

Familial Mediterranean fever (FMF) has been reported to be associated with vasculitis, including polyarteritis nodosa (PAN), yet vasculitis is not considered a manifestation of FMF.1
A 29-year-old male, diagnosed with FMF (compound heterozygote for V726A/E148q) at the age of 10 years, was admitted to our ward due to a recent exacerbation of FMF attacks. He was in complete remission with 2 mg/day of colchicine for several years and therefore decided to stop therapy. Three months prior to his admission, he began suffering from recurrent FMF attacks that included abdominal and pleuritic chest pain, accompanied by painful subcutaneous nodules on his arms and legs, lasting for 2 to 3 days (Figure 1). He reported no weight loss, fever, testicular pain, or arthralgia.

Painful erythematous subcutaneous nodules, appearing on the patient’s arms and legs parallel to FMF attacks, lasting 2 to 3 days. FMF: familial Mediterranean fever.
Laboratory tests revealed only a high C-reactive protein level during attacks and increased serum amyloid A (SAA) of 28 mg/L between attacks. Abdominal computed tomography angiography was normal. A skin biopsy of a subcutaneous nodule revealed fibrinoid necrosis within vessel walls, consistent with PAN (Figure 2).
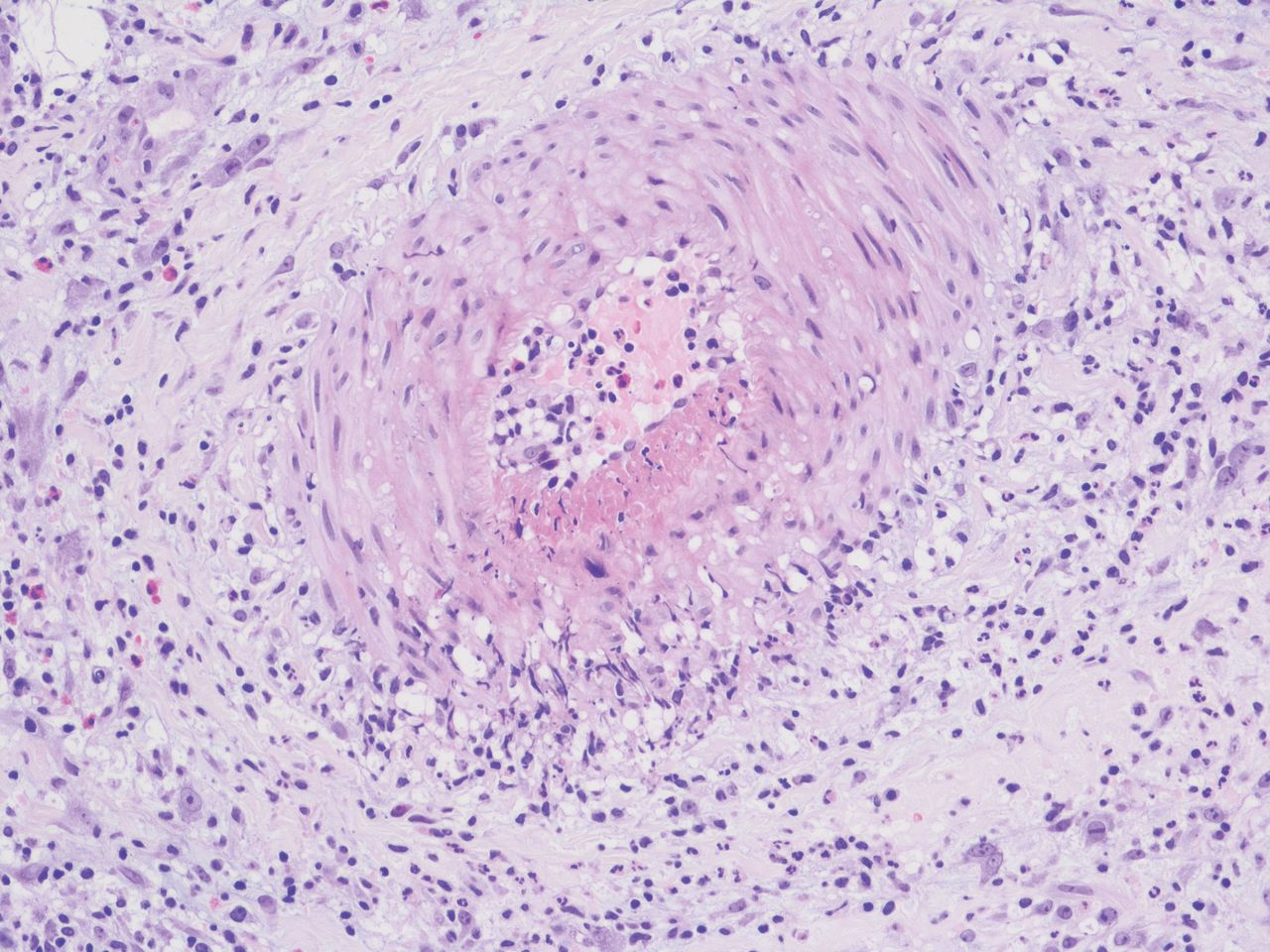
Skin biopsy of a subcutaneous nodule revealing fibrinoid necrosis within vessel walls, consistent with polyarteritis nodosa.
Reestablishing colchicine therapy at 1.5 mg/day resulted in complete remission of his attacks including the subcutaneous nodules, as well as a reduction of SAA value between attacks to 16 mg/L.
The temporal relation of FMF attacks with episodic cutaneous PAN vasculitis, and the complete response to colchicine therapy, suggest that vasculitis is not merely associated, but may be driven by autoinflammation, as proposed in our previous report.2 Indeed, interleukin 1, a key player in autoinflammatory diseases, has a deleterious, procoagulant, inflammatory effect on endothelial cells that may partially explain the predilection to vasculitis.3,4
Footnotes
The authors declare no conflicts of interest relevant to this article. Ethics approval was not required by the authors’ institution. The patient’s written consent was obtained.
- Copyright © 2023 by the Journal of Rheumatology








{kind=link}
{kind=link}