

Abstract
The majority of patients with systemic lupus erythematosus (SLE) have cutaneous manifestations at some point in their disease course. The skin findings in SLE are classified as SLE-specific or SLE-nonspecific based on histopathologic findings. SLE-specific skin diseases include chronic cutaneous lupus erythematosus (CLE), subacute CLE, and acute CLE. There are subsets of skin lesions within each group and the likelihood of associated SLE varies among them. SLE-nonspecific lesions are more common in patients with SLE and tend to coincide with active systemic disease. SLE-nonspecific lesions may be seen as a feature of another disease process, including other connective tissue diseases. It is important for the rheumatologist to be familiar with the spectrum of cutaneous diseases in SLE to help prognosticate the likelihood of systemic disease and to ensure patients receive timely dermatologic care with the goal of controlling disease activity to prevent damage.
Lupus erythematosus (LE) is a complex autoimmune disease entity with heterogeneous cutaneous and systemic manifestations that can evolve over the course of disease. The skin is the second most frequently affected organ system in systemic lupus erythematosus (SLE), with cutaneous manifestations occurring in 70% to 85% of individuals over the course of the disease and as a presenting symptom in up to 25% of patients.1 In the 1960s before autoimmune serology became generally available, skin changes were said to be the second most common presenting clinical manifestation of SLE.2 Skin disease carries a significant burden in terms of psychosocial well-being and medical costs. Patients with cutaneous lupus erythematosus (CLE) have similar or worse emotional components of quality of life than patients with hypertension, congestive heart failure, and type 2 diabetes mellitus.3 Population-based studies in the United States and Europe report an incidence of CLE of 3 to 4 per 100,000, with a prevalence of 70 per 100,000, whereas the incidence of discoid lupus erythematosus (DLE) is estimated at 0.8 to 3.7 per 100,000.4-9 These numbers are comparable to recent incidence and prevalence rates for SLE in the US.10
Classification of SLE and CLE
A brief review of the classification criteria of SLE and CLE is included to frame the discussion of cutaneous involvement in SLE. Importantly, these criteria are designed for research purposes and not intended to diagnose individual patients.
Four of the 11 criteria in the 1997 American College of Rheumatology (ACR) diagnostic criteria for SLE are cutaneous features of disease, including malar rash, discoid rash, photosensitivity, and oral ulcers.11,12 Based on these criteria, patients can be classified as having SLE with only skin manifestations that are not exclusive for SLE (photosensitivity is a typical feature of dermatomyositis [DM]); therefore, these diagnostic criteria may skew diagnosis and fail to distinguish CLE from SLE.13 The 2019 European Alliance of Associations for Rheumatology (EULAR)/ACR classification criteria for SLE include positive antinuclear antibodies (ANA) followed by additive weighted criteria in 7 clinical and 3 immunologic domains; patients accumulating > 10 points are classified as having SLE. Mucocutaneous is one of the 7 clinical realms, and includes alopecia (2 points), oral ulcers (2 points), subacute CLE (SCLE) or DLE (4 points), and acute CLE (ACLE; 6 points).14 One study, requiring ANA positivity according to the EULAR/ACR criteria, excluded 7.5% of patients with CLE previously diagnosed with SLE, some of whom had internal organ involvement including cytopenia, proteinuria, and/or inflammatory arthritis.15 The Systemic Lupus Collaborating Clinics (SLICC) criteria classify a patient as having SLE if they have biopsy-proven lupus nephritis with positive ANA or anti-dsDNA antibodies or at least 4 out of 17 criteria including at least 1 immunologic criterion and 1 clinical criterion.16 Four of the clinical criteria are mucocutaneous in nature including ACLE, chronic CLE (CCLE), oral ulcers, and nonscarring alopecia.16
No universally accepted classification criteria exist for CLE. Skin lesions in patients with SLE are divided according to the most widely used criteria suitable for rheumatologists in everyday clinical practice proposed by Gilliam and Sontheimer, which divides CLE into LE-specific and LE-nonspecific skin conditions.17,18 Other classification criteria, such as the Duesseldorf Classification, have been developed but have not gained universal acceptance.19 LE-specific skin conditions include CCLE, SCLE, and ACLE as well as their various subtypes (Figure 1). Although lupus erythematosus tumidus (LET) is considered by some as a form of CCLE, it is recognized by the Duesseldorf Classification and European S2k guidelines as a fourth primary subset of CLE known as intermittent CLE (ICLE).20,21 These LE-specific conditions have distinct clinical morphologies, but similar histopathologic features on routine H&E staining. These histologic features include lichenoid interface dermatitis with basal layer vacuolization, apoptotic keratinocytes, periadnexal and perivascular mononuclear cell infiltrate, epidermal atrophy, and basement membrane thickening (Figure 2).15 In DLE, there is a tendency for more hyperkeratosis, follicular plugging, and thickening of the basement membrane relative to ACLE or SCLE. However, not all these features are found in all forms of LE-specific variants, and they can be found in conditions other than CLE. Interface dermatitis, which consists of liquefactive degeneration of the epidermal basal layers, is not typically associated with LET or lupus erythematosus panniculitis (LEP) but is often seen in DM.22,23 A biopsy is recommended to confirm the diagnosis of CLE, as there are a variety of other diseases that mimic its variants (Figure 3).

Typical CLE lesions. (A) Active DLE lesions with erythema and scale are shown along with areas of damage (ie, dyspigmentation and scarring) from prior active lesions. (B) Erythematous DLE lesions are shown on the leg. (C) Annular SCLE lesions are seen on the arm and chest as well as (D) the legs. CLE: cutaneous lupus erythematosus; DLE: discoid lupus erythematosus; SCLE: subacute cutaneous lupus erythematosus.

This biopsy demonstrates the vacuolar interface dermatitis found in most LE-specific skin conditions. LE: lupus erythematosus.

Careful clinical examination is often required to distinguish CLE from dermatomyositis. (A) Dermatomyositis of the hands often shows confluent erythema of the skin overlying the MCP and IP joints and the extensor tendons while (B) DLE lesions are less likely to be localized to these areas and can resolve with scarring. Involvement of the v-area of the neck can appear very similar in (C) dermatomyositis and (D) CLE and requires clinical correlation with other areas of involved skin to arrive at the correct diagnosis. CLE: cutaneous lupus erythematosus; DLE: discoid lupus erythematosus; IP: interphalangeal; MCP: metacarpophalangeal.
LE-specific skin disease
As mentioned above, CLE is divided into the following primary subsets: ACLE, SCLE, CCLE, as well as ICLE in certain classification systems (Table 1). It is possible for patients to have more than one form of CLE. A study of 191 patients with CLE showed that 68% had 1 type, 29% had 2 types, and 3% had 3 types.24 A US population-based study showed that 12% of patients with CLE had disease progression to SLE, with a mean time to progression of 8 years.7 The cumulative incidence of SLE among patients with a diagnosis of CLE in the same study was 5% at 5 years, 10% at 10 years, 15% at 15 years, 19% at 20 years, and 23% at 25 years.7 Early recognition of patients with CLE who are at risk for developing SLE is important. Signs of nephropathy, elevated ANA titers, serositis, and arthralgias/arthritis or other new symptoms of systemic disease may suggest transition into SLE and should be closely followed. Patients with localized DLE, hypertrophic LE, LEP, and LET are more likely to have skin-limited LE; those with generalized DLE or SCLE often meet ACR criteria for SLE; and those with ACLE or LE-nonspecific skin lesions are most likely to have systemic disease.25
LE-specific skin disease.
CCLE. CCLE has several subtypes, including DLE (Figure 1A), LEP, LET, and chilblain LE.26 CCLE is notable for demonstrating a chronic, recurrent disease course which typically requires long-term treatment with potential for progression to involve internal organs.27,28 DLE is the most common subtype of CCLE, representing 50% of cases.28 DLE is considered localized if it involves exclusively the head and neck area and generalized if it extends below the neck with a predilection for the upper extremity extensor surfaces.28 Generalized DLE is more often associated with SLE, and patients with generalized DLE or progressive localized DLE should be reevaluated for progressive systemic disease.25 Both localized and generalized DLE consist of erythematous and sometimes scaly plaques in sun-exposed areas that progress to dyspigmentation and scarring.28 A recent study to develop classification criteria for DLE determined that clinical variables including atrophic scarring, location in the conchal bowl, and preference for the head and neck were most important, with lower importance given to dyspigmentation, follicular hyperkeratosis and/or plugging, and erythematous to violaceous color.29 Early in the disease course, prior to the development of damage, it can be difficult to differentiate DLE from SCLE since SCLE can also cause dyspigmentation that can mimic scarring. Careful attention to loss of skin markings including follicular openings is required to establish that scarring is present. Hypertrophic or verrucous DLE is characterized by papular lesions that tend to occur on the face, extensor surfaces, or palms and soles.28 Mucosal DLE typically presents as erosions or macules that can have radiating striae located in the lips, palate, gingiva, or other mucosal surfaces.30 LEP, also known as lupus profundus, presents as indurated subcutaneous nodules or plaques that tend to occur in the face, scalp, upper torso, buttocks, and proximal extremities. These lesions can progress to ulceration or subcutaneous atrophy.30 A biopsy shows lobular panniculitis, and it is important to confirm the diagnosis as the differential includes subcutaneous panniculitic-like T-cell lymphoma.25 Approximately 50% of patients with LEP will also have DLE skin lesions visible at the overlying skin surface. As mentioned above, LET is considered by European S2k guidelines to be a fourth primary subset of CLE, that is, ICLE.21 LET lesions tend to occur on the face, neck, upper chest, and shoulders, and consist of erythematous macules, papules, and plaques, normally with smooth surfaces and no scale.31 Compared to other variants of CCLE, LET is particularly photosensitive and less likely to be associated with SLE.25 However, there is a mucinous form of SLE with a skin biopsy identical to LET that can be seen in patients with SLE.32 Chilblain LE affects cold-exposed areas, particularly the acral surfaces, with painful, violaceous plaques and nodules that may progress to erosions or ulcerations.31 At some point in their disease course, 20% of patients with chilblain LE develop features of SLE.33
SCLE. SCLE is believed to occur in 10% to 15% of patients with SLE.1 Up to 50% of patients with SCLE meet diagnostic criteria for SLE, but systemic symptoms are typically arthritis/arthralgias, malaise, and myalgias, with internal organ involvement such as renal or nervous system disease occurring in less than 10%.4,27 Seventy percent of patients with SCLE are anti-Ro/SSA positive and 70% to 80% are ANA positive.34 Children of women who have SSA or SSB antibodies during pregnancy should be carefully monitored as they are at increased risk of neonatal LE.35 Histologically, SCLE is frequently characterized by a less dense infiltrate than in DLE, but a denser perivascular infiltrate than found in ACLE. Other histologic features include notable atrophy of the epithelium, and more significant vacuolization at the dermal-epidermal junction than in ACLE.28 Dust-like particles representing IgG binding to keratinocytes are a specific, but not sensitive, finding on direct immunofluorescence.36 The 2 forms of SCLE include the annular and papulosquamous subtypes, both of which are notable for a recurrent course of widespread, highly photosensitive lesions.28 Lesions tend to be distributed symmetrically in sun-exposed regions, though the central face, scalp, and skin below the waist are typically spared.28,31 Lesions usually resolve without scarring, though dyspigmentation may occur.31 Some patients exhibit features of both subtypes.31 Annular SCLE presents with scaly annular erythematous plaques, which often merge to form a polycyclic morphology.31 Papulosquamous SCLE can resemble psoriasis or eczema.31 Erythrodermic LE and LE gyrates repens are considered rare variants of SCLE.28 Erythrodermic LE presents with generalized exfoliative erythroderma that may represent a flare of papulosquamous SCLE after sun exposure.28 Only a few cases of LE gyratum repens have been discussed in the literature, and they typically manifest as widely distributed chronic and recurrent figurate erythematous plaques.28 Although most cases of SCLE are idiopathic, up to one-third of cases are believed to be induced by exposure to drugs. The most common causes of drug-induced SCLE are proton pump inhibitors (PPIs), antihypertensives (especially thiazide diuretics and calcium channel blockers), anticonvulsants, and antibiotics.37,38 Recently, cases of patients with preexisting SLE who subsequently developed SCLE after exposure to antihypertensives or PPIs have been described.37 It should be noted that patients with SLE on systemic corticosteroids are often placed on PPIs prophylactically to prevent gastrointestinal side effects. Adding to the risk of drug-induced SCLE are several over-the-counter forms of PPIs that are now available to the public in the US. Particularly relevant to the rheumatologist is the potential for biologic therapies including TNF-α inhibitors, interleukin (IL)-17 inhibitors, IL-12/23 inhibitors, and cytotoxic T-lymphocyte associated protein 4 therapy to induce SCLE.39-42 Rowell syndrome is an entity that can be associated with SLE, DLE, or SCLE, in which patients develop erythema multiforme-like lesions and have a speckled ANA pattern.25 Sjögren syndrome is often a concomitant autoimmune disorder found in patients with SCLE and is more commonly associated with SCLE than other CLE subtypes.43
ACLE. ACLE is believed to occur in 30% to 50% of patients with SLE.1 Systemic involvement is typical and ACLE rashes often flare in parallel with other organ disease activity.31 Ninety-five percent of patients with ACLE have positive ANA.34 Histologically, ACLE lesions show liquefactive degeneration of the basal layer, an interface dermatitis, with perivascular and periadnexal lymphocytic infiltrate. There are localized and generalized forms of ACLE. The localized form of ACLE is the malar rash, characterized by butterfly-shaped erythema over the cheeks and nasal bridge that tends to spare the nasolabial folds, as opposed to DM which typically involves nasolabial folds (Figure 4). The malar rash can be raised or flat, may be associated with a fine scale, and is classically sun-induced, nonscarring, and transient. The less common generalized form of ACLE, sometimes called a maculopapular lupus rash or photosensitive lupus dermatitis, occurs above and below the neck and presents as a widespread eruption of macules and papules that is photosensitive and often pruritic. The pattern of involvement on the dorsum of hands can help distinguish generalized ACLE from DM; the metacarpophalangeal and interphalangeal joints are normally spared in ACLE.31 Less common presentations of ACLE include involvement of the lips and periorbital edema. Rare cases of toxic epidermal necrolysis (TEN)-like ACLE or hyperacute CLE have been reported, which encompasses clinical and histological findings of both ACLE and toxic epidermal necrolysis together without an inciting drug or infection.44,45 The majority of patients have a previously confirmed or new diagnosis of SLE or SCLE at the time of TEN-like ACLE.46
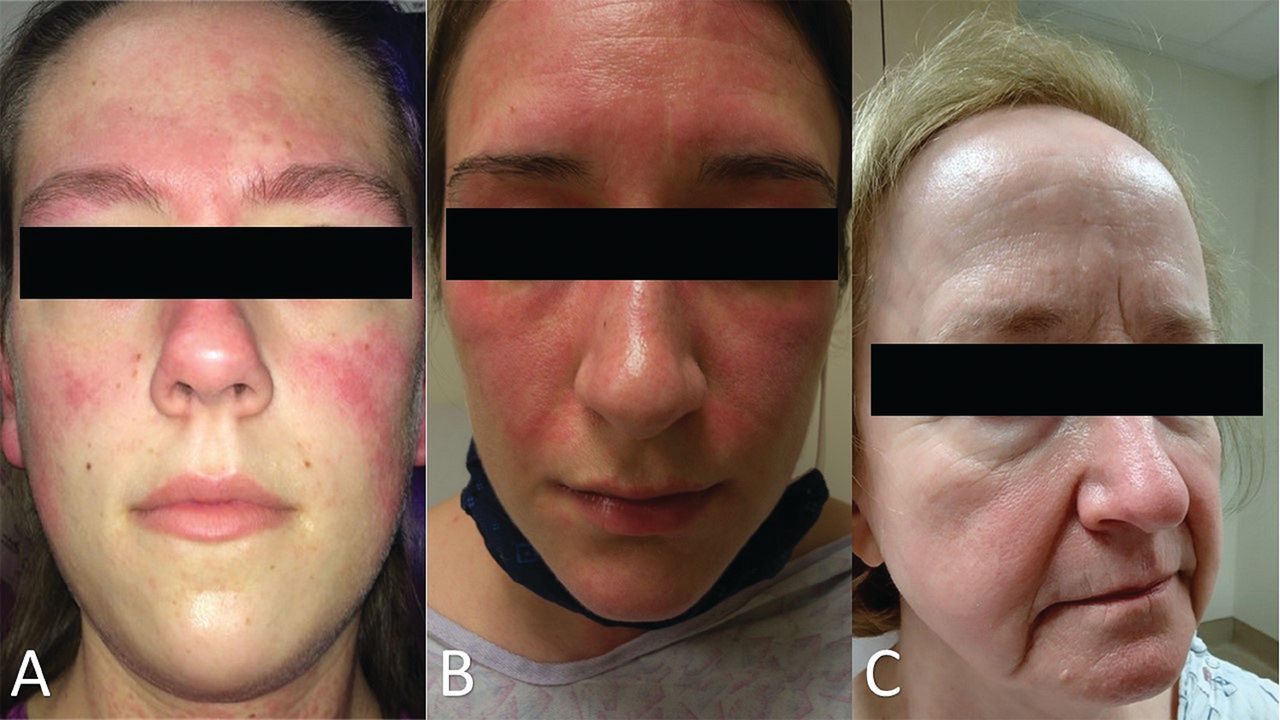
A “butterfly rash” may be due to a variety of dermatological conditions. (A) The malar rash of ACLE refers to erythema over the nasal bridge and cheeks that spares the nasolabial folds. Erythema of ACLE can be found in other areas of the face, such as the forehead here. (B) Facial erythema in dermatomyositis tends to involve the nasolabial folds. (C) Rosacea can mimic the facial erythema of ACLE but tends to worsen with specific triggers such as alcohol, heat, and spicy foods. ACLE: acute cutaneous lupus erythematosus.
LE-nonspecific skin disease
LE-nonspecific skin disease includes skin changes that are frequently associated with LE but are not specific to the disease itself (Table 2). LE-nonspecific skin lesions are common in patients with SLE and often occur during the active phase of disease. Compared to those with LE-specific lesions, those with nonspecific lesions tend to have increased SLE disease activity.47 In addition to vascular disease, which will be discussed in more depth below, other nonspecific cutaneous findings can occur in SLE including sclerodactyly, calcinosis cutis, rheumatoid nodules, urticaria, cutis laxa/anetoderma, acanthosis nigrans, lichen planus, and erythema multiforme. Bullous LE is considered a LE-nonspecific entity. Diagnosis of bullous LE requires an existing SLE diagnosis and patients frequently have increased SLE disease activity. Unlike the lymphocytic inflammation seen in SLE-specific lesions, the inflammation in bullous LE is neutrophilic, the blister is subepidermal, and an antibody against type VII collagen is seen in the blood. Skin biopsy shows linear IgG at the dermal-epidermal junction on direct immunofluorescence. Thus, a biopsy for direct immunofluorescence is helpful, and findings are distinguished from epidermolysis bullosa acquisita because of the diagnosis of SLE.48
LE-nonspecific skin disease.
Cutaneous vascular disease is a subtype of LE-nonspecific skin disease that includes vasculitis, vasculopathy, periungual telangiectasias, livedo reticularis, thrombophlebitis, Raynaud phenomenon (RP), and erythromelalgia. Cutaneous vasculitis has been reported in 10% to 20% of patients with SLE. It is a small vessel leukocytoclastic vasculitis that manifests as palpable purpura or urticarial vasculitis. Occasionally vessels in the deeper dermis and subcutaneous tissues can be involved, resulting in nodules or ulceration in a polyarteritis nodosa-like presentation. Cutaneous vasculitis is most common with increased SLE activity and is often associated with circulating immune complexes and hypocomplementemia. While vasculitic lesions are due to a primary inflammatory attack on the vessel wall, other vascular skin manifestations associated with SLE are the result of vasculopathy secondary to coagulation abnormalities, including, but not limited to, antiphospholipid antibody syndrome.49 Sometimes grouped as livedoid vasculopathy, these entities likely represent an inflammatory response because of hypercoagulability. Livedo reticularis, a bluish net-like pattern typically most prominent on the skin of buttocks, legs, and arms, results from reduced arterial blood flow and hypo-oxygenation and is common with cold exposure. Livedo racemosa, with an irregular, broken net-like pattern occurs with an underlying focal skin pathology such as thrombi or calcification.50 Other vascular related phenomena that occur in SLE include periungual telangiectasia and erythema in 10% to 15% of patients. RP, also common in other connective tissue disease such as scleroderma, DM, and mixed connective tissue disease, occurs in many patients with SLE and is characterized by cold-induced blanching followed by livedoid and erythematous color change of fingers and other acral skin. Nonspecific changes on nailfold capillaroscopy, including tortuous and dilated capillaries and hemorrhage, are more prevalent in SLE compared to healthy controls.51
Hair loss is frequent in SLE, occurring in more than half of patients at some point in the disease course (Figure 5).52,53 Nonscarring alopecia, defined as diffuse thinning and fragility of the hair in the absence of other causes, is seen in 40% to 70% of patients with SLE.16 It is important to rule out other potential causes of nonscarring alopecia before attributing it to SLE. Lupus hair refers to breakage of hair that typically occurs in the frontal scalp. It commonly occurs during disease flares and may be a form of telogen effluvium.
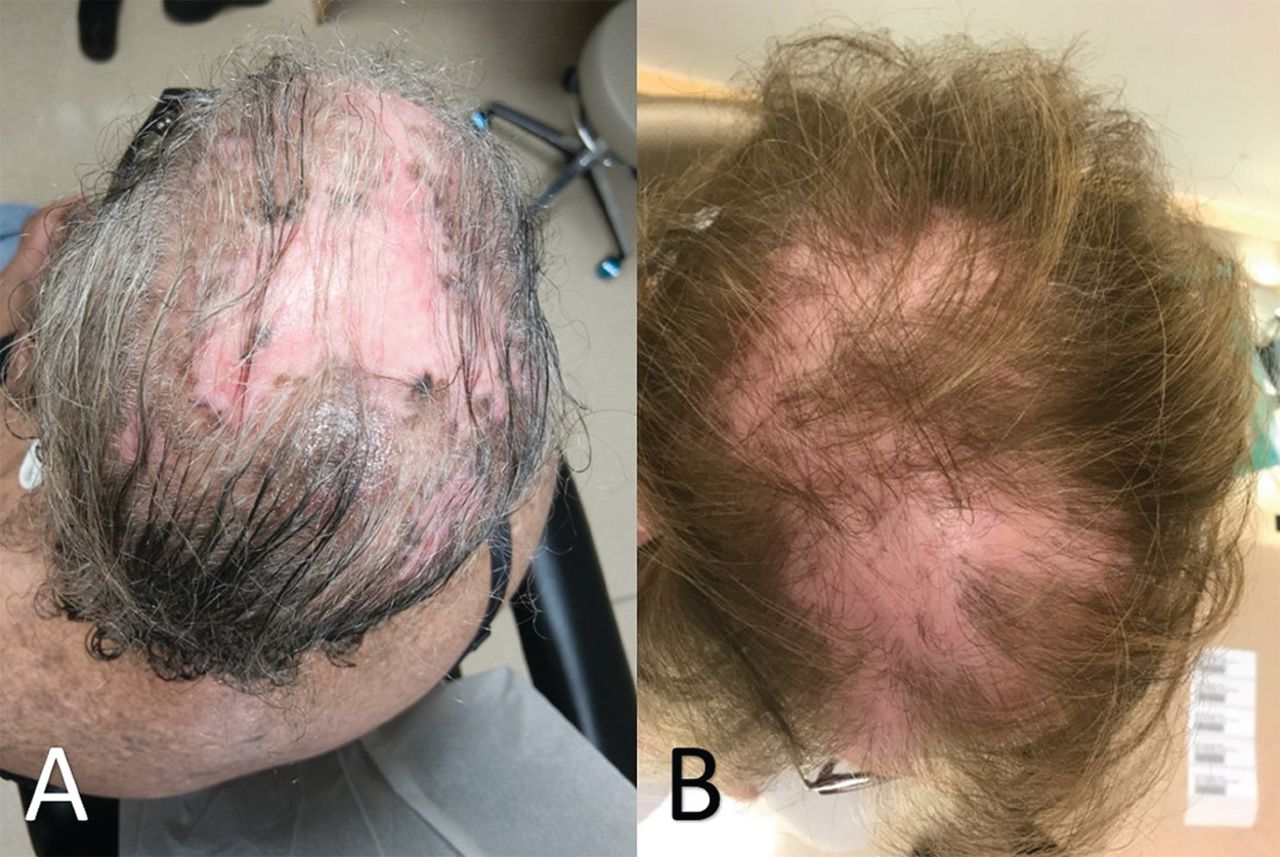
Alopecia due to (A) CLE can be difficult to distinguish from mimickers such as alopecia because of (B) lichen planopilaris; correlation between clinical and histologic findings may be required to correctly identify the cause of hair loss. CLE: cutaneous lupus erythematosus.
Finally, returning to the cutaneous features included in the 1997 ACR diagnostic criteria for SLE,12 2 of the 4 criteria that have not yet been discussed are photosensitivity and oral ulcers. Photosensitivity is a phenomenon whereby exposure to ultraviolet light causes skin rash in sun-exposed areas and/or other systemic symptoms of SLE flares. It is a clinical observation and occurs in a variety of other conditions, including DM, polymorphous light eruption, photoallergic contact dermatitis, solar urticaria, and porphyrias. Oral or nasopharyngeal ulcers occur in more than 40% of patients with SLE.54,55 Lesions can be painful or painless and while palatal ulcers are the most specific for SLE, ulcers can also occur on buccal mucosa, hard palate, and the vermilion border.
Disease monitoring
The differentiation between disease activity and damage is important in SLE and CLE, given the chronic nature of these diseases with periods of flares. The goal in managing SLE and CLE is to prevent and control activity in order to avoid damage, which is frequently irreversible. The Systemic Lupus Erythematosus Disease Activity Index (SLEDAI) and SLEDAI 2000 (SLEDAI-2K), tools used to assess disease activity and guide decisions to increase therapy, use a cut-off score of 3 to 4 to define active disease and include several cutaneous features. Both versions include alopecia (2 points), oral or nasal mucosal ulcers (2 points), vasculitis including ulceration, gangrene, tender finger nodules, periungual infarction, and splinter hemorrhages (8 points); the SLEDAI also includes “new rash,” defined as new onset or recurrence of inflammatory rash (2 points); and the SLEDAI-2K includes “rash,” defined as inflammatory rash (2 points).56,57 The SLICC/ACR Damage Index, used to assess damage over the course of disease, incorporates scarring chronic alopecia, extensive scarring of panniculum other than scalp and pulp space, and skin ulceration.58 Damage in the SLICC criteria is defined as an irreversible change not related to active inflammation that has occurred since the onset of disease and has been present for at least 6 months.
The Cutaneous Lupus Erythematosus Disease Area and Severity Index (CLASI) is a validated instrument that has separate scores to measure activity and damage of CLE. Activity scores are based on the extent of erythema, scale/hypertrophy, mucous membrane involvement, acute hair loss, and nonscarring alopecia. Damage scores are based on dyspigmentation and scarring, including scarring alopecia.59,60 Since the CLASI was developed and validated, it has been used in two-thirds of clinical studies and trials with CLE outcomes.61,62 Additional validated activity and damage scores for CLE have been developed. The revised CLASI includes adjustments to the original CLASI, such as new variables like edema/infiltration and subcutaneous nodules/plaques.61 A working core outcome set for CLE trials was recently developed to guide future clinical and outcomes research in CLE, recommending the CLASI as a primary endpoint and the Cutaneous Lupus Activity IGA (CLA-IGA) as a secondary endpoint for CLE physician-reported outcome measures.62
Treatment
As previously mentioned, the goal in the management of cutaneous manifestations of SLE is to prevent and treat skin activity to minimize damage. A treatment algorithm for CLE has been put forth in the European S2k guidelines.63 An essential component to managing cutaneous disease in SLE is prevention, with aggressive sun-protective measures including protective clothing, avoiding exposure during peak sunlight hours, and daily use of SPF 70 or higher broad-spectrum ultraviolet A/B sunscreens. Vitamin D supplementation should be considered in all patients, especially when serum levels are below normal range. Patients who use tobacco should be counseled on smoking cessation, as it has been identified as a risk factor for widespread CLE, it can increase disease severity, and it can decrease the efficacy of antimalarial therapy.64,65
Topical and intralesional corticosteroids can be used in limited cutaneous disease or as adjunctive therapy along with systemic agents. As with systemic steroid use, the goal is to use the least potent formula for the shortest amount of time to lower the risk of local complications such as steroid atrophy and telangiectasia. An initial regimen of a medium-strength (class III) topical corticosteroid such a triamcinolone acetonide 0.1% applied daily to lesional skin can be tried, especially on areas off the face. If this does not provide sufficient relief, a more potent topical steroid such as clobetasol propionate 0.05% or betamethasone dipropionate 0.05% (class I) should be considered. When class I to III topical corticosteroids are providing clinical benefit in sensitive areas such as the face, one can minimize the chances for developing cutaneous atrophy from longer-term therapy by rotating the topical corticosteroid every 2 weeks with a topical calcineurin inhibitor such as pimecrolimus cream or tacrolimus ointment.5 Calcineurin inhibitors are recommended as alternative first-line or second-line topical therapeutic options, especially for the face, on the basis of randomized clinical trials.63
Antimalarials (hydroxychloroquine, chloroquine, and quinacrine) are first-line therapies for cutaneous disease in SLE. Seventy-five percent of patients respond to antimalarials with or without the addition of topical glucocorticoids.66 Disease refractory to antimalarials can be treated with immunosuppressives common in the rheumatologists’ armamentarium, including methotrexate (MTX), mycophenolate mofetil (MMF), or azathioprine (AZA), although AZA is frequently less effective.67 Though the algorithm suggested in the European guidelines lists MTX as a second-line therapy and MMF as a third-line, there have been limited controlled trials in treating refractory CLE; therefore, the European guidelines were based on a consensus conference of dermatologists rather than being an evidence-based statement.67 A recent cohort study suggests similar efficacy for MTX and MMF between subtypes of CLE, suggesting that other factors such as side-effect profile and comorbid conditions may influence medication selection.68 Thalidomide is recommended only in treatment-refractory CLE with careful monitoring for the development of polyneuropathy, a potential adverse effect.63 Another therapeutic option for patients refractory to antimalarials is lenalidomide, a thalidomide analog with a superior adverse effect profile to thalidomide.69 Dapsone can be effective in the treatment of bullous LE, LEP, and in some cases of SCLE and DLE; use requires close monitoring for hematologic toxicities and the drug should not be used with patients who have a glucose-6-phosphate dehydrogenase deficiency. Three case series showed significant improvement in CLASI activity scores with belimumab.70-72 ACLE can respond favorably to rituximab; however, no beneficial effects and some exacerbations or new-onset disease have been seen in patients with DLE or SCLE.73-75 Anifrolumab, a drug recently approved by the US Food and Drug Administration for SLE, was shown in a phase III trial to be superior to placebo in improving skin disease measures in patients with at least moderately active skin disease.76 Multiple agents are also under investigation as alternative therapies for CLE. Iberdomide has been shown in a recent phase II trial to have beneficial effects on skin disease in patients with SCLE and CCLE, but not ACLE. BIIB059, a humanized monoclonal antibody targeting BDCA2 on plasmacytoid dendritic cells (pDCs), was shown to improve skin disease activity in patients with CLE in a recent phase II trial.77,78 Similarly, VIB7734, a monoclonal antibody that targets pDCs for antibody-dependent cellular cytotoxicity, showed clinically significant improvement in measures of skin disease activity in patients with CLE in a phase I trial.79
Conclusion
The spectrum of cutaneous disease in SLE is extremely broad and can occur at any point in the disease. Collaboration between dermatology and rheumatology specialists is essential to properly diagnose and manage affected patients. Skin biopsy is important to differentiate CLE from other skin conditions and must be considered in clinical context to reach a diagnosis. Timely and appropriate therapy to control activity and minimize damage is the goal of treatment.
Footnotes
This work was supported by the US Department of Veterans Affairs (Veterans Health Administration, Office of Research and Development and Biomedical Laboratory Research and Development) and the National Institutes of Health (R01AR071653).
The authors declare no conflicts of interest relevant to this article.
- Accepted for publication August 25, 2022.
- Copyright © 2023 by the Journal of Rheumatology
This is an Open Access article, which permits use, distribution, and reproduction, without modification, provided the original article is correctly cited and is not used for commercial purposes.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.
- 7.↵
- 8.
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.
- 41.
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.
- 72.↵
- 73.↵
- 74.
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}