

Abstract
Despite recent advances in the treatment of rheumatoid arthritis (RA), including the introduction of biologic therapies and employment of combination disease-modifying antirheumatic drug (DMARD) strategies, remission rates remain suboptimal and patients with RA are still missing a significant number of work days. Early diagnostic criteria are needed to ensure that appropriate treatment is initiated early so as to prevent joint damage. Better prognostic markers are also needed to identify patients with the potential for poor outcomes, in whom more aggressive strategies can be applied at the outset. Because of stringent inclusion criteria and heterogeneous definitions of remission, results seen in clinical trials of RA are not necessarily generalizable to results seen in clinical practice. As a result, existing guidelines may not adequately reflect current practice. In the absence of biomarkers to predict the course of disease, methotrexate remains the standard of care initially for most patients with RA. The ability to predict the course of disease could allow more appropriately targeted therapy and higher rates of remission.
In the absence of a cure for rheumatoid arthritis (RA), treatment for affected patients is aimed at controlling the inflammatory process so as to alleviate pain and stiffness, prevent joint deformity and work loss, and improve overall quality of life. Ideally, if the needs of RA patients were being met, all patients would have their disease diagnosed and treated early, before any permanent soft tissue, cartilage, or bone damage could occur. All patients would experience true remission, with no signs or symptoms of RA and no progression of joint damage, regardless of how it is measured. Patients would no longer be dependent on medications that they could not tolerate and/or afford. All patients would be treated according to algorithms based on current guidelines, with ready access to whatever therapies they needed. Biomarkers would exist to help physicians determine tailored and optimal treatments for their patients. Ultimately, all patients would be able to return to full function with no loss of work productivity.
Despite recent strides in achieving remission and reducing radiographic progression in patients with RA, these standards have not yet been met. By reviewing evidence from randomized, controlled trials of newer RA therapies, this article examines the reasons behind the unmet needs of patients with new-onset RA.
UNMET NEEDS LIMITING THE OPTIMAL TREATMENT OF RA
The disease course of RA is unpredictable, and a sophisticated means of predicting a patient’s disease course is currently lacking. RA may manifest a variety of disease courses. Some patients may experience a severe, acute onset of symptoms, while others may experience chronic, intermittent symptoms. No biomarkers currently exist to predict the course of disease. As a result, rheumatologists tend to prescribe methotrexate (MTX) monotherapy – the current standard of care for RA. MTX monotherapy has a reasonably rapid onset of action leading to improvements in the signs and symptoms of disease; however, only 40% of patients will achieve a 50% improvement in the American College of Rheumatology criteria for improvement in RA1 (ACR50), and only 20% of patients will achieve an ACR70 with MTX treatment alone even when used early2–4. Complete inhibition of radiographic progression occurs in only half of patients, and about half of patients discontinue treatment within 5 years5.
Remission
Remission for RA has been defined in many ways6, but no single means of measuring it has been adopted in the clinical setting, and there are controversies and barriers to implementing remission as a clinical target. First, healthcare providers tend not to target a composite remission state. Second, patients tend to accept small improvements in their original active disease state, having adapted to a chronic disease and their current therapy, rather than switch therapies. Switching therapy creates patient anxiety about uncertain responses and concerns about cost and potential side effects. Third, despite data showing cost-effectiveness of treatments, access to therapies is still restricted by formularies or by private insurers through requirements for co-payments and by limiting costly therapies only to those with the most severe and long-standing disease. Public payers may require patients to meet ACR criteria for the classification of RA7, such as the presence of radiographic erosions or rheumatoid factor, which may appear too late in the progression of disease for optimal treatment efficacy. There is often also a requirement for inadequate responses to multiple DMARD therapies, despite the lack of a clear definition for inadequate response. Further, there is a “disconnect” between an inadequate response, which is often defined as the 28-joint Disease Activity Score (DAS28)8 above 3.2, and remission, which has been frequently defined as DAS28 below 2.6. Patients with a disease activity between DAS28 3.2 and 2.6 may fall into an intermediate zone, where in some cases this goal is sufficient and in other cases it may not be. Inconvenient modes of administration with the newer agents, such as monthly infusions, and ongoing concerns about the risk of serious adverse events are additional barriers to achieving remission.
A number of randomized, clinical trials have examined the efficacy of the DMARD in the treatment of early RA2–4,8. The highest clinical remission rate achieved to date in patients with early RA, who have met 1987 ACR criteria for the definition of RA, has been in the range of 50%, using a combination of etanercept and methotrexate in the COmbination of Methotrexate and ETanercept in active, early, moderate to severe rheumatoid arthritis (COMET) trial4, and the combination of adalimumab and MTX in the PREMIER trial2. In the COMET trial, patients treated with the combination of etanercept and MTX achieved remission, according to the DAS28, at 141 days, compared with 365 days for patients who received MTX monotherapy. At one year, the mean DAS28 scores were 2.91 in the combination arm and 3.97 in the MTX monotherapy arm4.
In the Trial of Etanercept and Methotrexate With Radiographic Patient Outcomes (TEMPO), the combination of etanercept and MTX resulted in a remission rate of 41% after 3 years, compared with only 18% in MTX alone (p < 0.05) in patients with a longer duration of disease who had previously failed treatment with a DMARD9.
Although the remission rates in these trials are far from optimal, the results are encouraging given that enrolled patients had a shorter duration of disease, and more severe disease, with a higher number of tender and swollen joints than the average patient presenting in clinical practice with early RA. To determine whether data from randomized, clinical trials are generalizable to patients with early RA, Bykerk and colleagues evaluated whether their “real life” patients would have been eligible for inclusion in 44 published clinical trials10. Only 0.7% to 52% of the patients in this multicenter cohort would have been deemed eligible for inclusion in these clinical trials, highlighting the disconnect between randomized, controlled trials and patients in clinical practice with early RA. That a substantial portion of patients with severe disease have been able to achieve remission in clinical trials is therefore encouraging, as higher remission rates are anticipated to occur in the patient in clinical practice with less severe disease.
Studies have not yet compared the combination of conventional DMARD with MTX plus an anti-TNF therapy as an initial treatment strategy in new-onset RA. Trials on the horizon include the Rheumatoid Arthritis Comparison of Active Therapies (RACAT)11 study and the Treatment of Early Aggressive Rheumatoid Arthritis (TEAR) study12, which will compare the initial combination of MTX, hydroxychloroquine, and sulfasalazine with the combination of etanercept and MTX therapy.
Sustainability of remission
Despite the efficacy of the anti-TNF therapies in alleviating symptoms of RA, longterm sustainability is poor. Longterm data from open-label extensions of clinical trials with etanercept have shown that 8% of patients with early disease and 13% of those with long-standing disease have stopped treatment by 10 years due to a lack of efficacy13. In a prospective cohort of patients with RA in a United Kingdom national registry who had received a new anti-TNF therapy, 12% of patients prescribed adalimumab, 10% of those prescribed etanercept, and 15% of those prescribed infliximab had stopped taking their medication due to a lack of efficacy after a mean followup of 15 months14. Patients were more likely to switch to a second agent if they discontinued the first agent due to inefficacy than if they had discontinued due to an adverse event. As well, patients who discontinued one agent due to a lack of efficacy had a 3-fold greater risk of stopping a second medication for lack of efficacy compared with those who had discontinued the first agent because of the development of an adverse event14.
Recent evidence suggests that a patient’s longterm success with RA therapy can be determined based on their early response to treatment. By examining pooled data from 1,342 patients with early RA enrolled in clinical trials of DMARD, Aletaha, et al15 showed that a patient’s response to treatment during the first 3 months of therapy determined their level of disease activity at one year. Treatment strategies for early and late RA should therefore target disease activity at 3 months. Knowing how to target therapy for these patients to ensure remission is critical.
There is some evidence that the sustainability of the anti-TNF therapies is limited by their immunogenicity to epitopes on monoclonal antibodies. In a prospective, observational study of 121 consecutive patients at an Amsterdam medical center, patients with active RA who had previously failed treatment with 2 DMARD were treated with adalimumab16. Antibodies to adalimumab were detected in 17% of the cohort. Patients with these antibodies had significantly lower serum concentrations of adalimumab and diminished clinical response versus patients lacking these antibodies. The formation of anti-adalimumab antibodies may therefore be one explanation for some patients’ failure to respond to therapy.
Halting progression of joint damage
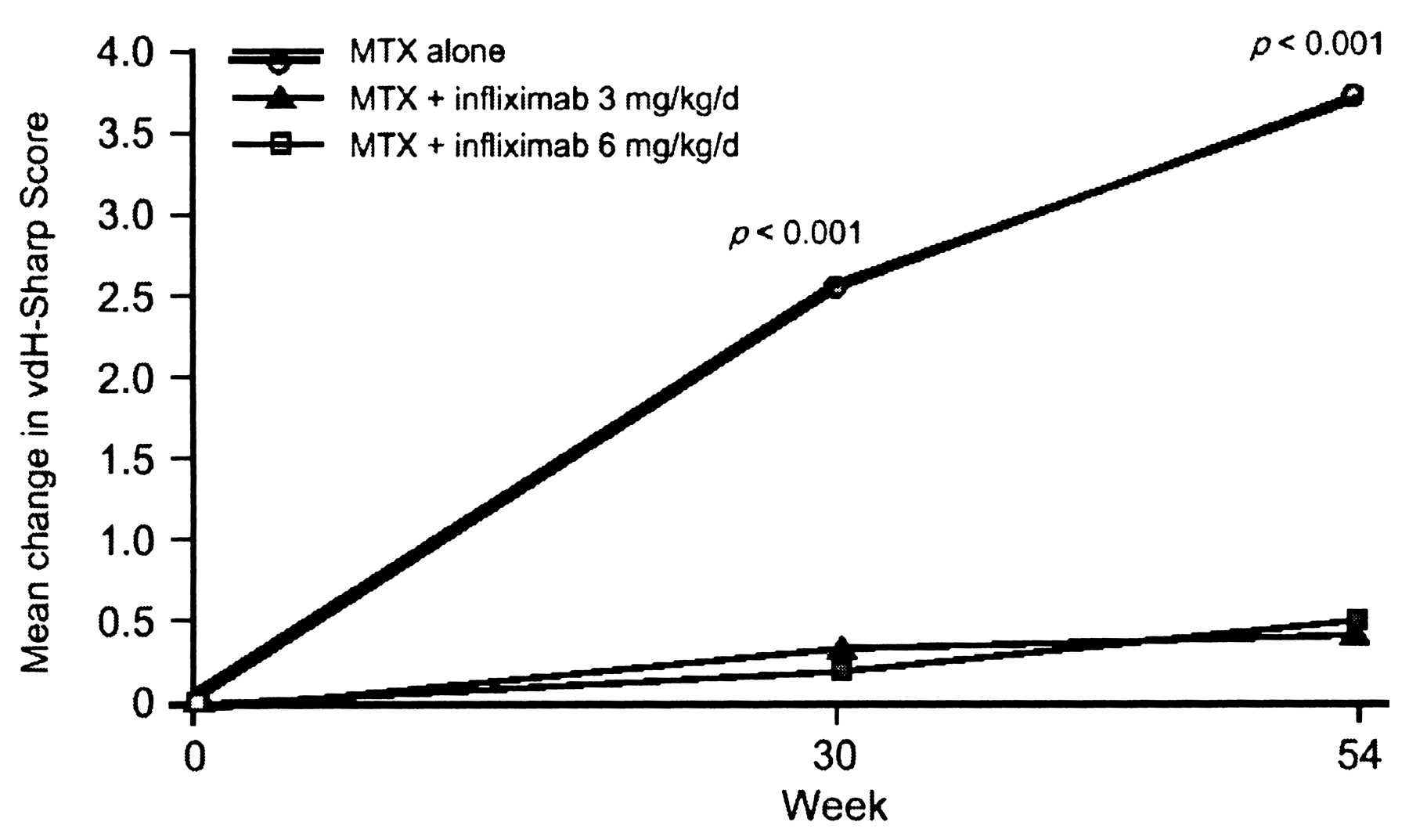
Halting progressive joint damage is not always achieved in patients with RA, particularly in patients with moderate to severe disease receiving DMARD monotherapy. In the Active-Controlled Study of Patients Receiving Infliximab for Treatment of Rheumatoid Arthritis of Early Onset (ASPIRE) trial, the combination of infliximab and MTX was compared with MTX monotherapy alone in RA patients with no prior MTX or anti-TNF therapy3. One of the major secondary endpoints was progression of joint destruction, as measured by the van der Heijde modification of the total Sharp score16. Combination therapy with infliximab and MTX was found to prevent the progression of joint destruction in patients with early RA, and was superior to MTX alone. Patients treated with MTX monotherapy continued to worsen significantly, as seen in the mean change in total Sharp score of 3.7, while patients treated with either 3 mg/kg or 6 mg/kg of infliximab showed almost no progression (0.4 ± 5.8 for 3 mg/kg and 0.5 ± 5.6 for 6 mg/kg; p < 0.001 for each comparison; Figure 1). Similar results were seen in the PREMIER trial, which showed significantly less radiographic progression at years 1 and 2 among patients treated with a combination of MTX and adalimumab (Sharp scores 1.3 and 1.9, respectively) compared with patients treated with either MTX (Sharp scores 5.7 and 10.4) or adalimumab alone (Sharp scores 3.0 and 5.5) (p < 0.002)2.

Mean change in van der Heijde (vdH)-modified Sharp scores in patients in the Active-Controlled Study of Patients Receiving Infliximab for Treatment of Rheumatoid Arthritis of Early Onset (ASPIRE) trial3.
Further, when evaluating progression of joint damage, mean values may not fully explain differences between treatments, as only 10% to 40% of patients will experience radiographic progression in a study. To determine whether joint damage is really being affected by a particular treatment, it is important to know the proportion of patients who actually progress radiographically. In the COMET trial, radiographic nonprogression – defined as a modified total Sharp score of 0.5 or less – was achieved by 80% of patients who received a combination of etanercept and MTX compared with 59% of patients who received MTX monotherapy (p < 0.001)4. These results demonstrate that both remission and halting radiographic progression are realistic therapeutic goals when combination therapy is initiated early in the RA disease process.
Return to work/function
Because of the debilitating nature of RA, loss of work productivity is a major concern for patients, and therapies to facilitate the patient’s return to work are needed. A companion health outcomes study to the PREMIER trial collected patient-reported measures of work performance, including number of missed work days because of RA and degree of work performance affected by RA, based on a visual analog scale (VAS-work)17. In a one-year period, patients treated with a combination of adalimumab and MTX missed 11 days of work compared with 24 missed days for patients treated with MTX monotherapy. Patients treated with the combination therapy also experienced greater improvements in work performance than the monotherapy group, suggesting that those who received the anti-TNF therapy early in the disease process tended to stop missing work fairly quickly18. Similar results were seen in the COMET trial, where patients who received a combination of the anti-TNF therapy etanercept and MTX missed fewer days of work from weeks 12 to 52, compared with those treated with MTX monotherapy4. While encouraging, these results show that, even with combination treatment, patients with RA are still missing a significant number of work days. Despite the higher work productivity demonstrated in patients with RA who receive an anti-TNF therapy early in the disease process, many public payers do not offer ready access to these agents in early disease.
CURRENT RECOMMENDATIONS FOR THE OPTIMAL TREATMENT OF RA
In light of the recent addition of biologic agents to the available therapies for treatment of RA, the ACR recently developed recommendations for the use of nonbiologic and biologic DMARD19. Following a systematic review of the scientific evidence, a series of treatment algorithms were developed based on disease duration and features of poor prognosis, which were subsequently validated using a series of clinical scenarios. Although such recommendations are useful to help guide therapy, they assume that every rheumatologist will use composite scores to determine the extent of disease activity and will make treatment decisions accordingly. The ACR algorithms also include recommendations that are not necessarily supported by payers. They do, however, provide options for patients with “cost or insurance limitations.” Presuming that these options are suboptimal, Bathon and Cohen commented that the mere fact that guidelines must factor in the possibility that patients cannot always afford the best treatments is a “sad commentary on our broken health care system” and may be “inadvertently construed as ACR support of a 2-tiered health care system, in which denial of expensive therapies to the poor is justifiable”20. Also, guidelines tend to rely almost solely on randomized, controlled trials rather than on real life, which limits their applicability to clinical practice.
CONCLUSIONS
Despite therapeutic advances in the treatment of RA, there are still a number of unmet needs in this patient population. Early diagnostic criteria are needed for new-onset, early inflammatory arthritis, as are more precise clinically implementable definitions of remission. Better predictive markers and/or algorithms are also needed to identify patients with a poor prognosis, in whom more optimal strategies can be applied at the outset.
In order to overcome obstacles to optimal treatment of RA, there needs to be an awareness of RA as a substantially disabling and life-threatening disease, comparable to the level of awareness for other diseases, such as multiple sclerosis and cancer. Patients need a better understanding of the implications of being diagnosed with RA and need to be treated according to effective algorithms, with no barriers to treatment access. Primary care physicians need to incorporate screening questions into their routine visits to identify patients early, and to expediently refer patients using an informative referral tool. Further studies need to be done to determine the optimal initial treatment strategy. Rheumatologists need to be able to rapidly evaluate patients who do not initially respond to a trial of MTX using prognostic tools such as biomarkers, enabling rapid diagnosis and prognosis.
Footnotes
-
Supported by an unrestricted educational grant from Bristol-Myers Squibb Canada.








{kind=link}