

Abstract
Immune-mediated inflammatory diseases (IMID) present a group of common and highly disabling chronic conditions that share inflammatory pathways. Several incidence and prevalence studies of IMID during the past decades have reported a considerable variation of the disease occurrence among different populations. Overall, the estimated prevalence of IMID in Western society is 5%–7%. This article provides an overview of studies of the incidence, prevalence, natural history, and comorbidities of IMID.
Immune-mediated inflammatory disease (IMID) is a concept used to describe a group of prevalent and highly disabling conditions that share common inflammatory pathways. IMID are characterized by acute or chronic inflammation that can affect any organ system. Disorders belonging to this group include, but are not limited to: ankylosing spondylitis (AS), psoriasis, psoriatic arthritis (PsA), rheumatoid arthritis (RA), and inflammatory bowel disease (IBD). The latter includes Crohn’s disease (CD) and ulcerative colitis (UC). Although each of these diseases has unique epidemiology and pathophysiology, their main commonality is that an imbalance in inflammatory cytokines is central to their pathogenesis. Several incidence and prevalence studies of IMID have been reported during the last decades, suggesting a considerable variation of the disease occurrence among different populations. The prevalence of IMID in Western society is about 5%–7%1. Although some IMID, such as psoriasis, have similar prevalence among men and women, others, including RA, are much more prevalent among women2. There are at least 2 theories for the differential prevalence. First, female sex hormones may promote immune-mediated inflammation, and second, fetal cells may lodge within the organs of pregnant women during gestation (a phenomenon called microchimerism) and later cause IMID pathogenesis3–5.
EPIDEMIOLOGY OF IMID — OVERVIEW
Rheumatoid Arthritis
Descriptive epidemiology studies of RA conducted in Northern European and North American countries indicate a population prevalence of 0.5%–1% and a mean annual incidence of 0.02%–0.05%6,7. While a low prevalence of RA has been reported in developing countries7, Native Americans appear to be highly affected by the disease8. A recent systematic review of the incidence and prevalence of RA9 revealed substantial variation depending on gender, ethnicity, and calendar year. These data emphasize the dynamic nature of the epidemiology of RA. Some studies from North American, North European, and Japanese populations suggest a decline in both the prevalence and incidence of the disease after the 1960s10,11. A shift toward a more elderly age of onset was also a consistent finding across several studies12. However, data from Rochester, Minnesota, USA11, demonstrate that although the incidence rate fell progressively over the 4 decades of study — from 61.2/100,000 in 1955 to 1964, to 32.7/100,000 in 1985 to 1994 — there were indications of cyclical trends over time (Figure 1). Moreover, data from the past decade suggest that RA incidence (at least in women) appears to be rising after 4 decades of decline13.
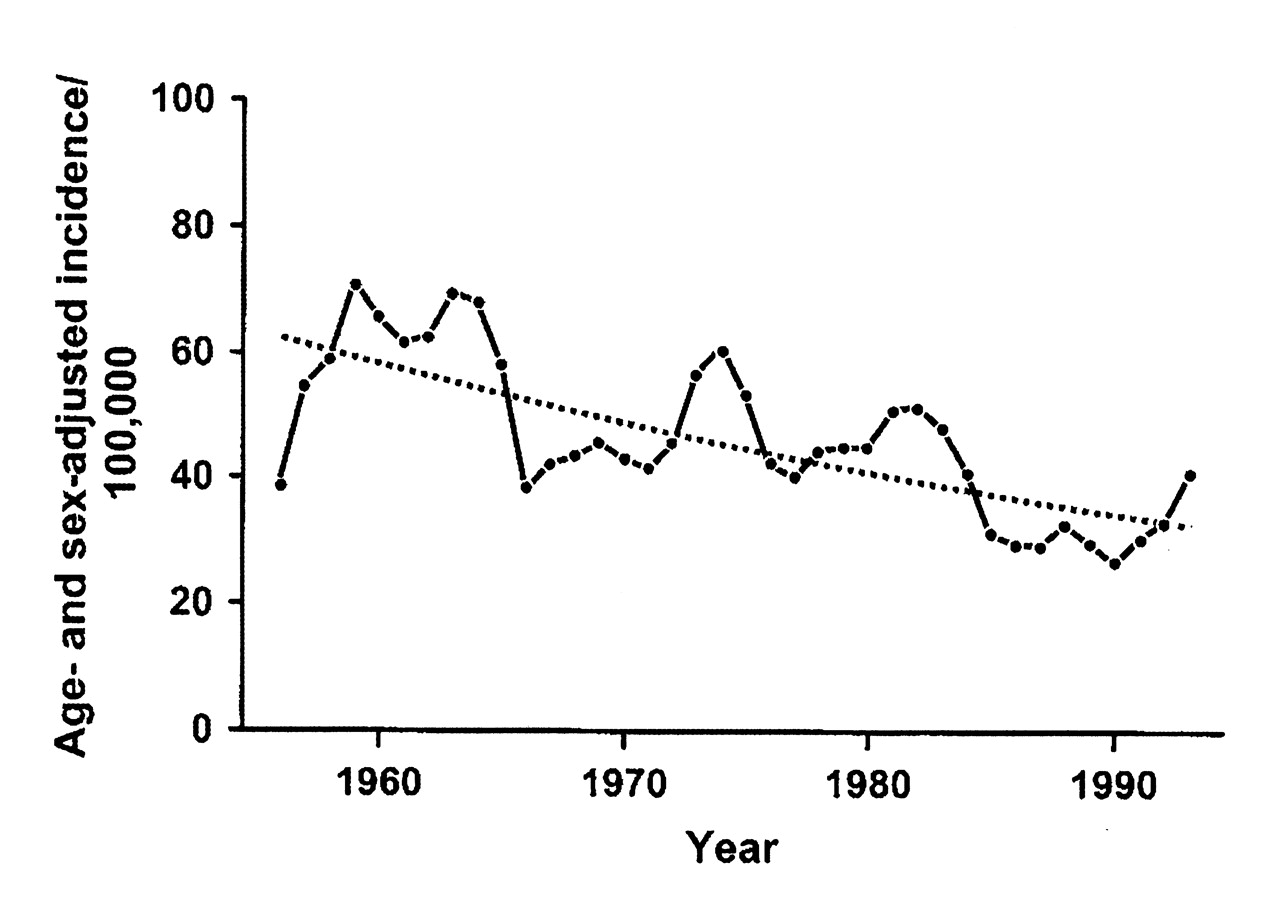
Annual incidence rate of rheumatoid arthritis (RA) in Rochester, Minnesota, USA, per 100,000 population: 1955 to 1995. Each rate was calculated as a 3-year centered moving average. The regression line fitted to the data shows the progressive decline over time. From Doran MF, et al. Arthritis Rheum 2002;46:625-3111, with permission from John Wiley and Sons, Inc.
Gender, ethnicity, and socioeconomic status as risk factors for RA
The incidence of RA is higher in women than in men. The sex ratio varies in most studies from about 3:1 to about 4:114–16. Although this difference suggests an influence of reproductive and hormonal factors on the occurrence of the disease, it is still unclear how exactly gender influences the occurrence of RA7. Socioeconomic factors appear to influence the course and the outcome of RA rather than the risk of developing RA. Available data suggest an association of adverse socioeconomic status with worse prognosis of the disease7.
The significant geographic variations of disease occurrence and the increased incidence observed in some specific ethnic groups suggest an association of RA with ethnicity. The observed differences may reside in the diverse distribution of environmental and genetic factors, as well as in their interaction. The relative prevalence of the RA-associated “shared epitope” alleles of the HLA-DRB1 locus, which are associated with the disease in multiple populations worldwide, is likely the most important genetic factor in determining the variation seen in different ethnic groups. Since smoking is also associated with RA in multiple populations, but primarily in shared epitope-positive individuals, these observations indicate that ethnicity could be considered as an independent risk factor, reflecting interactions between genetic and environmental factors17.
Ankylosing Spondylitis
AS primarily affects men before the age of 45 years. Worldwide prevalence varies from 0.036% to 0.10%12. Disease onset is usually between 17 to 35 years of age. The incidence and prevalence of AS have also been studied in various populations12. The incidence appears to mirror that of human leukocyte antigen HLA-B27 seropositivity; HLA-B27 is present throughout Eurasia, but is virtually absent among the genetically unmixed native populations of Australia, South America, and in certain regions of equatorial and southern Africa. Similar to RA, the prevalence of AS and other spondyloarthropathies is also known to be very high in certain North American Indian populations18,19.
Psoriasis and Psoriatic Arthritis
Although psoriasis occurs worldwide, similar to other IMID, its prevalence varies considerably. About 2% of the North American population is affected20. The disease can present at any age; however, the mean age of onset for the first presentation of psoriasis ranges from 15–20 years of age, with a second peak occurring at 55–60 years21,22.
Henseler and Christophers22 examined a series of 2147 patients and reported 2 clinical presentations of psoriasis, type I and II, distinguished by a bimodal age at onset. Type I begins on or before age 40 years and accounts for more than 75% of cases; type II begins after age 40 years. A positive family history and more severe disease were present in patients with early-onset (type I) psoriasis compared with the later-onset type II disease. Earlier onset has also been reported to be associated with the presence of human HLA-Cw623.
Among patients with psoriasis, the prevalence of inflammatory arthritis varies from 6% to 42%24. A recent study of the incidence of PsA25 reported an overall age- and sex-adjusted annual incidence of 7.2 [95% confidence interval (CI) 6.0–8.4] per 100,000 population (Figure 2). The incidence was higher in men (9.1, 95% CI 7.1–11.0) than in women (5.4, 95% CI 4.0–6.9). Further, the age- and sex-adjusted annual incidence of PsA per 100,000 population increased from 3.6 (95% CI 2.0–5.2) between 1970 and 1979, to 9.8 (95% CI 7.7–11.9) between 1990 and 2000 (p for trend < 0.001). The point prevalence per 100,000 was 158 (95% CI 132–185) in 2000, with a higher prevalence in men (193, 95% CI 150–237) than in women (127, 95% CI 94–160).
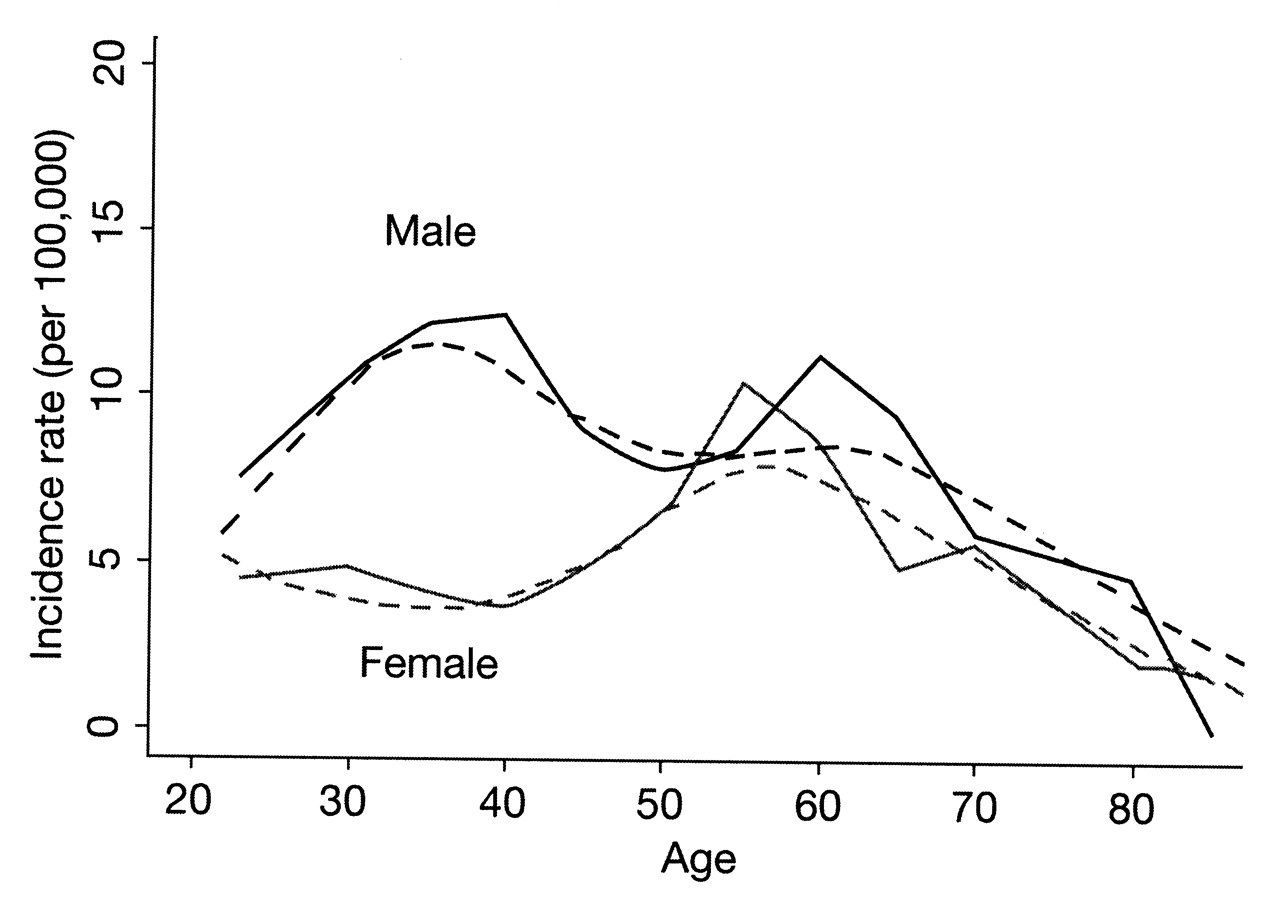
Annual incidence of psoriatic arthritis (PsA) by age and sex. Annual incidence (per 100,000) of PsA by age and sex (January 1, 1970, to December 31, 1999; Olmsted County, Minnesota, USA). Broken lines represent smoothed incidence curves obtained using smoothing splines. From Wilson FC, et al. J Rheumatol 2009;36:361-725; with permission.
Inflammatory Bowel Disease
A number of IBD-related, population-based studies have been published from Europe and North America26–29. Data from these studies suggested a north-south gradient with higher rates of IBD in northern European countries, and northern versus southern states. However, it remains unclear whether these findings reflect a difference between the developed nations in the Northern Hemisphere and developing nations in the Southern Hemisphere, or if there exist environmental influences in northern jurisdictions.
Recently, Bernstein, et al27 reported on the incidence and prevalence of CD and UC by age, sex, and region in the Canadian provinces of British Columbia (BC), Alberta (AB), Saskatchewan (SK), Manitoba (MB), and Nova Scotia (NS) (Table 1). The incidence rate for CD ranged from 8.8 (BC) to 20.2 (NS), and for UC ranged from 9.9 (BC) to 19.5 (NS). The prevalence of CD was about 15 to 20-fold higher than the incidence rate, ranging from 161 (BC) to 319 (NS). This was similar for the prevalence of UC, which ranged from 162 (BC) to 249 (MB). While these rates seem far-ranging, in fact BC was the principal outlier, with quite similar rates among the 3 Prairie Provinces of Canada (AB, SK, MB). Based on these data, it was estimated that in 2005 there were about 170,000 (or roughly 1 in 180) Canadians with IBD. Thus, Canada has one of the highest incidence (Figure 3) and prevalence rates of IBD in the world.

Incidence rates of inflammatory bowel disease reported in the past decade. A. Crohn’s disease; B. Ulcerative colitis. From Bernstein CN, Shanahan F. Gut 2008;57:1185-9130; with permission from BMJ Publishing Group Ltd.
Incidence, prevalence, and incidence rate ratios (IRR) based on sex and urban/rural population for inflammatory bowel disease (IBD) in 5 Canadian provinces: 1998–2000. From Bernstein, et al. Am J Gastroenterol 2006; 101:1559–6827; with permission from Macmillan Publishers Ltd.
Recent changes in global epidemiological trends
The incidence of IBD varies greatly worldwide (Figure 3)30. However, in traditionally high-incidence areas such as Western European and North American countries, the figures have stabilized or slightly increased, with even decreasing incidence rates for UC31. In contrast, low prevalence and incidence rates have historically been reported in other parts of the world, including Eastern Europe, South America, Asia, and the Pacific region. Recent trends, however, also indicate a change in the epidemiology in these areas as they are now reporting a progressive increase in the incidence of IBD.
It is also important to note that, as IBD emerges in developing countries, UC appears first, followed at a variable interval by a rising trend in CD30. This trend has been observed in countries and global regions, as well as in societal sectors living in underdeveloped conditions within highly developed countries. Examples of the latter include the First Nations of Canada32 and the Maoris of New Zealand33.
Although some of the recent changes in IBD epidemiology in developing areas may represent differences in diagnostic practices and increased awareness of the disease, it is more likely that changes in environmental factors have led to changes in the incidence of IBD. This abrupt increase in frequency of IBD when there is a transition from a “developing” to a “developed” nation further demonstrates how modifications in lifestyle and the environmental influences of modern society contribute to changing epidemiology of certain diseases. In Canada, for instance, the difference between incidence rates of CD in BC versus other provinces may be explained by population genetics, with nearly one-fourth of British Columbians being visible minorities and many being new immigrants who would more likely carry the risk for these diseases from their native countries. Hence BC will be a particularly important jurisdiction to follow over time to determine if incidence rates among children of Asian immigrants growing up in BC rather than Asia have incidence rates similar to Caucasian Canadians. If rates of CD remain low in BC, this may be due to a distinct and protective environmental influence compared to the Prairie Provinces or Atlantic Canada.
CO-OCCURRENCE AND COMORBIDITIES — IMPACT ON IMID OUTCOMES
Comorbidities are often present in patients with IMID and greatly contribute to the burden of disease, healthcare utilization, and impairment of quality of life. Numerous studies have established that, in comparison to the general population, IMID patients are at greater risk for developing another IMID-related condition34–36. Although multiple IMID may coexist within the same patient, individuals with IBD or with AS are more likely to have another IMID than patients with RA. For example, a large study of patients with AS found that 39% of subjects also developed iritis, 16% psoriasis, and 8% IBD36. Various IMID may also coexist within the same family. Using US healthcare claims data, Robinson, et al34 demonstrated that among musculoskeletal IMID, AS conferred a particularly pronounced risk for IBD [relative risk (RR) 7.63–8.62]. Further, this risk relationship was bidirectional: among IBD patients, the RR for AS is between 5.81 and 7.75.
The average RA patient, for example, has about 1.6 comorbidities37, and the number increases with the patient’s age. Patients with IMID are at particularly high risk for infectious, cardiovascular, and renal disease, as well as malignancies34. Lymphoma is the most common cancer in IMID patients. As expected, these comorbidities add considerable complexity to patient care, making diagnosis and treatment decisions more challenging. Therefore, it is important to recognize such illnesses and to account for them in the care of the individual patient.
Rheumatoid Arthritis
It has been demonstrated that the excess mortality in persons with RA is largely attributable to cardiovascular disease (CVD)38. Research has also repeatedly demonstrated that the risk for ischemic heart disease is significantly higher among persons with RA than in control individuals39,40. A recent population-based study showed that RA patients are at a 3.17-fold higher risk for experiencing a hospitalized myocardial infarction (MI; multivariable odds ratio = 3.17, 95% CI 1.16–8.68) and a nearly 6-fold increased risk for having a silent MI (multivariable odds ratio = 5.86, 95% CI 1.29–26.64) compared with age- and sex-matched non-RA subjects40.
An emerging body of evidence indicates that persons with RA are also at increased risk for heart failure. The cumulative incidence of heart failure, defined according to Framingham Heart Study criteria41, after incident RA has been shown to be statistically significantly higher in persons with RA versus those without the disease in a population-based setting42. At all age levels, the incidence of heart failure in RA patients was about twice that in non-RA individuals.
After CVD, cancer is the second most common cause of mortality in RA patients. The overall standardized incidence rate (SIR) of non-skin cancer malignancy in RA is estimated to be 1.05 (95% CI 1.01–1.09)43. Although the risk appears to be slightly increased in persons with RA, this increase appears to be due to only a few specific malignancies: lymphoma, lung cancer, and skin cancer. According to Baecklund, et al44, lymphoma is not only increased in RA but also is related to the severity of the disease itself. After analyzing combined data from 6 recent studies, Smitten and coworkers43 determined the SIR of lymphoma to be 2.08 (95% CI 1.80–2.39) in RA.
Recent research has linked smoking exposure to an increased incidence of developing RA45,46. After examining 12 recent studies, Smitten and coworkers43 reported an SIR of 1.63 (95% CI 1.43–1.87) for lung cancer in RA. This increase in lung cancer is probably related, at least in part, to the high smoking rates in RA47.
Similar to other inflammatory disorders, RA appears to increase the risk for bacterial, tubercular, fungal, opportunistic, and viral infections. Further, these infections are more common in more active and severe RA48. Although anti-tumor necrosis factor (TNF) therapy has been associated with increased risk for infection49,50, studies in RA patients before the era of methotrexate (MTX) and anti-TNF showed a general increase in mortality due to infections in these patients51–54. In a recent study in an inception cohort of 2108 patients with inflammatory polyarthritis from a community-based registry, the incidence of infection was more than 2.5 times higher than that in the general population. Smoking, corticosteroid use, and rheumatoid factor were also found to be significant, independent predictors of infection-related hospitalization55.
Psoriasis and PsA
Individuals with psoriasis are at increased risk for insulin resistance, obesity, dyslipidemia, and hypertension — components that characterize the metabolic syndrome56. The metabolic syndrome is an important driver of adverse CV outcomes. Proinflammatory cytokines such as TNF-α and other factors that are overproduced in patients with psoriasis likely contribute to the increased risk for development of the metabolic syndrome. Recently, Gelfand, et al57 suggested that psoriasis is an independent risk factor for MI. Further, the risk of psoriasis-related MI is greatest in young patients with severe psoriasis, is attenuated with age, and remains increased even after controlling for traditional CV risk factors. Although psoriatic patients are also more likely to be obese, the causal link between psoriasis and obesity has not been established. While a large prospective study indicated that increased adiposity and weight gain are strong risk factors for incident psoriasis in women58, Herron, et al59 concluded that obesity usually develops after the onset of psoriasis. Smoking, on the other hand, appears to have a role in the onset of psoriasis and increased risk of malignancies in this patient population59,60. Alcoholism is also highly prevalent among psoriatic patients, contributing to liver disease and aggravation of psychiatric disorders61. Other comorbidities significantly associated with psoriasis include arthritis, depression, sleep disorders, chronic obstructive pulmonary disease, and gastroesophageal reflux disease62.
Inflammatory Bowel Disease
According to a systematic review of 11 studies, published between 1965 and 2006, there is no statistically significant increase in CV-standardized mortality ratios (SMR) in patients with IBD compared to the general population11. However, increased carotid intima media thickness (IMT)63,64, increased risk of cerebral and arterial thromboembolic disease65, and microvascular endothelial dysfunction66 have been reported. Romanato, et al67 found total and low-density lipoprotein cholesterol to be lower in active UC and CD than in the healthy subjects. This could be secondary to malabsorption as a result of faster intestinal transit and/or systemic inflammation causing reduced lipoprotein and hepatic lipase activity. Further, reduction in high-density lipoprotein (HDL) during CD exacerbation implies an impaired HDL protection in these patients63.
IMID-RELATED MORTALITY
A wealth of evidence supports the observation that persons with IMID have a shorter lifespan than the general population. Although mortality rates vary widely among studies, they are consistently higher in hospital-based than in population-based studies7,68. The expected survival of RA patients is likely to decrease by 3–10 years according to the severity of the disease and the age of disease onset7. As the most common causes of death do not differ significantly among RA patients and the general population, it can be concluded that the majority of affected individuals die from the same causes as the general population, but at a younger age67,70. The strongest predictors of survival in RA appear to be those related to disease complications, extraarticular manifestations of the disease, and comorbidities (Table 2)70.
Predictors of mortality in 609 incidence cases of RA. From Gabriel SE, et al. Arthritis Rheum 2003;48:54–5870; with permission from John Wiley and Sons.
Similarly, Wong, et al71 found the 4 leading causes of death in PsA to be diseases of the circulatory (36.2%) or respiratory (21.3%) system, malignant neoplasms (17.0%), and injuries/poisoning (14.9%). The SMR for the female PsA Toronto cohort was 1.59, and for the men it was 1.65, indicating a 59% and 65% increase in the death rate, respectively, over the study’s 15-year followup period compared with the general Ontario population.
According to Gelfand, et al72, male and female patients with severe psoriasis died 3.5 (95% CI 1.2–5.8) and 4.4 (95% CI 2.2–6.6) years younger, respectively, than patients without psoriasis (p < 0.001).
IBD is a relatively uncommon cause of death, and a general trend suggests continued reductions in IBD-related mortality. However, IBD is still associated with reduced life expectancy in certain subgroups, such as those with pancolitis or older age at diagnosis73. A recent metaanalysis using a random-effects model shows the pooled estimate for SMR in CD is 1.52 (95% CI 1.32 to 1.74, p < 0.0001) compared to the general population74.
SUCCESSFUL IMID MANAGEMENT REDUCES CVD BURDEN AND MORTALITY
It has been suggested that successful treatment of IMID and reduction of inflammation might reduce CV morbidity and mortality. For example, Prodanovich, et al75 showed that MTX therapy reduced the incidence of vascular disease in veterans with psoriasis or RA. Patients prescribed MTX therapy had a significantly reduced risk of vascular disease compared to those who were not prescribed MTX (psoriasis: RR 0.73, 95% CI 0.55–0.98; RA: RR 0.83, 95% CI 0.71–0.96). The authors hypothesized that this effect is caused by the antiinflammatory properties of MTX. These data are supported by the Quest-RA study, which demonstrated that successful treatment of RA and prolonged exposure to MTX [hazard ratio (HR) = 0.85, 95% CI 0.81–0.89], leflunomide (HR 0.59, 95% CI 0.43–0.79), sulfasalazine (HR 0.92, 95% CI 0.87–0.98), glucocorticoids (HR 0.95, 95% CI 0.92–0.98), and biologic agents (HR 0.42, 95% CI 0.21–0.81; p < 0.05) were associated with a reduction in risk of CV morbidity76.
The effectiveness of anti-TNF therapy on reduction of CV events is supported by several studies77–79. According to Jacobsson et al77, the age- and sex-adjusted incidence rate of a first CVD event in RA patients receiving an anti-TNF agent is 14.0/1000 person-years (95% CI 5.7–22.4), compared with 35.4/1000 person-years (95% CI 16.5–54.4) in RA patients who did not receive anti-TNF therapy. Controlling for disability, the age- and sex-adjusted rate ratio was 0.46 (95% CI 0.25–0.85, p = 0.013) in anti-TNF-treated versus untreated subjects. In an analysis of patients who responded to anti-TNF-α therapy within 6 months versus those who did not, MI rates were found to be 3.5 events/1000 person-years in responders and 9.4 events/1000 person-years in nonresponders (Figure 4)78.

Incidence rates of first myocardial infarction (MI) in responders and nonresponders to anti-tumor necrosis factor treatment. From Dixon WG, et al. Arthritis Rheum 2007;56:2905-1278; with permission from John Wiley and Sons, Inc.
In a retrospective analysis of patients with RA, PsA, and AS receiving etanercept or placebo in clinical trials, treatment with etanercept was associated with a trend toward lower exposure-adjusted rates of CV events in the etanercept group compared with placebo. The trend of lower event rates in the etanercept group was consistent across all types of CV events, including congestive heart failure79.
CONCLUSIONS
IMID are common, highly disabling conditions with a prevalence in Western society of between 5% and 7%. Patients with IMID are more likely than unaffected individuals to have another IMID, supporting the concept that the diseases are related. High comorbidity rates, especially CVD, associated with IMID add to the already high socio-economic burden of these diseases. Thus, regular screening of IMID patients for signs and symptoms of CVD (i.e., monitoring blood pressure, glucose and lipid levels, waist circumference, and body mass index) is highly recommended. It has also been suggested that successful treatment of IMID and reduction in inflammation might reduce CV morbidity and mortality. However, potent immunosuppressive agents may contribute to an increased risk for infection and cancer.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵








{kind=link}
{kind=link}
{kind=link}
{kind=link}