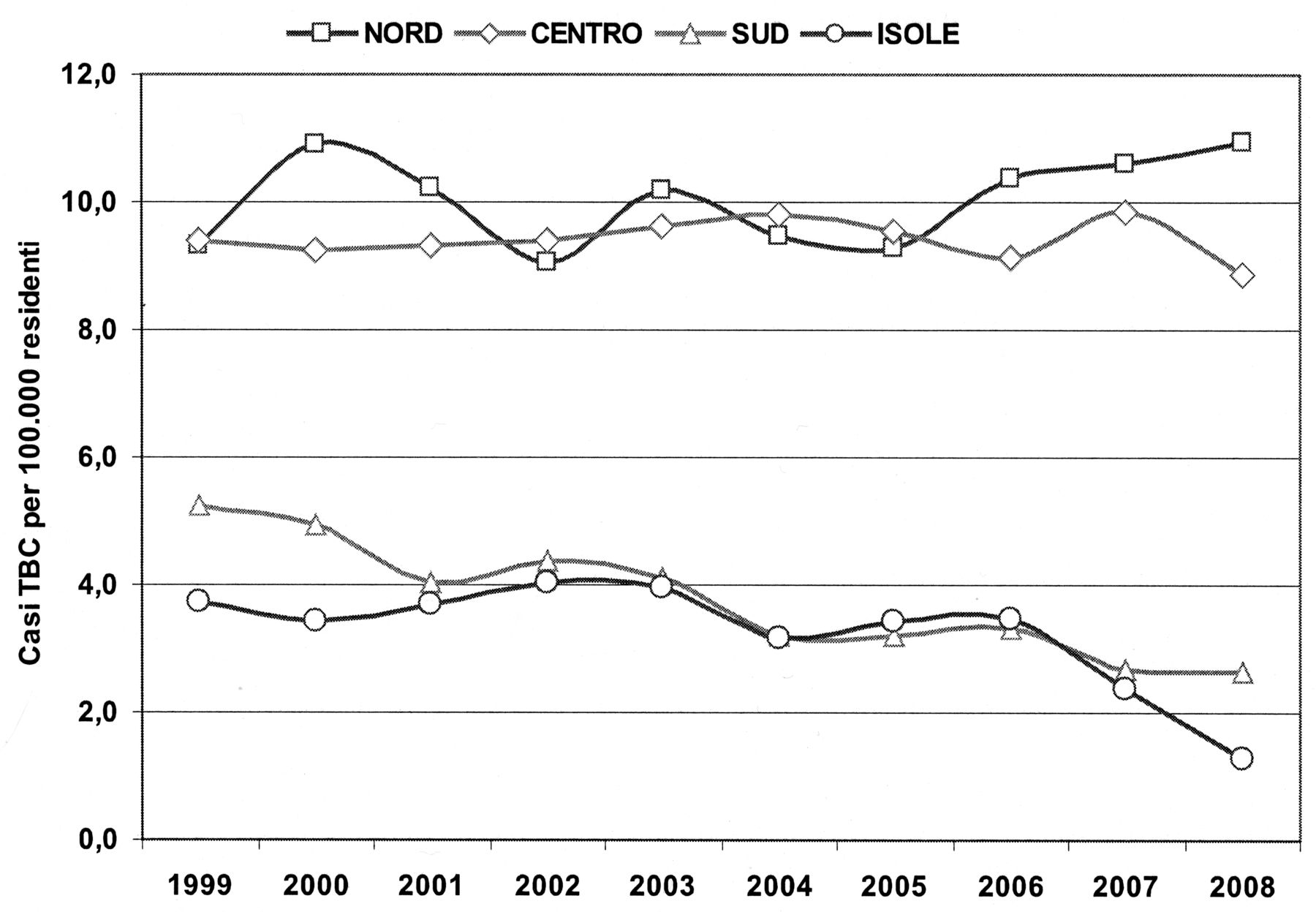
Incidence rate of tuberculosis for geographical areas from 1999 to 2008, Italy2. Y axis: Cases of TB per 100,000 inhabitants. Nord: North; Centro: Center; Sud: south; Isole: islands. From the Italian Ministry of Health, Directorate-General of Prevention, Office V Communicable Diseases and Global Prophylaxis; with permission.
According to these data almost 90% of all cases of TB reported in Italy occur in people living in the north and center of the country. In 2008 more than 70% of cases were reported in only 5 regions of the country: Lombardy (29%), Lazio (13%), Veneto (12%), Emilia-Romagna (11%), and Piedmont (9%). In 2008 the highest incidence rate was in Lombardy (more than 13 cases per 100,000), followed by Emilia-Romagna (11.4 cases per 100,000), and Veneto and the Autonomous Province of Bolzano (10.7 cases per 100,000)2.
The incidence rate is highest among those 15 to 24 years old in the north and center of the country (respectively, 14.7 and 13.4 cases per 100,000 population) and among those 25 to 64 years old in the south (3.1 cases per 100,000 population); in the Islands it holds steady (about 1 case per 100,000 population).
Immigrants
Overall, 36.5% of reported cases of TB in Italy occurred in foreign-born people. This proportion increased from 22% in 1999 to 46% in 2008. In 2008, 2026 cases were reported in foreign-born people compared to 2102 cases among Italian people (for 290 cases the country of origin was unknown; 6.6% of all cases)2.
Specific incidence rates relating to foreigners living in the country were higher than in the Italian population, even if they show a decreasing trend. The reported values do not include data from undocumented immigrants so it is not possible to calculate the real denominator. In fact, using estimates of all foreigners living in the country and living in each region as the denominator, TB incidence rates seem to be high in most regions but characterized by very variable CI, because of the different population sizes. In Lombardy, Lazio, and the Veneto regions the lower CI limit is more than 50 cases per 100,000 immigrants. In those regions where the presence of foreigners is limited (e.g., Basilicata and Valle d’Aosta), larger CI were reported, and the TB incidence rates in foreigners are therefore uninformative.
The CI of the incidence rates of TB in the 2007 Italian population were lower than 10 cases per 100,000 residents3. In Lazio, Veneto, and Emilia-Romagna the CI lower incidence was always higher than 7 per 100,000 Italians4. Even among foreign-born citizens, most cases of TB occur in males (about 60%). Considering the distribution by age and nationality of reported cases, most cases occur among foreign-born persons in the 25- to 34-year-old group, which is the most represented group among foreign-born citizens. In 2008, in both the 25- to 64-year-old and the 15- to 24-year-old groups, the number of TB cases among foreigners was higher than among Italians. For the group aged 65 years and over, more than 90% of all reported cases were observed in the Italian population2.
Most of the foreign-born citizens who develop TB come from Africa (35% of cases), followed by Europe and Asia. The country of origin of the highest number of cases was Romania (505 cases), followed by Morocco, Senegal, Peru, Pakistan, and India2 (Figure 4). The distribution by sex of foreign-born cases showed that the incidence was higher among males from all countries with the exception of Peru, where females are more frequently affected by the disease. This variability in the absolute number of cases also clearly depends on the composition of the resident population. Worldwide data have shown that countries with TB incidence rates higher than 100 cases per 100,000 residents are the Horn of Africa (Ethiopia, Eritrea, Somalia), Senegal, Sudan, Ivory Coast, Nigeria, Peru, Bolivia, India, Pakistan, and Bangladesh. Comparing TB incidence rates reported by countries of origin, some discrepancies were found: the incidence rates are lower in Italy (a reduction of more than 100 cases per 100,000 for the Ivory Coast, Nigeria, the Philippines, Ghana, Bangladesh, Burkina Faso, and Republic of Moldova), with the exception of the Horn of Africa, Sudan, Bolivia, and Peru, where they are higher.

Number of cases of tuberculosis in foreign-born citizens by sex, 10 most frequent nationalities in 2008, Italy2. Cina Popolare: Peoples Republic of China; Filippine: Philippines. From the Italian Ministry of Health, Directorate-General of Prevention, Office V Communicable Diseases and Global Prophylaxis; with permission.
These discrepancies are due to the different composition of the various communities, the variable portion of undocumented residents, and various features such as social, economic, climatic, nutritional, and psychological factors that influence health and diagnosis and treatment of the disease. These factors help the spread of TB disease. Further, in more fragile communities with a low socioeconomic status level, the number of underestimated cases could be relevant.
Surveillance System and Antibiotic Resistance
In the period from 2004 to 2008, 30 mycobacteriology laboratories with high volumes of activity and homogeneously distributed throughout the country were recruited by the Italian National Institute of Health (ISS) to implement a surveillance system of national cases of TB resistant to standard antibiotic therapy. An external quality control program was implemented, based on sending strains of Mycobacterium tuberculosis with known resistance characteristics for the determination of sensitivity to isoniazid (INH), rifampicin (R), streptomycin (S) and ethambutol (E). The strains were derived from laboratory strains sent by the World Health Organization in Antwerp, Belgium.
The data collected were analyzed by the ISS and sent to the European Centre for Disease Prevention and Control (ECDC) from the Ministry of Health. It was seen that for the period 2004 to 2007, the percentage of monotherapy-resistant and multidrug-resistant cases of TB remained steady, being about 10% and 12%, respectively. In 2008, however, the value rose to more than 14% of cases of TB, with multidrug-resistant TB (resistant to at least INH and R) values increasing from 3% to 4% of all patients analyzed.
Data regarding the outcomes of monitoring TB treatment in the 2007 cohort were collected through the interregional coordination office of the TB-SORV, an Italian TB surveillance project, and were sent to the Ministry of Health5.
The protocol for monitoring outcomes of TB treatment, which is compatible with the specifications of the Euro-TB project, involves only the surveillance of outcomes for cases of pulmonary TB, as the only location or in combination with other sites. Only information about final outcomes were sent for each case that met the notification criteria. Only the regions of Emilia-Romagna, Friuli-Venezia-Giulia, Lombardy, Marche, Piedmont, Tuscany, and Veneto activated the surveillance system and sent information about the outcomes; 67% of cases of TB in Italy were reported in 2006 and 71% in 2007. Outcome data were analyzed both globally and for individual regions, then the regions with a level of coverage (number of outcomes received over the number of people with pulmonary TB reported in 2007) ≥ 85% or < 85% were lumped together6.
According to the definitions of the ECDC European Surveillance System, the data were further analyzed considering the different types of outcomes (cured, completed treatment, died, treatment failure, transferred, still in treatment, and terminated/not known) in 2 groups: positive outcomes (cured and treatment completed) and negative outcomes for potential treatment failure (all the rest).
Information about the outcomes was reported for 1818 of 2107 cases of pulmonary TB, with a total coverage of 86.3%2. In the regions that reached 85% coverage, the average percentage coverage was over 99%, while in all the other regions it was about 58%.
Overall, in 58% of cases the outcome was positive, in 29% negative, and in 13% was unknown. Among the cases with known outcome, in 67% of the cases the outcome was positive and in 33% it was negative.
Considering the regions with higher coverage, the percentage of positive outcomes was about 67%, even after leaving out unknown outcomes; in the regions with lower coverage, about 39% of outcomes were positive, but the percentage rose to 67% when unknown outcomes were left out. Negative outcomes in the 2 groups of regions were, respectively, 33%, even leaving out unknown outcomes, and about 19%, which rose to 85% leaving out unknown outcomes.
TB in People with AIDS
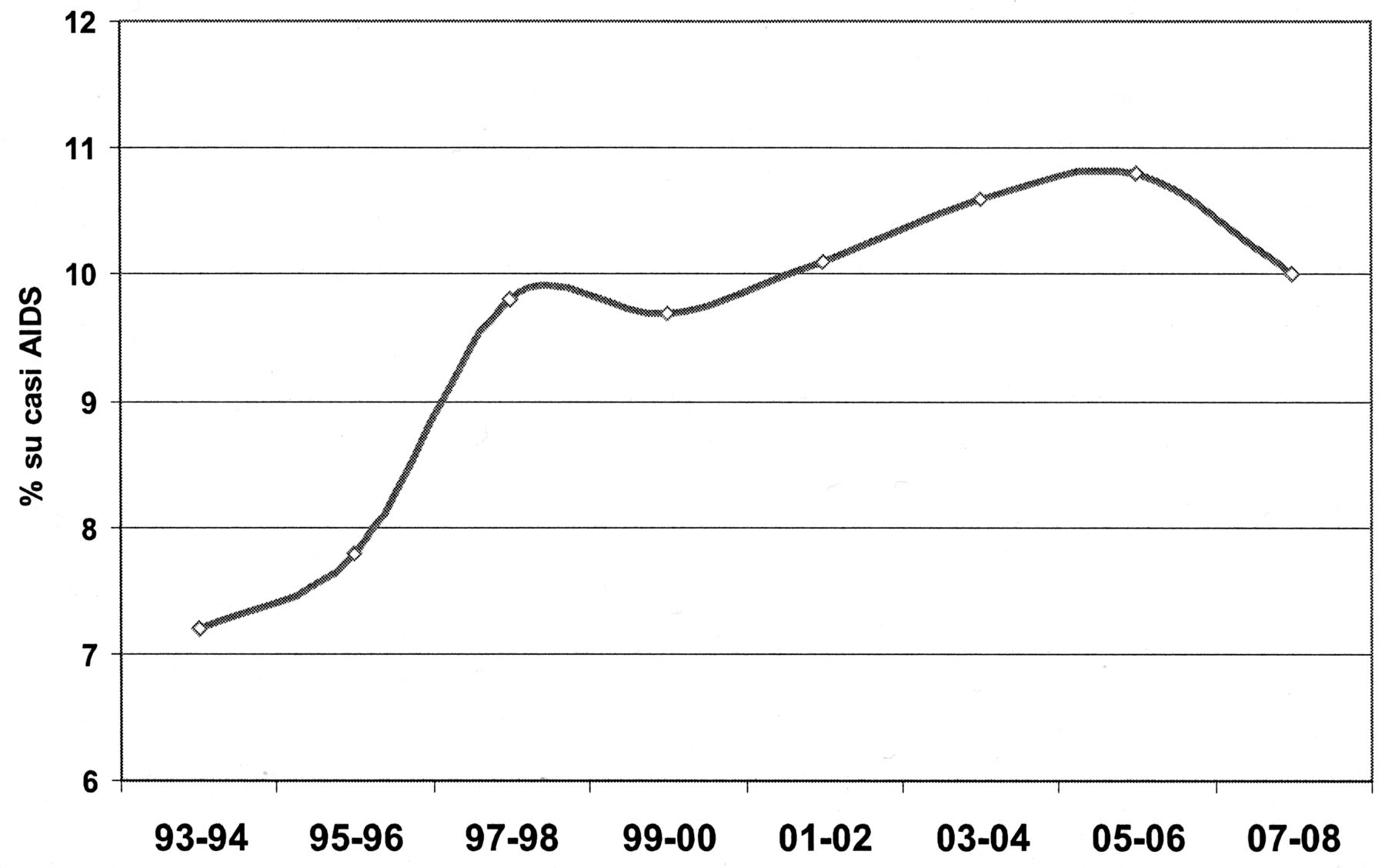
From 1993 to 2008, 3809 cases of AIDS (8.8% of a total of 43,134 cases of AIDS), initially diagnosed as TB cases, were reported to the AIDS Operational Centre. The average age of patients in the whole period was 36 years. Since 1997 there has been a very marked reduction in the number of AIDS cases because of the introduction of antiretroviral therapy, while the percentage of cases initially diagnosed as TB gradually increased from 7% in the 1990s to 10% in the first decade of the new millennium (Figure 5). The proportion of TB cases associated with AIDS has grown steadily to over 70% in males.

Percentage of tuberculosis cases in patients with AIDS, 1993 to 2008, Italy2. From the Italian Ministry of Health, Directorate-General of Prevention, Office V Communicable Diseases and Global Prophylaxis; with permission.
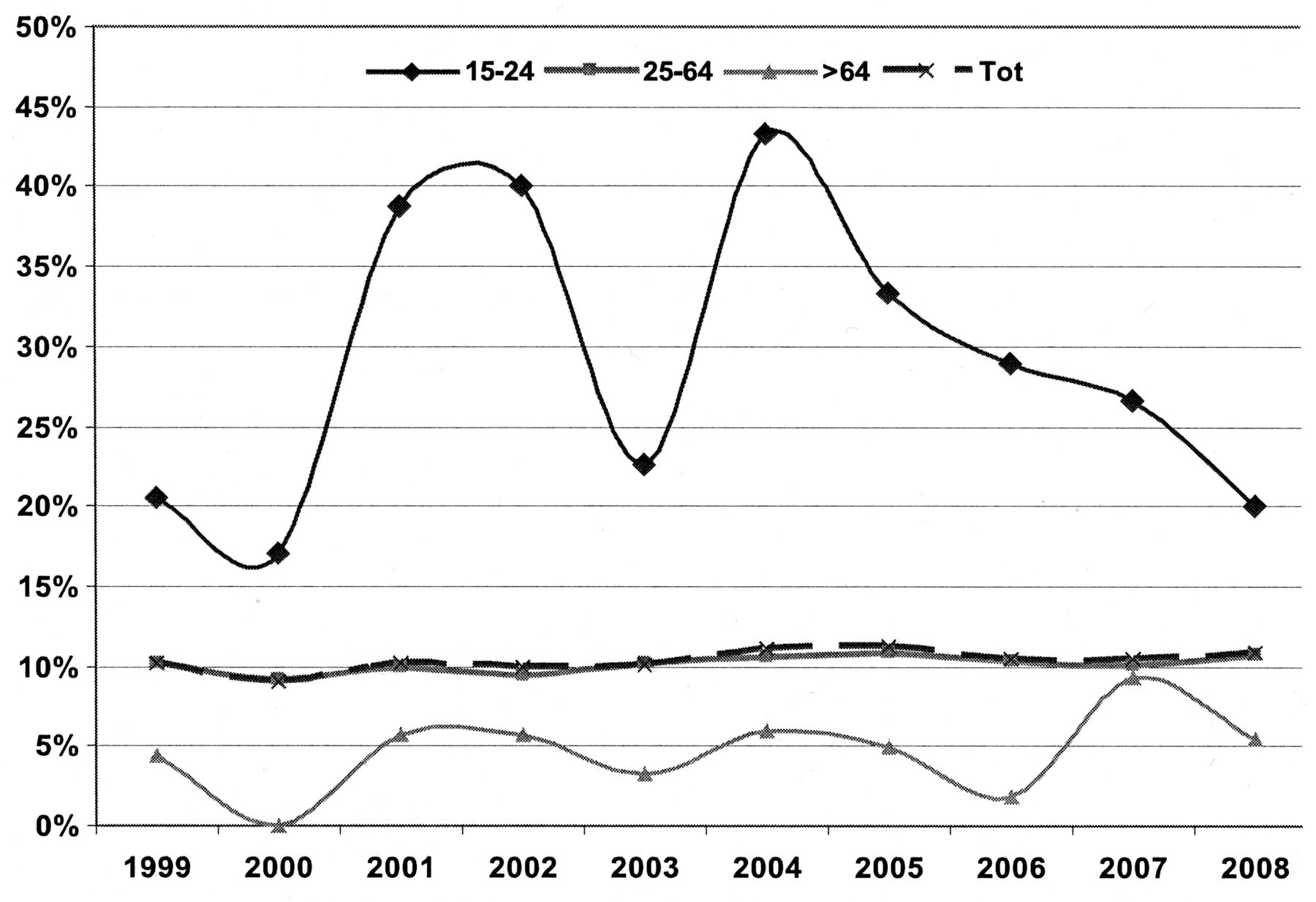
Considering TB cases among people with AIDS by age group, the percentage increased in the group under 25 years old, even if the absolute values were very low and the trend was, therefore, variable (Figure 6).
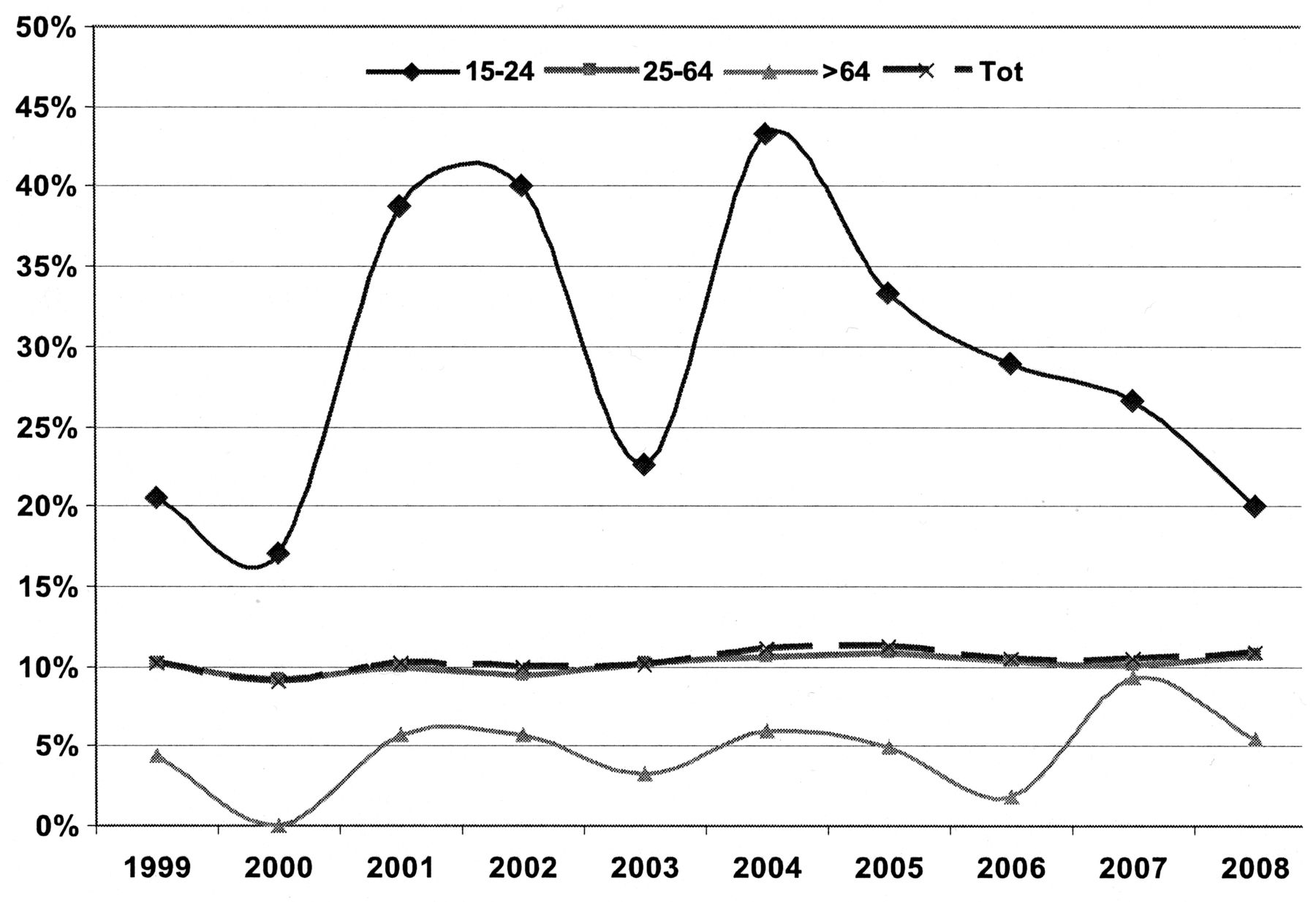
Tuberculosis trends (%) in AIDS cases by age group, Italy2. From the Italian Ministry of Health, Directorate-General of Prevention, Office V Communicable Diseases and Global Prophylaxis; with permission.
The number of AIDS-related TB cases in different regions shows important differences associated with the characteristics of the population. Most of the AIDS-related TB cases were reported in Lombardy (381) and Lazio (277), and these cases accounted for 38.4% of all cases in the last decade.
In the decade from 1999 to 2008 the total number of AIDS-related TB cases increased from about 80 to 98 cases in the foreign-born population and decreased from 139 to 38 cases in the Italian population. The incidence of AIDS-related TB cases by country of origin is very heterogeneous; in particular, a higher proportion of cases was reported in Africa and Central–South America while a lower proportion was reported in Eastern Europe and Asia.
Mortality
Over the period from 1955 to 2008, 160,000 deaths due to TB were reported. The crude mortality rate decreased from 22.5 per 100,000 in 1955 to 0.7 per 100,000 in 2006 (the average rate in Europe in the same year was 0.8 per 100,000 population)6.
Between 1955 and 2006, the average annual decrease was 6.1% (6.5% for males compared to 5.6% for females). Even if the difference between the annual rates in males and females is small, after 52 years the mortality rate by sex tends to be the same. In 1955, in fact, there were 7266 deaths in males and 3655 in females, while in 2006 there were 407 deaths: 222 in males and 185 in females. Males accounted for 72.9% of all TB deaths (range of variation between 77.8% and 54.5%, the latter value recorded in 2006; Figure 7).

Tuberculosis deaths: total cases and cases by sex from 1955 to 2006, Italy2. Maschi: Males; Femmine: Females; Totale decessi: Total deaths. From the Italian Ministry of Health, Directorate-General of Prevention, Office V Communicable Diseases and Global Prophylaxis; with permission.
Since 1969, TB mortality has steadily decreased and now involves adult and elderly people: 84.5% of deaths in 2006 occurred in people 65 years old or over and 18.9% in those 85 years old and over. In the same year, 3.5% of TB-related deaths occurred in the 25- to 44-year-old group, and 3 deaths (0.7%) were reported for TB in the under 15-year-old group, 2 of which were children2.
The epidemiology of TB in Italy has changed over the last 60 years. From 1950 to the early 1980s the prevalence decreased slowly and then remained steady, before a current new increase among some age groups. In absolute terms the rate of TB is low, and most of the cases occur in groups at risk and in specific age groups. Multidrug-resistant cases are beginning to be reported. Italy is classified among the low-incidence countries for TB (less than 10 cases per 100,000 population).
In Italy, as in the rest of the world, the incidence of TB is higher among males than females. In Italy the incidence is higher in elderly persons versus younger ones, but whereas the trend is decreasing in the former group, it is increasing in the latter. There are also some differences in incidence rates between different geographic areas of Italy. Over one-third of cases of TB in the country occurred in foreign-born people, with a strong increase in the number of such cases of TB in recent years. Considering the distribution of TB by age and nationality, in recent years in both 25- to 64-year-olds and 15- to 24-year-olds, the number of TB cases among foreigners was higher than among Italians. For the ≥ 65-year-old group, more than 90% of all reported cases were observed in the Italian population. One-third of foreign-born citizens with TB came from Africa.
Since 1997 there has been a very marked reduction in the number of AIDS cases as a result of the introduction of antiretroviral therapy, while the percentage of cases initially diagnosed as having TB gradually increased from 7% in the 1990s to 10% in the last decade. The proportion of TB cases associated with AIDS is steadily increasing.
The crude mortality rate from TB in Italy decreased from 22.5 per 100,000 in 1955 to 0.7 per 100,000 in 2006 (the average rate in Europe in the same year was of 0.8 per 100,000 population).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}