

Abstract
Objectives. To determine the efficacy and safety of antidepressants in pain management in patients with inflammatory arthritis (IA).
Methods. We searched the Cochrane Central Register of Controlled Trials, Medline, Embase, and PsychINFO for randomized controlled trials in adults with IA that compared any antidepressants (administered via any route) to another analgesic intervention or placebo. We also searched the 2008–2009 American College of Rheumatology and European League Against Rheumatism abstracts and performed a hand search of reference lists of relevant articles. Primary outcomes were patient-reported pain relief ≥ 30% and withdrawals due to adverse events. Two authors independently assessed methodological quality and extracted data. A risk of bias assessment was performed using methods recommended by the Cochrane Collaboration.
Results. Eight trials (652 participants) in patients with rheumatoid arthritis (RA) and 1 trial in patients with ankylosing spondylitis (100 participants) were included in this review. The majority of studies were published in the late 1980s in patients with active disease receiving minimal disease-modifying antirheumatic drug therapy. All trials evaluated tricyclic antidepressants (TCA) and 2 studies included a selective serotonin uptake inhibitor. Seven of the 9 trials had high risk of bias, 2 were unclear, and metaanalysis was not performed due to trial heterogeneity. RA trials with short-term outcome (< 1 week) found no significant benefit of amitriptyline 25 mg in combination with dextropropoxyphene (DXP) 65 mg over placebo, and inferiority of amitriptyline + DXP versus DXP 130 mg [mean difference (MD) 10.0, 95% CI 0.4 to 19.6]. There was conflicting evidence regarding medium (1–6 wks) or longer-term (> 6 wks) benefits on pain. One trial in depressed patients with RA showed no significant difference between amitriptyline and paroxetine given for 8 weeks (65% vs 56% much or very much improved; RR 1.2, 95% CI 0.9 to 1.5). One trial found that amitriptyline was no better than placebo in reducing pain in patients with active AS over 2 weeks (MD −0.2, 95% CI −1.2 to 0.8). From 5 trials, withdrawals due to adverse events were not significantly different from placebo. However, there were significantly more minor adverse events in patients receiving TCA compared with those receiving a placebo (RR 2.3, 95% CI 1.2 to 4.4). These included somnolence, dizziness, dry mouth, and nausea.
Conclusion. Based upon 9 trials of high or unclear risk of bias, it is not possible to draw firm conclusions about the efficacy of TCA as analgesics for patients with IA. The use of these agents may be associated with adverse events that are generally mild and do not lead to cessation of treatment. High-quality trials are needed in this area.
Despite the positive effects of biological therapies on the outlook for patients with inflammatory arthritis (IA), many patients continue to experience musculoskeletal pain1. Pain that is untreated and pain despite treatment are well known to negatively affect sleep, overall well-being, mood, and functional status2,3. With possible analgesic, sleep-promoting, and mood altering properties, antidepressants have been used to improve the symptoms and quality of life of patients with IA for over 50 years4. However, despite growing evidence of a benefit on pain in conditions such as fibromyalgia5, neuropathic pain6, and low back pain7, the evidence in IA remains less clear.
Classified by their structure and mechanism of action, antidepressants include the tricyclic antidepressants (TCA), monoamine oxidase inhibitors, selective serotonin reuptake inhibitors (SSRI), selective serotonin noradrenaline reuptake inhibitors, and norepinephrine reuptake inhibitors. Despite extraordinary advances in the understanding of pain pathways at the molecular level, the precise analgesic mechanisms of action of the antidepressants remain unclear. It is also debated whether any improvements in pain are independent of changes in mood. Evidence supporting this is that analgesia occurs more rapidly than any antidepressant effect, and at significantly lower doses8,9.
Antidepressants are known to cross the blood-brain barrier and exert central mechanisms of action that involve both spinal and supraspinal mechanisms10. They are also known to target serotonin and noradrenaline, which are key mediators of neural transmission. Other modes of action have been reported including a possible effect on opioid receptors11, blocking adenosine uptake10, ion channels12, and as antagonists of N-methyl-D-aspartic acid receptors13. Interestingly, there are also data suggesting that distinct peripheral analgesic mechanisms may be relevant in patients with IA14,15,16,17. However, their role as analgesics in patients with IA also remains controversial.
This article is part of the 3e (Evidence, Expertise, Exchange) Initiative on Pain Management by Pharmacotherapy in Inflammatory Arthritis18. The objective of this report was to systematically review the literature concerning one of the 10 selected questions as an evidence base for generating the recommendations: What is the effectiveness, safety, and role of antidepressants (muscle relaxants and neuromodulators) in inflammatory arthritis, and how should they be administered (i.e., interval, safety, and route)?”
This article is a modified version of a Cochrane Review that is specifically focused on rheumatoid arthritis19.
METHODS
We conducted a systematic literature review in several steps in accordance with the methods recommended by the Cochrane Collaboration20.
Rephrasing the research question
The clinical question posed by the expert clinicians was rephrased to enable epidemiological enquiry using the PICO (Patient, Intervention, Comparator, Outcome) method21. Patients were defined as adults with rheumatoid arthritis (RA), psoriatic arthritis, ankylosing spondylitis (AS), or spondyloarthritis. The intervention was defined as treatment with any formulation or dose of an antidepressant as either monotherapy or in combination. Comparators included placebo or any other pharmacological (excluding DMARD) or nonpharmacological analgesic modalities. The primary outcomes of interest were pain and withdrawals due to adverse events (AE), including mortality. The literature search was limited to randomized controlled trials (RCT), including trials where treatment was allocated via a quasi-random method.
Systematic literature search
A literature search for articles published between January 1950 and May 2010 was performed in Medline, Embase, and the Cochrane Central Register of Controlled Trials. The search strategy was developed in collaboration with an experienced librarian; for details see the online Appendix available from www.3epain.com. In addition, a search was conducted of abstracts from the European League Against Rheumatism (EULAR) and American College of Rheumatology (ACR) scientific meetings in 2008 and 2009. Review articles were also retrieved for identifying additional references via hand search.
Selection of articles
The titles and abstracts of all studies identified by the search strategy were screened, and all potentially eligible studies were reviewed in full text by 2 authors (BR and SW). Studies were excluded if they contained a mixed population where the data of those with IA could not be extracted separately, or if they were written in languages that could not be translated by one of the members of the 3e Initiative multinational panel. Drugs that had been withdrawn from the market due to safety concerns were excluded from the review. Any disagreement in study selection was resolved by consensus or by discussion with a third reviewer (RB).
Data extraction and quality appraisal
Raw data were extracted from the included studies by 2 authors (SW and BR), using predetermined forms. Differences in data extraction were resolved by referring to the original articles and establishing a consensus. A third reviewer (RB) was consulted to help resolve differences as necessary. Two authors (SW, BR) independently assessed risk of bias for all included studies for the following items: random sequence generation, allocation concealment, blinding of participants, care provider and outcome assessor for each outcome measure, incomplete outcome data, and other biases in accordance with the methods recommended by the Cochrane Collaboration20. To determine the risk of bias of a study, each criterion was rated as Yes (low risk of bias), No (high risk of bias), or Unclear (either lack of information or uncertainty over the potential for bias).
Data analysis
For continuous data, results were analyzed as mean differences (MD) between the intervention and comparator group with 95% confidence intervals. However, when different scales were used to measure the same conceptual outcome (e.g., pain), standardized mean differences (SMD) were calculated. For dichotomous data, a relative risk (RR) with corresponding 95% confidence intervals was calculated. In cases where individuals were missing from the reported results, we assumed the missing values to have a poor outcome. Prior to metaanalysis, we assessed studies for clinical homogeneity and where studies were sufficiently homogeneous that it was clinically meaningful for them to be pooled, a metaanalysis was performed using a random-effects model. Statistical heterogeneity was assessed using the I2 statistic22. In addition to the absolute and relative magnitude of effect, for dichotomous outcomes, the number needed to treat (NNT) to benefit or the number needed to treat to harm (NNTH) were calculated from the control group event rate and the relative risk using the Visual Rx NNT calculator (for details see: http://www.nntonline.net/visualrx/). Analysis was performed using Review Manager 5.
RESULTS
Study characteristics
A total of 487 references were identified with the systematic search strategy. After title and abstract screening, 35 articles were retrieved for full-paper review. Eight trials (n = 652 participants) in patients with RA and one trial in patients with AS (100 participants) fulfilled the inclusion criteria. No further relevant studies were identified from searching the 2008–2009 ACR and EULAR abstracts or article references (Figure 1). For a detailed list of excluded references see the online Appendix available from: www.3epain.com.

Literature search from which 35 articles were selected for detailed review. Eight articles met inclusion criteria.
Characteristics of included studies are summarized in Table 1. The majority of studies were published in the late 1980s, with the most recent publications being Ash, et al23 and Bird and Broggini24. Eight studies were performed in outpatients with RA who were taking various doses of nonsteroidal antiinflammatory drugs (NSAID) and minimal or no disease-modifying antirheumatic drug (DMARD) therapy. All trials evaluated TCA, 7 trials were placebo controlled23,25,26,27,28,29,30, and 2 studies included an SSRI as a comparator24,27. There were 4 studies with 334 participants evaluating amitriptyline24,26,27,29, 2 studies with 52 participants assessing dothiepin23,30, and 1 small study each evaluating trimipramine (n = 20)28 and imipramine (n = 36)25. No trial was longer than 12 weeks in duration, with the shortest study being a single-dose trial with outcomes measured at 2 and 4 hours29. The single trial with AS patients was an RCT that evaluated amitriptyline versus placebo31. All patients were attending a 2 week inpatient physiotherapy course.
Characteristics of included studies.
Amitriptyline
The 4 studies assessing amitriptyline ranged from 2 hours to 3 months in duration. Three of these studies evaluated amitriptyline versus placebo26,27,29 and did not include patients with depression. These trials were heterogeneous, using different doses of amitriptyline, ranging from 25 to 150 mg, and reporting different outcome measures at varying points in time. The Grace 1985 trial27 was a 12 week RCT of amitriptyline versus placebo in patients with active RA not taking corticosteroids or DMARD. The largest trial (n = 210) evaluated amitriptyline against paroxetine (SSRI) in white patients with RA and depression24. In that trial, participants had a mean Ritchie Articular Index of 22 (0–78 scale), no patient was taking DMARD therapy, and 36% were using corticosteroids.
Two trials were crossover studies that included several comparators. Frank, et al26 assessed amitriptyline against desipramine, trazodone, and placebo in 8-week intervals, and Saarialho-Kere, et al29 was a single-dose study that evaluated amitriptyline in combination with dextropropoxyphene versus dextropropoxyphene, indomethacin, and placebo. In both trials, baseline visual analog scale (VAS) scores for pain were about 40 to 50 (0 to 100 mm), and more than 50% of both groups of patients were also receiving corticosteroids or DMARD.
Dothiepin
Of the 2 trials evaluating dothiepin, one was a 12-week placebo-controlled trial23 and one was a 7-week combination trial with ibuprofen (600 mg orally tds) versus placebo and ibuprofen (600 mg orally tds)30. The Ash23 trial included only patients with RA and depression, whereas the Sarzi Puttini trial30 included patients with RA only. Both trials recruited patients with active disease and VAS score for pain > 50 mm. Patients were predominantly women (87%–100%) and additional medications including DMARD were not described in either study.
Trimipramine
One small 12-week trial evaluated trimipramine versus placebo in patients with RA and depression28. These patients had active disease (mean erythrocyte sedimentation rate 61 mm/h) and were not receiving corticosteroids or other DMARD therapy.
Imipramine
One 10-week trial evaluated imipramine against placebo25. This study was designed to assess the effect of imipramine on the titer of rheumatoid factor. Pain was a secondary outcome. No patient was taking corticosteroids or other DMARD and mean baseline pain scores were 2.7–2.8 (0–3 point scale).
Risk of bias assessment
Seven of the 9 trials had high risk of bias, and 2 did not provide enough information and were deemed “unclear.” The predominant methodological flaws of the included trials included failure to describe randomization, allocation concealment, and blinding of study personnel (Figure 2). There were also high dropout rates in many studies, and it was often unclear whether an intention-to-treat analysis was performed or how missing data were dealt with. The clinical trials often used poorly described methods to measure important clinical outcomes, including pain, with studies using the same scale often reporting results differently (e.g., mean scores after treatment, mean improvement from baseline, or number of patients “improved”). The included studies also did not record the concomitant use of other analgesic agents.
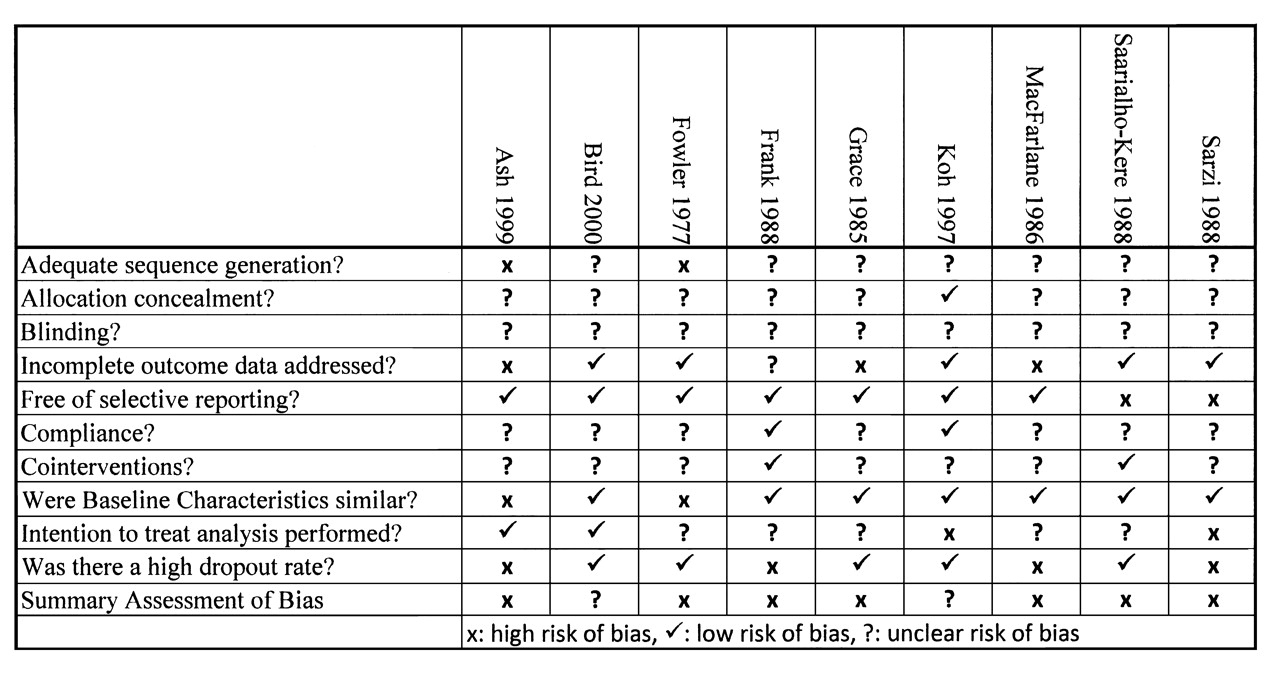
Risk of bias summary: review of authors’ judgments about each risk of bias item for each included study.
Primary outcomes. Efficacy
No study reported the primary outcome measure of patient-reported pain relief ≥ 30%.
Pain intensity (< 1 week).
Two small heterogeneous trials evaluated short-term outcomes and hence metaanalysis was not performed29,30. One small (n = 15) crossover study evaluated amitriptyline in combination with 65 mg dextropropoxyphene and reported inferior pain control at 4 h compared to 130 mg dextropropoxyphene alone using a 100-mm VAS (MD 10.00, 95% CI 0.43 to 19.57) and no significant benefit over placebo (insufficient data provided for analysis)29. A second study compared dothiepin and ibuprofen versus ibuprofen alone and also reported no evidence of benefit30.
Pain intensity (1–6 weeks)
Seven trials evaluated pain outcomes between 1 and 6 weeks’ duration23,24,25,26,27,28,30. There was considerable variability in the doses and types of antidepressants used in these trials, and outcomes were reported at different timepoints. Metaanalysis was not performed due to heterogeneity and high risk of bias in all of the studies.
Two studies reported no benefit of dothiepin at Week 223 and Week 330, respectively. Four studies with high or unclear risk of bias evaluated pain outcomes at 4 weeks23,24,27,28, with 2 studies reporting a benefit over placebo23,28 and 2 studies reporting no benefit over placebo27 or paroxetine24. Two of these studies evaluated amitriptyline and reported no significant benefit over placebo28 or the active comparator paroxetine24.
Macfarlane, et al28 evaluated trimipramine versus placebo in patients with RA and depression, and reported a modest but significant reduction in pain [MD (0–4 pain scale) −0.40, 95% CI −0.78 to −0.02; NNT 3.7, 95% CI 1.9 to 237.4), while Ash, et al23 also reported a significant reduction in pain in depressed patients taking dothiepin versus placebo [MD (VAS 0–100 mm) −25.10, 95% CI −39.97 to −10.23; NNT 2.4, 95% CI 1.6 to 6.8].
Three studies with high risk of bias evaluated pain outcomes at 6 weeks23,25,26. All evaluated different TCA. Ash, et al23 reported a significant reduction in pain in patients taking dothiepin compared to placebo on average of 30.9 points on 100-point scale (95% CI −56.59 to −5.21; NNT 3.1, 95% CI 1.8 to 26.4), Fowler, et al25 did not provide enough data to enable extraction and reported no significant difference in patients taking imipramine. Frank, et al26 reported no significant difference on a 10-cm VAS, but a significant difference on present pain intensity and worst pain in patients taking amitriptyline over placebo (insufficient data for extraction). This finding may have been due to chance and not to true differences. In this trial, trazodone and desipramine failed to show a benefit over placebo.
Pain intensity (> 6 weeks)
Five studies evaluated pain outcomes of more than 6 weeks’ duration23,24,27,28,30. Only 3 of these studies provided data that could be extracted23,24,28. With significant heterogeneity and high or unclear risk of bias, a metaanalysis was not performed.
Two studies23,28 suggested a benefit over placebo, and 2 studies reported no benefit over placebo27,30. Specifically, Ash, et al23 reported a benefit of dothiepin over placebo in depressed patients with RA at up to 12 weeks using a 100-mm VAS (MD −21.90, 95% CI −37.76 to −6.04; NNT 2.2, 95% CI 1.5 to 9.9), while Macfarlane, et al28 reported a significant reduction in pain in patients with RA and depression receiving trimipramine at 8 weeks (MD −0.60, 95% CI −0.89 to −0.31) and 12 weeks (MD −0.80, 95% CI −1.21 to −0.39) using a 0–4 numeric rating scale. Bird and Broggini24 reported that the paroxetine group contained a higher proportion of patients in the “very much improved” and “much improved” categories compared with the amitriptyline group (65% vs 56%, respectively) after 8 weeks; however, this was not statistically significant (RR 1.17, 95% CI 0.93 to 1.48).
Safety. Number of withdrawals due to adverse events
Withdrawals due to adverse events were analyzed across all included studies, with 6 trials reporting data24,25,26,27,28,30. One study reported no withdrawals due to adverse events and so did not contribute to the metaanalysis25. Overall there were 25 withdrawals in 230 patients receiving a TCA and 25 withdrawals in 225 patients receiving a comparator. Event rates in the trials ranged from 3.4% to 27.8%. When pooled there was no significant difference between those receiving a TCA agent versus a comparator (RR 0.98, 95% CI 0.59 to 1.64). When comparing only placebo-controlled trials24 (study removed) the results were unchanged (RR 1.09, 95% CI 0.49 to 2.42).
Total number of adverse events
Despite not leading to withdrawal there were significantly more adverse events in patients receiving TCA compared with those receiving placebo (RR 2.27, 95% CI 1.17 to 4.42). Overall, 50% of patients receiving a TCA reported side effects compared with 32% of patients in the placebo groups (NNTH 5, 95% CI 3 to 22). There was no significant difference when comparing amitriptyline versus paroxetine (RR 1.20, 95% CI 0.96 to 1.50). Adverse event rates in the trials varied from 0% to 56%. The low event rate for individual drugs and doses prohibited any further subgroup analysis.
The most common side effects reported in patients receiving TCA were central nervous system 22% (somnolence, fatigue, headache, dizziness), anticholinergic symptoms 15% (dry mouth, constipation, palpitations), and gastrointestinal 12% (nausea, abdominal pain). Other reported adverse events included hypotension and tremor. There were no cases of serotonin syndrome and no other serious adverse events reported.
Paroxetine was better tolerated than amitriptyline in one trial, with an overall frequency of adverse experiences of 56% and 68% in the 2 groups, respectively24. There was a lower frequency of anticholinergic adverse experiences (18% vs 44% taking amitriptyline), and somnolence was much lower in the paroxetine treatment group (25.0% vs 9.6% with paroxetine).
DISCUSSION
This is the first systematic review to assess the efficacy and safety of antidepressants for treating pain in patients solely with IA. The results of this review served as an evidence base for one of the 10 recommendations regarding pain management by pharmacotherapy, which were generated by a multinational panel of rheumatologists as part of the 3e Initiative. A detailed description of all final recommendations can be found elsewhere18.
Based upon 9 trials of high or unclear risk of bias, it is not possible to draw firm conclusions about the efficacy of TCA as analgesics for patients with IA. In the RA trials with short-term outcomes (< 1 week) there was no significant benefit of amitriptyline 25 mg in combination with dextropropoxyphene (DXP) 65 mg over placebo and inferiority of amitriptyline + DXP versus DXP 130 mg. There was conflicting evidence regarding medium (1–6 weeks) and longer-term (> 6 weeks) benefits on pain. One trial in patients with RA with depression showed no significant difference between amitriptyline and paroxetine over 8 weeks. In AS there was no benefit of amitriptyline over placebo in reducing pain over 2 weeks.
The use of these agents may be associated with adverse events, which are generally mild and do not lead to cessation of treatment. From 5 trials, withdrawals due to adverse events were poorly reported and not significantly different from placebo. However, there were significantly more minor adverse events (somnolence, dizziness, dry mouth, nausea) in patients receiving TCA compared with placebo (RR 2.3, 95% CI 1.2 to 4.4), occurring in 1 in every 5 patients treated on average.
There are several limitations in the interpretation of the results of our review. There were relatively small numbers of placebo or head-to-head trials, short duration of followup, generally poor quality of adverse event assessment, and heterogeneity in study design and interventions. The study populations in the included trials of this review are not reflective of current-day patients with RA. In general they had poorly controlled disease and were receiving only NSAID, with occasional low-dose corticosteroid or DMARD only. The interpretation of a patient’s pain response may also be confounded by associated changes in mood. The percentage of patients with and without depression, and the severity of their depression, varied among the trials. Both trials that showed a benefit of antidepressants for pain included patients with depression, raising the possibility that pain improvement occurred as a result of improvements in mood.
All these factors make comparisons across trials difficult and the conflicting results of the studies are likely to have resulted from these inconsistencies both within and between studies. It is also likely that the methodological failures in the majority of the included trials have contributed to their success or failure in demonstrating the benefits of efficacious treatments. There were no studies that evaluated drugs from antidepressant classes other than the TCA and SSRI, and no trials included newer antidepressant agents (e.g., venlafaxine, paroxetine, sertraline). No conclusions could be drawn regarding optimal dosages of individual agents.
In conclusion, based upon 9 trials of high or unclear risk of bias, it is not possible to draw firm conclusions about the efficacy of TCA as analgesics for patients with IA. The use of these agents may be associated with adverse events, which are generally mild and do not lead to cessation of treatment. Further high-quality trials are required in this area.
Footnotes
-
Based on a Cochrane Review published in the Cochrane Database of Systematic Reviews (CDSR) 2011, Issue 11, doi:10.1002/14651858.CD008920 (for details see www.thecochranelibrary.com). Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and the CDSR should be consulted for the most recent version of the review.








{kind=link}
{kind=link}