

Abstract
Objective To develop and validate a patient knowledge questionnaire regarding axial spondyloarthritis (axSpA).
Methods Knowledge considered essential for patients with axSpA was identified through Delphi rounds among rheumatologists, healthcare professionals (HCPs), and patients, then reformulated to develop the knowledge questionnaire. Cross-sectional validation was performed in 14 rheumatology departments to assess internal validity (Kuder-Richardson coefficient), external validity, acceptability, reproducibility (Lin concordance correlation coefficient), and sensitivity to change (knowledge score before vs after patient education sessions and effect size).
Results The Spondyloarthritis Knowledge Questionnaire (SPAKE) is a self-administered 42-item questionnaire with a 32-item short form, both scored 0 to 100, assessing knowledge of disease, comorbidities, pharmacological treatments, nonpharmacological treatments, self-care, and adaptive skills. In the validation study (130 patients; 67 [51.5%] male, mean age 43.5 [SD 12.9] yrs), the mean (SD) score of the long-form questionnaire was 71.6 (15.4), with higher scores (better knowledge) in nonpharmacological treatments and adaptive skills and lower scores in cardiovascular comorbidity and pharmacological treatments. Acceptability was good, with no missing data; the internal validity coefficient was 0.85. Reproducibility was good (0.81, 95% CI 0.72-0.89). SPAKE showed good sensitivity to change; scores were 69.2 (15.3) then 82.7 (14.0) after patient education sessions (Hedges effect size = 0.92, 95% CI 0.52-1.31).
Conclusion SPAKE is a knowledge questionnaire for patients with axSpA, developed with the involvement of HCPs and patients and reflecting current recommendations for the management of axSpA. SPAKE will be useful in assessing knowledge acquisition and self-management strategies in routine care and research.
Self-management strategies help patients improve or maintain their quality of life1,2 by playing an active role in their learning about their condition and building their ability to deal effectively with its practical, physical, and psychological effects.2 Patient education (PE) underpins all self-management interventions1,3 and is part of the standard of care for people with inflammatory arthritis4 and spondyloarthritis (SpA).5,6 PE includes a wide range of activities such as individual and/or group sessions through face-to-face or online interactions.4 It is recommended that PE should be individually tailored and based on each patient’s educational needs, performed by trained healthcare professionals (HCPs), and assessed for effectiveness and outcomes.4 Several PE needs have been identified in patients with inflammatory arthritis7 and some are particularly important for patients with SpA,8 such as knowledge of disease characteristics and management, course and prognosis, social support,9 or self-help.10 Assessing a patient’s knowledge is important, from an individual point of view as a starting point for appropriate information and education, and from a collective point of view for the evaluation of educational and self-management interventions.
Only 1 validated knowledge questionnaire is available for patients with ankylosing spondylitis11 or psoriatic arthritis.12 Although still used,13,14 this generic questionnaire was constructed in 1998 before the era of targeted disease-modifying antirheumatic drugs (DMARDs), including biologics.5,6 Since that time, specific questionnaires have addressed patients’ safety competencies regarding medications such as biologics.15 However, new issues have arisen for patients with SpA, such as comorbidities,16 cardiovascular (CV) medication risks,17,18 physical activity,19 social or professional issues,20 adherence,21 and more generally, changes in disease management that HCPs should communicate to patients as part of their comprehensive support.22
In this context, the aim of the present study was to develop and validate the Spondyloarthritis Knowledge (SPAKE) questionnaire, a new knowledge questionnaire for patients with axial SpA (axSpA), in order to meet the significant changes that have occurred since 1998 in the management of axSpA, such as the availability of targeted DMARDs,5,6 the consideration of comorbidities and adapted physical activity,15-22 and the new educational needs identified for patients.7,10
METHODS
Construction of the questionnaire. The questionnaire was developed in 3 steps. In step 1, a list of knowledge items was extracted from the published questionnaire11 and from 2 unpublished questionnaires currently used in PE in France to select knowledge considered essential for patients with SpA to facilitate self-management.23 A Delphi process included rheumatologists, HCPs, and patients, and first enriched the list to items considered potentially useful. The list was then reduced to obtain the most important items. Participants in the Delphi rounds were enrolled on a voluntary basis from 13 multidisciplinary teams dealing with inflammatory arthritis in France. The rheumatologists and HCPs invited patients and peer-patient educators to participate.
In step 2, a final Delphi round selected a list of items considered essential, selected by more than two-thirds of the participants, and items considered useful, selected by more than half and less than two-thirds of the participants.
The first version of the questionnaire was derived from the results of the final Delphi round. It was elaborated by 2 rheumatologists and 1 rheumatology nurse. Each question in the questionnaire was matched with the corresponding item on the list. The questionnaire was designed for patients with axSpA-predominant features whether or not they had associated features of peripheral SpA, psoriasis (PsO), or inflammatory bowel disease (IBD).
The questionnaire was reformulated during a consensus face-to-face meeting involving 2 rheumatologists, 2 rheumatology nurses, and 1 patient research partner, who, together, checked the questionnaire for ease of understanding and relevance to the Delphi results.
The questionnaire underwent linguistic validation and cognitive debriefing by 10 patients. The completion time was noted. The questionnaire was then reviewed by the investigating centers to obtain the final version.
Translation. The original French questionnaire was translated into English through 3 independent forward translations (French to English) followed by 2 independent back translations (English to French), with reconciliation of the translated texts.24
Validation. Patients included in the validation study were recruited by 13 secondary or tertiary care rheumatology centers in France and by 1 private practice center. In addition, 8 of the participating centers were asked to test the reproducibility and the other 6 to test the sensitivity to change by including patients who were scheduled to participate in an educational session after completing the questionnaire.
The inclusion criteria checked by the rheumatologist or the rheumatology nurse were the following: patients aged ≥ 18 years, with a diagnosis of axSpA (fulfilling the 2009 Assessment of SpondyloArthritis international Society classification criteria)25,26 followed up in outpatient or inpatient care, and able to complete a questionnaire in French.
Data collection. A variety of data were collected at inclusion: sociodemographics (age, sex, family status, education level, socioprofessional status), disease and treatment characteristics (disease duration, current treatment, nonpharmacological treatment), type of follow-up, and patients’ information sources. Several self-administered questionnaires were completed: the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)27 for disease activity, the Arthritis Helplessness Index (AHI),28 the General Self-Efficacy scale (GSE),29 and the Beliefs about Medication Questionnaire (BMQ).30 The rheumatologist or rheumatology nurse reported his or her opinion of the patient’s level of knowledge about the disease and its treatments using numeric rating scales (0 = very poor level of knowledge, to 10 = very high level of knowledge).
Ethics. The study was approved by the local ethics committees (IRB00013412, CHU de Clermont-Ferrand IRB #1, IRB number 2022-CF002) with compliance to the French policy of individual data protection and declared to the Clermont-Ferrand (France) Advisory Committee on Information Processing in Material Research in the Field of Health and the French national data protection agency (CNIL, no. 15 863). Patients received oral and written information on the objectives of the study and gave signed informed consent to participate and consent to publish before entering the study.
Statistics. Sample size was determined according to the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN) guidelines (https://www.cosmin.nl/) as 100 subjects for internal consistency to ensure stability of the variance–covariance matrix, and 50 subjects for reproducibility.
Statistical analysis was performed with Stata 15 (StataCorp), with 2-sided type I error set at 5%. Continuous data were expressed as mean (SD) or as median (IQR) according to their statistical distribution (assumption of normality assessed using the Shapiro-Wilk test). Categorical variables were expressed as number of patients and associated percentages. In addition to these descriptive statistics, we also addressed the following psychometric properties.31,32 Acceptability was assessed based on data quality, which was considered good if < 5% of the data were missing for each item/question. Internal consistency was determined using the Kuder-Richardson α coefficient calculated from the good/bad responses (ie, considering the “I don’t know” responses as incorrect). Internal consistency α was described as follows: α ≥ 0.9 is excellent, 0.9 > α ≥ 0.8 is good, 0.8 > α ≥ 0.7 is acceptable, 0.7 > α ≥ 0.6 is questionable, 0.6 > α ≥ 0.5 is poor, and 0.5 < α is unacceptable. The following values were calculated: item difficulty (proportion of patients providing the correct answer for an item, noted as “p”), item variance (noted as “p [1-p]”), and item–test correlations (corrected item–test point-biserial correlation coefficients, also termed the “discrimination index”).33,34 Reproducibility was assessed by calculating the strength of agreement (for each item, the percentage of identical answers at test and retest for the same patient) and the κ coefficient, when taking into account true/false/I don’t know responses, and, subsequently, correct/incorrect responses. The κ coefficient, weighted using quadratic weights as appropriate, was used for categorical data (items) to determine the test-retest reliability for each item. For total scores, Lin concordance correlation coefficient was estimated. Agreement values were considered, again as per the usual recommendations, as poor (< 0.2), weak (0.2-0.4), moderate (0.4-0.6), substantial (0.6-0.8), or almost perfect (> 0.8).35 Reproducibility was tested at a 2-week interval. The patients were asked not to check their responses between the 2 assessments. Sensitivity to change was assessed by testing the total questionnaire score and each domain score before and after 1 patient face-to-face or patient-group education session delivered as part of routine care in the rheumatology departments. The results were expressed as Hedges effect size and 95% CIs. The relationships between patient characteristics and knowledge levels were evaluated by univariate analysis. The following statistical tests were carried out: a t test or Mann-Whitney U test to compare groups, and Spearman or Pearson correlation coefficients to analyze relationships between continuous variables. The coefficients were interpreted as follows: negligible (< 0.2), low (0.2-0.4), moderate (0.5-0.7), and high (> 0.7).36 In order to determine the most relevant characteristics associated with better knowledge, a multivariate linear regression was conducted on univariate significant variables with a particular attention to the multicollinearity by computing the variance inflation factor and using the Farrar-Glauber test.
RESULTS
Construction of the questionnaire. In step 1, 67 items were extracted from the existing questionnaires. The Delphi rounds included 104 rheumatologists, HCPs, and patients. In each Delphi round, participants were 8 to 12 rheumatologists, 12 patients including 2 peer-patient educators, and 11 to 14 HCPs, mostly nurses. The first Delphi round enriched the list to 265 items considered potentially useful. The list was then reduced to obtain the 59 most important items, of which 34 (58%) were not present in the former published questionnaire or were substantially modified.11,23
In step 2, the final Delphi round selected 42 items: 32 considered essential, and 10 considered useful.
Questionnaire content. The SPAKE questionnaire contains 42 questions, of which 32 questions are considered essential (short-form SPAKE) and 10 questions are considered useful (long-form SPAKE). The English version is in Table 1 and the scorings and the French version are in Supplementary Material S1 and S2 (available with the online version of this article). The questions (Q) are related to 6 domains: knowledge of disease (12 items, questions 1-8 and 33-36), pharmacological treatment (11 items, questions 9-16 and 37-39), nonpharmacological treatment (8 items, Q18-23 and Q40-41), comorbidity (1 item, Q17), self-care for pain and fatigue (4 items, Q24-27), and adaptive skills to psychosocial and professional issues and the healthcare system (6 items, Q28-32 and Q42). Compared with the published questionnaire,11 SPAKE includes new questions on the pharmacological strategy and biologic DMARDs (bDMARDs), self-care for fatigue, CV comorbidity, and adaptive skills such as the patient’s pathway, shared decision making, and psychosocial/professional issues. The questionnaire took a mean of 12 minutes (minimum 8, maximum 15) to complete.
SPAKE questionnairea.
Validation of population. The validation study included 130 patients from September 2016 to September 2018, 67 (51.5%) men, mean age 43.5 (SD 12.9) years, and median disease duration 8 years (IQR 3-16). Descriptive data are shown in Table 2.
Patient characteristics and opinions of health professionals.
Acceptability. There were no missing items in the questionnaire; thus, acceptability was good.
Total score and scores by domains. Scoring was in the range of 0 to 100, with higher scores indicating better knowledge. Mean (SD) total score was 71.6 (15.4) on the long-form SPAKE and 71.0 (14.8) on the short-form SPAKE. The median (IQR) scores of the long form and the short form were 74 (62-83) and 75 (59-83), respectively. Table 3 reports the responses, domain by domain. Scores tended to be higher in knowledge of disease (83, IQR 58-92), nonpharmacological treatments (88, IQR 75-100), and adaptive skills (83, IQR 67-100), and lower in CV comorbidity (28 [21%]) and pharmacological treatments (64, IQR 45-73).
SPAKE scoresa by domain and the corresponding questions in the 42-item (long-form) and 32-item (short-form) questionnaires.
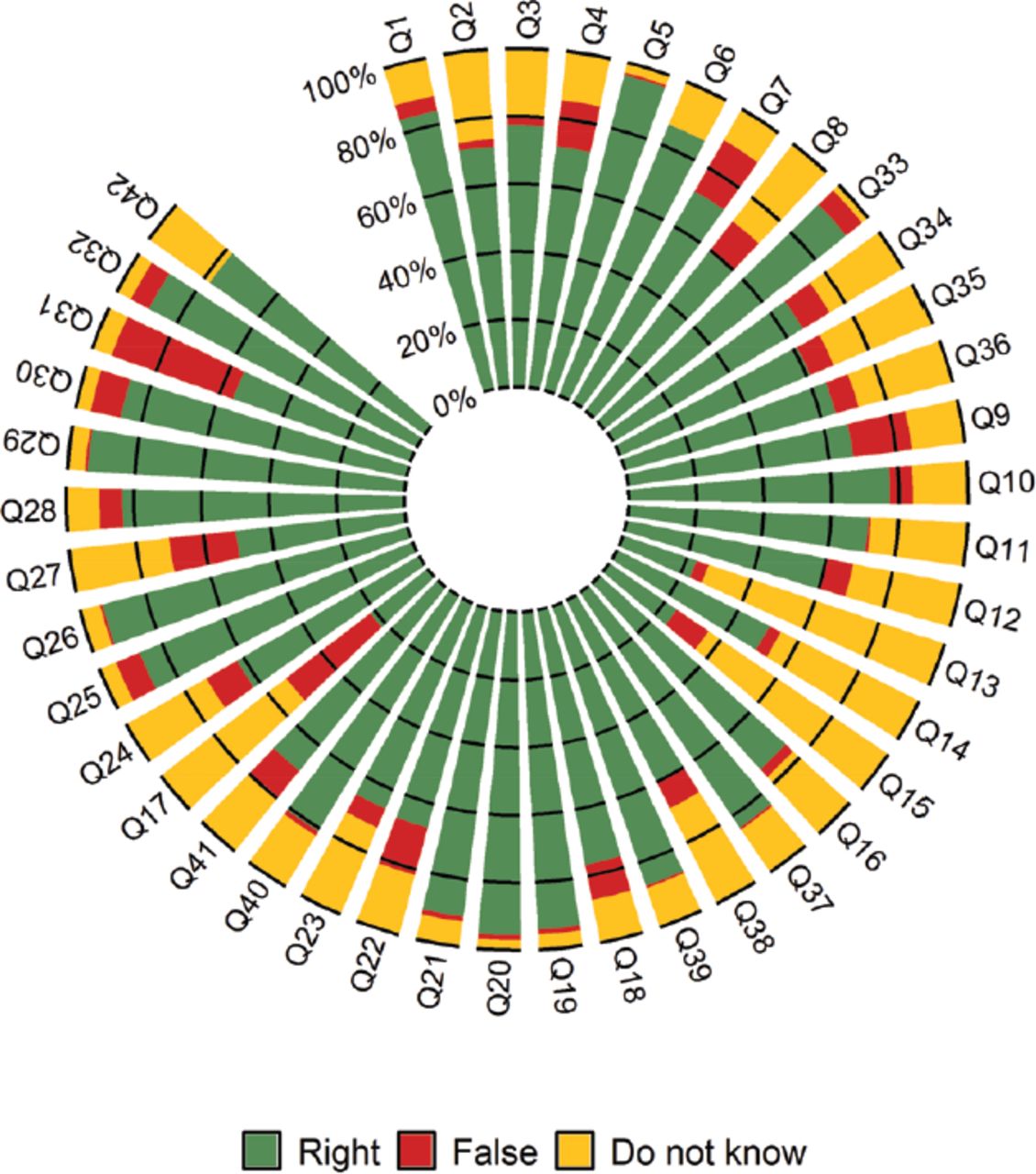
Scores per questions. The question-by-question distribution of responses (Figure) shows that the best knowledge (> 90%) was related to fatigue, which was considered a symptom of SpA (Q5) and not only related to lifestyle (Q26). Patients also had a good knowledge of the benefit of stretching exercises and of the importance of controlling efforts during sports practice (Q19, 20). They were also familiar with patient pathways (Q29) and professional issues such as workplace adaptations (Q32). Scores on bDMARDs were good, with a 77% good response rate for bDMARD management in case of fever or infection (Q10) and a 70% good response rate in case of planned surgery (Q11).

Scores per question. Q: question.
The highest rates of “I don’t know” responses concerned the safety of nonsteroidal antiinflammatory drugs (NSAIDs): to stop medication in case of black stools (Q13; 73% of “I don’t know” responses), not to take 2 NSAIDs concomitantly (Q14; 46% of “I don’t know” responses), and the need for blood pressure monitoring in patients taking NSAIDs (Q15; 64% of “I don’t know” responses). Similarly, the CV comorbidity (Q17) in SpA was unknown for 80% of patients (response of “I don’t know” or wrong answer) as was the fact that NSAIDs should be taken at the lowest possible dose, as long as they are effective (Q12; 53%).
Internal validation. The Kuder-Richardson α coefficient was 0.85 for the long-form SPAKE and 0.79 for the short-form SPAKE, indicating good internal consistency. The correlation between items and total long-form SPAKE score (item-retest correlation) varied between 0.14 and 0.50. The correlations between domains and total long-form SPAKE score are reported in Supplementary Material S3 (available with the online version of this article). The highest correlations (coefficient > 0.70) were found between the long-form score and the knowledge of disease (0.81) as well as pharmacological treatments (0.78), and the lowest correlation was found between the long-form score and comorbidity (0.36).The correlation coefficient between the long-form score and the short-form score was excellent at 0.98.
Reproducibility. Reproducibility was assessed in 61 subjects (descriptive data in Table 2). Lin concordance correlation coefficient was good for the long-form SPAKE score, at 0.81 (95% CI 0.72-0.89), and for the short-form SPAKE score, at 0.80 (95% CI 0.70-0.88). The concordances by domains are reported in Supplementary Material S4 (available with the online version of this article). Better reproducibility was found for knowledge of disease and treatments; whereas, self-care and adaptive skills had lower reproducibility. Of the 42 questions, 28 had a concordance rate of > 80%.
External validity. External validity was confirmed by a statistically significant correlation with the degree of information the patient had about his or her disease and treatment, as gauged by the doctor or nurse (r = 0.27 for both), as well as a significant correlation with the patient’s level of education (P = 0.004; Table 4). Correlation with patient-reported outcomes was low: r = 0.15 and r = −0.08 with the BMQ necessity scale and BMQ concern scale, respectively, r = 0.07 with the GSE, and r = −0.05 with the AHI (data not shown).
Long-form SPAKE score according to patient characteristics (univariate analysis).
Sensitivity to change. Sensitivity to change was measured in 53 patients (descriptive data in Table 2). There was a statistically significant difference in total score before and after PE sessions: mean value from 69.2 (SD 15.3) to 82.7 (SD 14.0; P < 0.001); Hedges effect size was 0.92 (95% CI 0.52-1.31). Domain-by-domain results are reported in Table 5. The domains with higher progression were CV comorbidity and pharmacological treatments, for which scores increased from mean value 14.5 (SD 35.6) to 49.1 (SD 50.4) and from 58.5 (SD 21.6) to 80.2 (SD 20.1), respectively.
Sensitivity to change. Correct response rate before and after patient education.
Association between patients’ variables and knowledge levels in SPAKE. Table 4 reports the factors associated with knowledge levels in the long-form SPAKE.
In the multivariate analysis, the patients’ relevant characteristics independently associated with a better knowledge were: sex (female vs male: odds ratio [OR] 5.8, 95% CI 0.8-10.8, P = 0.02), grade level (> high school vs ≤ high school: OR 5.3, 95% CI 0.2-10.3, P = 0.04), how well informed the patient was according to the opinion of the rheumatologist or the nurse (OR 2.3, 95% CI 0.8-3.7, P = 0.002), and PE sessions (yes vs no: OR 7.9, 95% CI 1.7-14.2, P = 0.01). No correlation was found with age or disease duration (data not shown).
DISCUSSION
This study reports the development and the validation of the SPAKE, a knowledge questionnaire for patients with axSpA. The SPAKE showed good acceptability with no missing responses, good internal and external consistency, good reproducibility, and a high sensitivity to change assessed before and after PE sessions.
The questionnaire was developed with the input of HCPs and patients who determined the knowledge essential for patients with axSpA to manage their health. Compared with the existing literature,11,12 SPAKE is the only knowledge questionnaire, to our knowledge, developed in over 20 years and is in line with current recommendations for SpA management.5,6
The SPAKE was designed to assess the knowledge of patients with axSpA. SPAKE is not appropriate for patients with SpA with predominant peripheral joint involvement and with skin or intestinal involvement such as psoriatic arthritis or IBD, because the questionnaire does not contain any specific questions on cutaneous or gut symptoms. Including numerous questions on extrarheumatic symptoms would have been inappropriate for most patients with axSpA, given that PsO is present in 4% to10% of patients with SpA, and IBD is also found in 4% to 10% of patients.37,38 Additionally, an important portion of the SPAKE is devoted to information on NSAIDs, which are rarely prescribed in IBD.
The SPAKE is in line with patients’ needs for knowledge in the era of targeted DMARDs, providing safety messages on pharmacological treatments, particularly bDMARDs. High scores were found on bDMARDs (77%) in a population containing 62% of patients treated with bDMARDs. This may be a result of bias in recruitment performed in hospital rheumatology departments in France, where PE is focused on safety skills related to targeted DMARDs. Conversely, the study shows that basic knowledge on NSAIDs was lacking, indicating that HCPs should be attentive to warning patients about the risks of intestinal bleeding, hypertension, and related CV diseases.39,40 In addition, the overall increased risk of CV diseases in SpA was not well known, although it is well documented.16,40 The SPAKE allows the detection of unmet educational needs regarding these comorbidities41 or drug-related issues. As expected, the SPAKE did not correlate with the psychological status (GSE, AHI) and the BMQ, which have other determinants such as health beliefs and medication adherence.28-30 It correlates with PE sessions which means that patient knowledge can be improved as recommended.3,4
Higher scores were obtained for nonpharmacological treatments. However, the SPAKE contains more questions on physical activity, in accordance with new recommendations,19 such as information on types of exercise and advice on how to manage pain occurring during exercise. The questionnaire contains information on self-care that is particularly focused on fatigue.
Other domains of the questionnaire include adaptive skills. This domain is original to the questionnaire, resulting from the selection of key messages by patients and HCPs. The formulation of the questions often appeared to be commonplace and intuitive. However, the designers chose to retain these elements, considering that a knowledge questionnaire is not merely an assessment tool but also an educational tool that can favor communication between the patients and HCPs as part of the educational process.3
The strengths of this study include the multicentric validation and the high level of patient involvement in the development of the questionnaire. This was not the case for the existing questionnaires,11,12 which were developed by HCPs only, validated by a smaller number of patients, and for which reproducibility was not evaluated. Our present study also included the psychometric validation in line with the recommended guidelines and the simultaneous validation of a short-form version of the questionnaire, which will be easier to use in current practice. The short form can be used by rheumatology nurses in the routine detection of the patients’ educational needs, whereas the long form can be dedicated as an educational and assessment tool in structured educational programs.
Limitations include a potential cultural bias, since the development resulted from Delphi rounds conducted only in France. The SPAKE was not specifically designed for people with low literacy, which is another limitation. Additional educational strategies for knowledge assessments will be needed for these patients. One limitation is also related to the involvement of patients and nonmedical HCPs. Some of them were not perfectly aware of previous recommendations. Consequently, the role of tobacco consumption did not appear in the SPAKE, although it is a determinant of SpA onset and disease activity42 and is negatively associated with responses to bDMARDs.43 Therefore, we believe that HCPs must be aware of this significant limitation and discuss tobacco cessation in addition to the SPAKE.44 Further steps will be needed, such as knowledge assessment in cohorts of patients with axSpA to improve information strategies toward the patients. The evaluation of HCP knowledge is also interesting because the competencies of HCPs should be promoted and monitored.4
In conclusion, SPAKE is a knowledge questionnaire for patients with axSpA, developed with the involvement of HCPs and patients. It may be valuable in meeting patients’ educational needs regarding essential self-management knowledge. It may also be useful in improving the information content delivered by HCPs and in assessing knowledge acquisition and self-management strategies in routine care and research.
ACKNOWLEDGMENT
This study is an initiative by the French Rheumatology Society Therapeutic Education Group. The authors thank the patients and HCPs who participated in the Delphi rounds and in the development of the questionnaire, and all the centers and their patients who participated in the questionnaire validation tests. We thank José Osorio y Fortea, Stéphanie Young, and Nicolas Valeyrie for their participation in the translation of the SPAKE.
Footnotes
The study was supported by an institutional grant from the University Hospital of Clermont-Ferrand (Centre Hospitalier Universitaire Gabriel-Montpied, Clermont-Ferrand, France; reference AOI RODERE 2016).
CB has received research grants from BMS, Fresenius Kabi, Eli Lilly, and Mylan; advisory board fees from Novartis and Sandoz; and speaker fees from BMS, AbbVie, MSD, Mylan, Pfizer, Roche, Sanofi, and UCB. TP has received speaker and consulting fees from AbbVie, Amgen, Biogen, BMS, Celgene, Fresenius Kabi, Janssen, Eli Lilly, MSD, Nordic Pharma, Novartis, Pfizer, Sandoz, Sanofi, and UCB. CS has received consulting fees from AbbVie, UCB, Eli Lilly, Nordic Pharma, GSK, Roche Chugaï, and BMS. DW has received speaker fees from AbbVie, BMS, MSD, Pfizer, Chugaï, Nordic Pharma, UCB, Novartis, Eli Lilly, Amgen, Grunenthal, and Galapagos; advisory board fees from Novartis, Janssen, AbbVie, and Amgen; and support for attending meetings from MSD, Galapagos, Chugaï, UCB, Mylan, and Fresenius Kabi. FC has received consulting and/or speaker fees from Eli Lilly, Novartis, and UCB. LG has received research grants from Amgen, Galapagos, Janssen, Eli Lilly, Pfizer, Sandoz, Sanofi; and consulting fees from AbbVie, Amgen, BMS, Biogen, Celgene, Galapagos, Gilead, Janssen, Eli Lilly, Novartis, Pfizer, Samsung Bioepis, Sanofi-Aventis, and UCB. The remaining authors declare no conflicts of interest.
- Accepted for publication July 6, 2022.
- Copyright © 2023 by the Journal of Rheumatology
This is an Open Access article, which permits use, distribution, and reproduction, without modification, provided the original article is correctly cited and is not used for commercial purposes.








{kind=link}