

Abstract
Objective. The calcineurin inhibitor tacrolimus has been approved in Japan for the treatment of interstitial pneumonia (IP) in patients with polymyositis (PM) and dermatomyositis (DM). Postmarketing surveillance was initiated to examine long-term outcomes of immunosuppressive regimens containing tacrolimus in real-world settings.
Methods. Observational, prospective, postmarketing surveillance is ongoing in 179 patients with PM/DM-associated IP initiating treatment with tacrolimus. We report interim findings after 2 years of follow-up. Cumulative overall survival was assessed using Kaplan-Meier analysis. Potential prognostic factors for mortality were assessed by univariate Cox proportional hazards analysis.
Results. A total of 170 patients were included in this analysis. At the time of starting treatment with tacrolimus, almost all patients were receiving corticosteroids (98.8%), and cyclophosphamide was additionally used in 42 patients (24.7%). Forty-nine patients (28.8%) discontinued tacrolimus during follow-up, mainly due to loss to follow-up, patient death, and adverse events. Mean (SD) oral corticosteroid dose decreased from 32.4 (21.6) mg/day at baseline to 7.6 (4.2) mg/day at 2 years. Overall survival at 2 years was 90.3%; corresponding progression-free survival was 62.5%. Factors found to be associated with all-cause mortality included diagnosis of clinically amyopathic DM (hazard ratio [HR] 9.04, 95% CI 1.18-69.51 vs PM), ferritin level 500 to < 1500 ng/mL (HR 8.61, 95% CI 2.51-29.45 vs < 500 ng/mL), and presence of antimelanoma differentiation-associated gene 5 antibodies (HR 8.16, 95% CI 1.03–64.47 vs absence).
Conclusion. Immunosuppressive regimens containing tacrolimus appear useful for the management of IP in patients with PM/DM. [ClinicalTrials.gov: NCT02159651]
- dermatomyositis
- immunosuppressive agent
- interstitial lung disease
- polymyositis
- postmarketing product surveillance
Polymyositis (PM) and dermatomyositis (DM) are systemic autoimmune diseases characterized by chronic inflammation and weakness of the skeletal muscles.1 Patients with DM also have cutaneous manifestations.1 Interstitial lung disease (ILD), or interstitial pneumonia (IP), is a common manifestation of PM/DM, which is associated with increased risk of morbidity and mortality in patients with PM/DM.2,3,4 The reported prevalence of ILD in patients with PM/DM ranges from 20% to 78%.2 Corticosteroids are generally used as first-line therapy for the treatment of ILD in patients with PM/DM; however, many patients fail to respond adequately to corticosteroids alone and require additional immunosuppressive drugs.2,3
T cells are an essential treatment target for PM/DM-related ILDs. Further, CD25+/CD8+ T cells in bronchoalveolar lavage fluid are increased in patients with corticosteroid-resistant PM/DM-related ILD vs those in corticosteroid-sensitive patients.5 Tacrolimus, a calcineurin inhibitor, is a T cell-specific immunosuppressant with an inhibitory effect on T cell activation and cytokine production.6,7 Several retrospective studies have shown potential efficacy and safety of adding tacrolimus to usual immunosuppressive therapy in patients with PM/DM-associated ILD.8,9,10,11,12 In a recent prospective, multicenter, open-label study, significant improvement in lung function was observed over a period of 52 weeks in patients with PM/DM-associated ILD receiving tacrolimus in combination with corticosteroids as their initial immunosuppressive regimen; overall survival at 52 weeks was 88.0%.13 Adverse events (AEs) were consistent with the known safety profiles of tacrolimus and high-dose corticosteroids.13 Based on these results, tacrolimus was approved in 2013 for the treatment of ILD in patients with PM/DM in Japan. Postmarketing surveillance has been undertaken to prospectively assess safety and clinical outcomes over a period of 3 years in patients with PM/DM-associated ILD initiating treatment with tacrolimus in real-world clinical settings in Japan. We report interim findings at 2 years.
METHODS
Surveillance design and patients. This observational, prospective, postmarketing surveillance was conducted in patients with PM/DM-associated ILD initiating treatment with tacrolimus at 51 medical institutions across Japan between January 2014 and January 2017 (ClinicalTrials. gov: NCT02159651). PM/DM and clinically amyopathic DM (CADM) were classified according to the diagnostic criteria of Bohan and Peter14,15 and Sontheimer16, respectively. Patients were registered into a central registration system within 14 days of the start of treatment with tacrolimus. The planned total follow-up period is 3 years. This is an interim report of safety and clinical outcome data at 2 years after the start of treatment (data cut-off date, March 2020). Surveillance was conducted under routine clinical practice conditions in accordance with the ordinance for Good Post-marketing Study Practice (GPSP) issued by the Ministry of Health, Labour and Welfare. GPSP does not require the obtainment formal ethics committee approval from participating medical institutions or informed consent from participating patients. Written agreements with all participating medical institutions were executed prior to patient enrollment. To maintain privacy, all patient data were anonymized.
Tacrolimus treatment. In accordance with the prescribing information in Japan, tacrolimus was initiated at a dose of 0.0375 mg/kg twice daily, to be taken after the morning/evening meals, with a suggested target trough blood level of 5–10 ng/mL. Subsequently, the dosage could be adjusted on the basis of clinical signs and symptoms, and according to the patient’s tacrolimus blood concentration, up to a maximum daily dose of 0.3 mg/kg. There was no restriction on the use of concomitant drugs, including corticosteroids and cyclophosphamide (CYC). High-dose corticosteroids were defined herein as prednisolone equivalent ≥ 40 mg/day.17
Data collection. Patients were assessed at the time of initiation of tacrolimus treatment (baseline) and routine visits up to 36 months, and at the time of treatment discontinuation, if applicable. Data concerning patient baseline demographics and clinical characteristics, tacrolimus dose, whole blood trough concentrations, and use of concomitant corticosteroids and other immunosuppressants were collected. Definitions of acute/subacute ILD used in this study followed those used in related studies that were available at the planning of this study (2014),18 although there are more recent definitions available for reference.19 Laboratory tests, including testing for the presence of autoantibodies, were undertaken according to routine practice at each participating medical site. For detection of serum autoantibodies, validated ELISA were used.20,21,22
AEs were summarized in accordance with preferred terms from the Japanese version of the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use Medical Dictionary for Regulatory Activities (MedDRA/J; version 22.1). Adverse drug reactions (ADRs) were defined as AEs for which a causal relationship to treatment with tacrolimus could not be ruled out. An ADR was considered serious if it resulted in death, was life-threatening, required hospitalization or prolongation of existing hospitalization, or resulted in persistent or significant disability/incapacity. ADRs considered to be of special interest were cardiac dysfunction, renal impairment, impaired glucose tolerance, pancreatic dysfunction, infections, lymphoma, and psychiatric and nervous system disorders.
The primary clinical outcome was overall survival, defined as the time from initiation of tacrolimus to death due to any cause. Progression-free survival was also assessed, defined as the time from initiation of tacrolimus to disease progression or death due to any cause (whichever occurred first). Disease progression was defined as exacerbation of ILD as evidenced by any of the following : (1) ≥ 10% reduction in percent forced vital capacity (%FVC) from baseline23; (2) ≥ 15 mmHg increase in resting alveolar-arterial oxygen gradient (AaDO2) from baseline; (3) any exacerbation of at least equivalent severity to those defined above, including need for enhanced treatment for ILD; or (4) evidence of exacerbation on chest computed tomography (CT) or radiographs (compared with most recent data). Other secondary clinical outcomes included the following: respiratory function (assessed by %FVC and percent diffusing capacity for carbon monoxide [%DLCO]); arterial blood gas analysis (partial pressure of arterial oxygen [PaO2] and AaDO2); chest CT findings; and serum ferritin, Krebs von den Lungen 6 (KL-6), and surfactant protein D (SP-D) levels.
Statistical analysis. Categorical variables are shown as n (%) and continuous variables as mean (SD) or median (IQR). Survival rates were estimated using the Kaplan-Meier method; patients who dropped out or were lost to follow-up without events of interest were censored at subsequent assessments. Log-rank tests between subgroups stratified by baseline demographic and clinical characteristics were undertaken to identify potential prognostic factors associated with mortality. Univariate Cox proportional hazard models incorporating those factors as explanatory variables were also undertaken to estimate hazard ratios (HRs) with 95% CIs. Missing data were not imputed in any of the analyses. All analyses were performed using SAS statistical software (version 9.4; SAS Institute).
RESULTS
Patient population. A total of 179 patients were enrolled at 51 medical institutions (32 rheumatology departments, 17 pulmonology departments, and 2 dermatology departments) from January 2014 to January 2017. At the cut-off date for this interim report (March 2020), case report forms were available for a total of 171 patients, with safety and clinical outcome data available for 170 and 169 patients, respectively.
Baseline demographics and clinical characteristics are shown in Table 1. Female patients accounted for 68.8% of the total population, and mean (SD) age was 59.4 (12.4) years. The underlying disease was PM in 46 patients (27.1%) and DM in 124 patients (72.9%). Approximately half of the patients with DM had CADM. At the time of starting treatment with tacrolimus, 78.8% of patients had initial onset of ILD and 21.2% had relapse. Median disease duration at enrollment was 90 days in patients with initial onset and 920 days in those with relapse. The course of ILD was acute/subacute in 42.9% of patients, and the most common CT or histological finding was non-specific ILD (NSIP; 76.5%). Diffuse alveolar damage (DAD) was reported in 5 patients, all of whom were classified as having CADM.
Patient demographic and clinical characteristics at the time of initiation of tacrolimus treatment (safety analysis population).
Anti–Jo-1 and antiaminoacyl tRNA synthetase (anti-ARS) antibody testing, which was approved by the medical insurance system in Japan and available in clinical practice throughout the surveillance period, was performed in most patients (81.8% and 78.2%, respectively; Table 1). Of those tested, 19.4% were positive for anti–Jo-1 antibodies (34.2% with PM, 9.3% with CADM, and 19.1% with classic DM) and 55.6% were positive for anti-ARS antibodies (61.8% with PM, 40.0% with CADM, and 70.5% with classic DM). In contrast, testing for antimelanoma differentiation-associated gene 5 antibodies (anti-MDA5; previously known as anti-CADM 140) was not approved by the medical insurance system in Japan until 2017 and was conducted in only 50 patients at baseline. Anti-MDA5 antibodies were detected in 29 patients (58.0%), all of whom had DM.
Treatment regimen. Prior to initiating tacrolimus treatment, 3 patients with rheumatoid arthritis (RA) were receiving methotrexate, 1 patient with RA was receiving etanercept, and 1 patient was receiving azathioprine. The latter was discontinued 3 weeks before the start of tacrolimus treatment. Almost all patients (98.8%) were receiving corticosteroids at baseline (Table 1). CYC use at baseline was reported in 42 patients (24.7%), most commonly those with CADM. Twelve patients (7.1%) were receiving corticosteroid pulse + CYC (10 CADM, 1 classic DM, and 1 PM).
The mean (SD) dose of tacrolimus was 0.058 (0.024) mg/kg/day at baseline and increased to 0.067 (0.032) mg/kg/day at 1 week. Thereafter, tacrolimus dose was generally maintained and whole blood tacrolimus trough concentrations remained stable over the 2 years of follow-up, with mean tacrolimus trough levels ranging from 6 to 8 ng/mL (Figure 1). There was no difference in mean (SD) tacrolimus dose and whole blood trough concentration according to anti-MDA5 and anti-ARS antibody status (data not shown).

Mean (SD) tacrolimus (A) daily dose and (B) trough concentration (safety analysis population).
Overall, 49 patients (28.8%) discontinued tacrolimus treatment during follow-up, for the following reasons (there could be > 1 reason per patient): loss to follow-up due to changing hospitals (n = 20), patient death (n = 16), AEs (n = 12), cancellation of hospital visit during the observation period (n = 8), inadequate treatment response (n = 3), uncontrolled tacrolimus trough level (n = 1), and concerns of drug-drug interactions (n = 1). For the patients who discontinued tacrolimus, the median duration of therapy was 55 days (min 2 days, max 1023 days).
The mean (SD) dose of oral corticosteroids (prednisolone equivalent) at the start of tacrolimus treatment (baseline) was 32.4 (21.6) mg/day (n = 168) and decreased to 13.6 (5.8) mg/day (n = 133) at 6 months and 7.6 (4.2) mg/day (n = 90) at 2 years (Supplementary Table 1, available with the online version of this article). At baseline, approximately half of the patients were receiving a total daily corticosteroid dose > 30 mg/day (94/168 patients [56.0%]). Oral corticosteroids were similarly reduced over time in patients with PM, DM, and CADM (Supplementary Table 1), and in patients with or without anti-MDA5 and anti-ARS antibody (data not shown).
Safety. A total of 301 ADRs were reported in 121 patients (71.2%). In the 29 patients who were confirmed to have anti-MDA5 antibodies, 45 ADRs were reported in 19 patients (65.5%), whereas in the 74 patients who were anti-ARS antibody positive, 140 ADRs were reported in 57 patients (77.0%).
ADRs of special interest in the total safety analysis population are summarized in Table 2. Infections were reported in 48 patients (28.2%), renal impairment in 29 patients (17.1%), impaired glucose tolerance in 29 patients (17.1%), psychiatric and nervous system disorders in 26 patients (15.3%), cardiac dysfunction in 5 patients (2.9%), and pancreatic dysfunction in 1 patient (0.6%). The most prevalent serious ADRs of special interest were infections, which were reported in 23 patients (13.5%). Thrombotic microangiopathy (thrombotic thrombocytopenia purpura) was reported in 1 case. No cases of lymphoma were reported.
Incidence of ADRs and serious ADRs of special interest reported by MedDRA preferred terms occurring in > 1 patient over the 2-year follow-up (safety analysis population; n = 170).
Sixteen patients died during the 2-year follow-up (12 CADM, 3 classic DM, and 1 PM). The most common cause of death was ILD (12 patients, all with CADM), followed by lung cancer (2 patients, both with classic DM). All other causes of death were reported in only a single patient: suicide (CADM), worsening of congestive heart failure (classic DM), and myocarditis (PM).
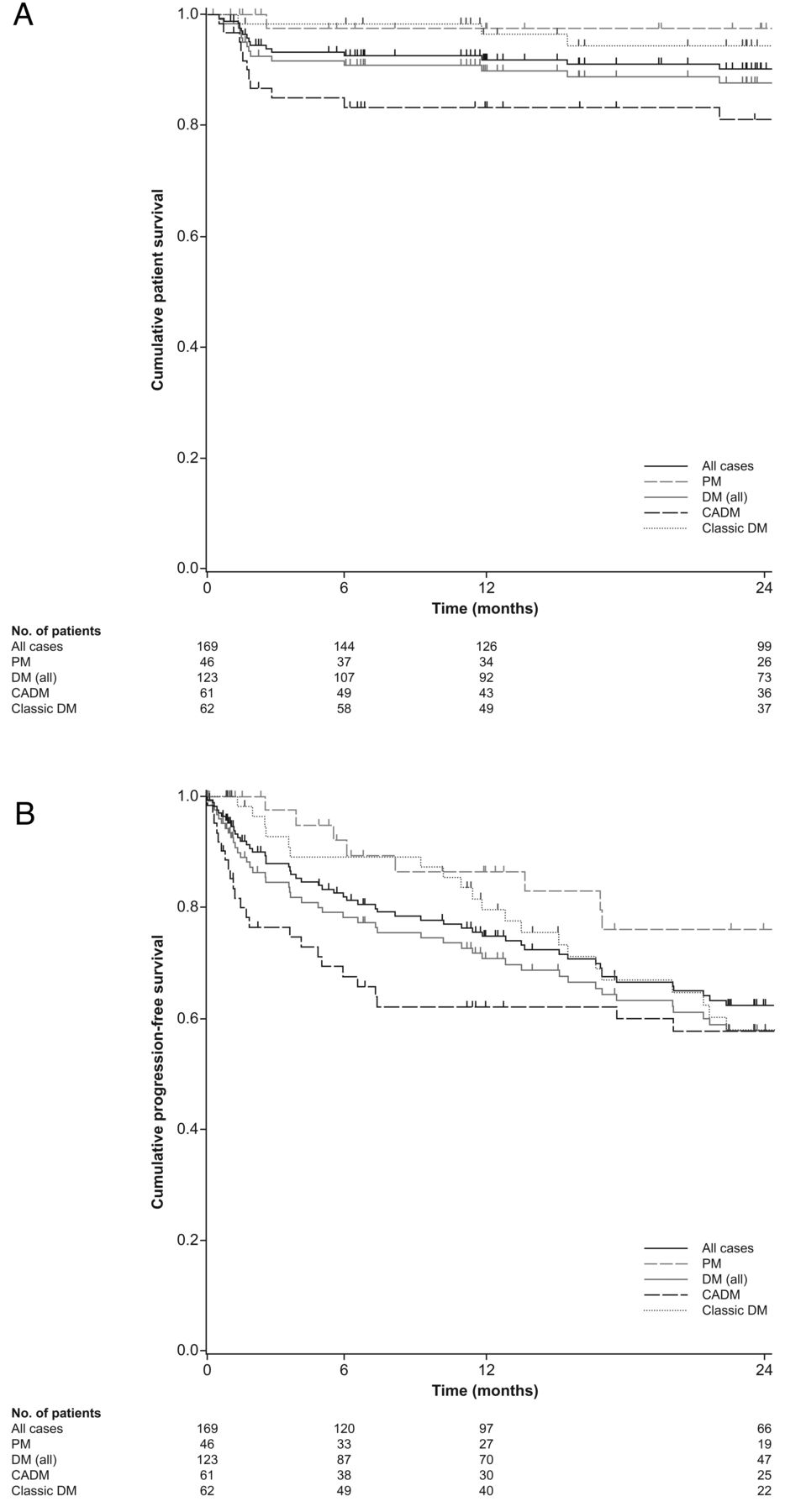
Clinical outcomes. Kaplan-Meier estimated cumulative overall and progression-free survival is shown in Figure 2. At 2 years, cumulative overall survival was 90.3% and cumulative progression-free survival was 62.5%. Overall and progression-free survival rates over the 2-year follow-up were highest in patients with PM (97.5% and 76.1%, respectively) and lowest in those with CADM (81.1% and 57.9%, respectively; Figures 2A,B). At 2 years, Kaplan-Meier estimated cumulative overall and progression-free survival were numerically lower in patients who were anti-MDA5 antibody positive vs negative (overall survival: 66.7% vs 100.0%, respectively; progression-free survival: 44.3% vs 62.0%; Figures 2C,D), and were numerically higher in patients who were anti-ARS positive vs negative (overall survival: 98.6% vs 77.4%; progression-free survival: 70.5% vs 55.7%; Figures 2E,F).



Kaplan-Meier curves of (A) overall patient survival, (B) overall progression-free sur-vival, (C) patient survival according to anti-MDA5 antibody status, (D) progression-free survival according to anti-MDA5 antibody status, (E) patient survival according to anti-ARS antibody status, and (F) progression-free survival according to anti-MDA5 antibody status, over the 2-year follow-up (clinical outcome analysis population). Anti-MDA5: antimelanoma differentiation-associated gene 5; anti-ARS: antiaminoacyl tRNA synthetase; CADM: clinically amyopathic dermatomyositis; DM: dermatomyositis; PM: polymyositis.
Changes in clinical outcome variables over the 2-year follow-up are shown in Table 3. Numerical increases in %FVC and PaO2 were observed from baseline to 2 years, while there was almost no change in %DLCO and AaDO2. Serum ferritin, KL-6 and SP-D levels decreased from baseline to 2 years; however, it should be noted that the number of patients with available data decreased over the 2-year follow-up. In patients with available data, improvement in chest CT findings from baseline was observed in 80/113 patients (70.8%) after 1 month of treatment and in 44/54 patients (81.5%) after 2 years.
Key clinical outcome parameters over the 2-year follow-up (clinical outcome analysis population).
Prognostic factors. Results of the analysis of potential prognostic factors for all-cause mortality are shown in Table 4. Factors found to have the highest association with mortality were diagnosis of CADM (HR 9.04, 95% CI 1.18–69.51 vs PM), ferritin level 500 to < 1500 ng/mL (HR 8.61, 95% CI 2.51–29.45 vs < 500 ng/mL), presence of anti-MDA5 antibody (HR 8.16, 95% CI 1.03–64.47 vs absence), arterial oxygen saturation (SaO2) level 90 to < 95% (HR 7.53, 95% CI 2.73–20.82 vs ≥ 95%), evidence of DAD (HR 4.58, 95% CI 1.03–20.38 vs NSIP), and oxygen administration (HR 3.82, 95% CI 1.23–11.88 vs without administration). Since there was general correlation between these prognostic factors, multivariable analysis was not undertaken to evaluate independence of individual factors.
Potential prognostic factors for all-cause mortality (clinical outcome analysis population).
DISCUSSION
This postmarketing surveillance was undertaken to assess long-term safety and clinical outcomes in patients with PM/DM-associated ILD treated with immunosuppressive regimens including tacrolimus. Data were available for a total of 170 patients; of these, most had initial onset of ILD (78.8%) and DM (72.9%). Approximately half of DM cases were CADM. Demographic and clinical characteristics at baseline were as expected for the patient population in Japan.24 Tacrolimus dose and trough levels were generally stable over the 2-year follow-up, with mean tacrolimus trough levels ranging from 6 to 8 ng/mL. In accordance with the prescribing information in Japan, tacrolimus was initiated at a dose of 0.0375 mg/kg twice daily, to be taken after the morning/evening meals, with a suggested target trough blood level of 5–10 ng/mL. In a recent clinical trial in patients with PM/DM-associated ILD initiating treatment with tacrolimus in combination with prednisolone, mean tacrolimus trough level over the 52-week study period was 6.6 ng/mL.13
A reduction in corticosteroid dose was seen in the patient population over the 2 years of follow-up regardless of PM or DM type, although the potential corticosteroid-sparing effect of tacrolimus could not be assessed due to the lack of an adequate control group. Other studies have also suggested that use of tacrolimus may permit a reduction in oral corticosteroid dosage in patients with PM/DM, potentially reducing the likelihood of AEs arising from prolonged corticosteroid exposure.10,11,25
Tacrolimus-containing immunosuppressive regimens were generally well tolerated, with a safety profile consistent with that seen in previous studies in this patient population.11,13 No unexpected safety concerns were identified over the 2 years of follow-up, although over 10% of patients initiated treatment with tacrolimus in combination with high-dose corticosteroids and CYC. As expected, the most common ADRs of special interest were infection (observed in 28.2% of patients), renal impairment (17.1%), impaired glucose tolerance (17.1%), and psychiatric and nervous system disorders (15.3%). These findings are in line with results of postmarketing surveillance of tacrolimus-containing immunosuppressive regimens for the treatment of other conditions, such as RA and lupus nephritis, in Japanese patients.26,27
Cumulative overall patient survival at 2 years was 90.3% and cumulative progression-free survival was 62.5%. In a recent openlabel clinical trial in 26 patients with PM/DM-associated ILD treated with tacrolimus and corticosteroids, 52-week patient and progression-free survival rates were 88.0% and 76.4%, respectively.13 The progression-free survival rates observed in our surveillance demonstrate that disease exacerbations may occur despite ongoing treatment in patients with PM/DM-associated ILD, highlighting the need for close clinical monitoring. Although overall survival was lowest in patients with CADM, the 2-year survival rate in this patient group was 81.1%.
Overall and progression-free survival over the 2-year follow-up were found to be lower in patients who were anti-MDA5 antibody positive than in those who were anti-MDA5 antibody negative. In contrast, 2-year overall and progression-free survival rates were higher in patients who were anti-ARS antibody positive compared with those who were anti-ARS antibody negative. Other studies in Japan and the US have also shown anti-MDA5 antibody–positive patients with interstitial pneumonitis to have more rapidly progressive disease and lower survival than anti-MDA5 antibody–negative patients.24,28 Similarly, presence of anti-ARS antibodies has also previously been shown to be associated with a higher overall survival rate.24,28
Improvements in chest CT findings and lung function variables (%FVC and PaO2), as well as serum ferritin, KL-6, and SP-D levels, were observed in patients with available data over the 2-year follow-up. Such improvements were also observed over 52 weeks in a recent open-label clinical trial of patients receiving tacrolimus.13 Collectively, these findings confirm the potential utility of immunosuppressive regimens including tacrolimus in patients with PM/DM-associated ILD.8-13,29
Identification of risk factors associated with poor prognosis in PM/DM patients with ILD is important for improving clinical outcomes.30 Potential factors found to have the highest association with all-cause mortality in this analysis were diagnosis of CADM, ferritin level 500 to < 1500 ng/mL, presence of anti-MDA5 antibodies, SaO2 90 to < 95%, and evidence of DAD. These findings are consistent with the results of other previous analyses of potential risk factors associated with poor outcomes in patients with myositis-associated ILD.24,31,32
An important strength of this surveillance is that it was conducted in real-world settings under routine clinical practice conditions. Potential limitations include the observational, open-label, noncomparative design and the collection of laboratory test data under routine practice conditions, resulting in some missing data. In particular, anti-MDA5 antibody status data were only available for a small proportion of patients, as the anti-MDA5 antibody test was only reimbursed through the Japanese medical insurance system from October 2016 (ie, during the last 3 months of the 3-year enrollment period). As such, it is possible that patients who were anti-ARS negative were positive to anti-MDA5, which might confound Kaplan-Meier estimates. The analysis of potential prognostic factors for mortality was limited by the low number of deaths observed over the 2-year follow-up (n = 16). This might result in insufficient precision and/or potentially biased estimates. In addition, it should be noted that this is an interim assessment of data from ongoing surveillance, with further analyses planned after 3 years of follow-up.
The principal aims of treatment in patients with PM/DM-associated ILD are improvement of current health status (ie, resolution of symptoms and increased physical activity) and reduction of future risk (ie, prevention of disease progression and improved overall prognosis).33 The results of this interim report suggest that tacrolimus-containing immunosuppressive regimens are well tolerated in patients with PM/DM-associated ILD, and may address both of these treatment goals. This surveillance is ongoing and longer-term follow-up is planned to further clarify the clinical utility of tacrolimus in this setting.
ACKNOWLEDGMENT
The authors wish to thank all investigators who participated in this postmarketing surveillance. Medical writing support was provided by Jennifer Coward for Lumanity, funded by Astellas Pharma Inc.
Footnotes
This work was supported by Astellas Pharma Inc. Editorial support was funded by Astellas Pharma Inc.
All authors report nonfinancial support from Astellas during the development of this manuscript. MK has received personal fees from MBL, Tanabe-Mitsubishi, Chugai, Ono Pharmaceuticals, Boehringer Ingelheim, Pfizer, Janssen, AbbVie, Eisai, Nippon Shinyaku, Mochida, and Asahi Kasei; and has received grants from Ono Pharmaceuticals and Boehringer Ingelheim. NW, TF, and SU are employees of Astellas Pharma Inc.
- Accepted for publication April 1, 2022.
- Copyright © 2022 by the Journal of Rheumatology
This is an Open Access article, which permits use, distribution, and reproduction, without modification, provided the original article is correctly cited and is not used for commercial purposes.
REFERENCES
DATA AVAILABILITY
Researchers may request access to anonymized participant level data, trial level data and protocols from Astellas sponsored clinical trials at www.clinicalstudydatarequest.com. For the Astellas criteria on data sharing see: https://clinicalstudydatarequest.com/Study-Sponsors/Study-Sponsors-Astellas.aspx
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.








{kind=link}
{kind=link}
{kind=link}
{kind=link}