

Abstract
Objective To investigate coronavirus disease 2019 (COVID-19) hospitalization risk in patients with immune-mediated inflammatory diseases (IMIDs) compared with matched non-IMID comparators from the general population.
Methods We conducted a population-based, matched cohort study using health administrative data from January to July 2020 in Ontario, Canada. Cohorts for each of the following IMIDs were assembled: rheumatoid arthritis (RA), psoriasis, psoriatic arthritis (PsA), ankylosing spondylitis, systemic autoimmune rheumatic diseases (SARDs), multiple sclerosis (MS), iritis, inflammatory bowel disease, polymyalgia rheumatica, and vasculitis. Each patient was matched with 5 non-IMID comparators based on sociodemographic factors. We compared the cumulative incidence of hospitalizations for COVID-19 and their outcomes between IMID and non-IMID patients.
Results A total of 493,499 patients with IMID (417 hospitalizations) and 2,466,946 non-IMID comparators (1519 hospitalizations) were assessed. The odds of being hospitalized for COVID-19 were significantly higher in patients with IMIDs compared with their matched non-IMID comparators (matched unadjusted odds ratio [OR] 1.37, adjusted OR 1.23). Significantly higher risk of hospitalizations was found in patients with iritis (OR 1.46), MS (OR 1.83), PsA (OR 2.20), RA (OR 1.42), SARDs (OR 1.47), and vasculitis (OR 2.07). COVID-19 hospitalizations were associated with older age, male sex, long-term care residence, multimorbidity, and lower income. The odds of complicated hospitalizations were 21% higher among all IMID vs matched non-IMID patients, but this association was attenuated after adjusting for demographic factors and comorbidities.
Conclusion Patients with IMIDs were at higher risk of being hospitalized with COVID-19. This risk was explained in part by their comorbidities.
Immune-mediated inflammatory diseases (IMIDs) are complex disorders caused by a combination of genetic susceptibility and environmental factors.1 Population-based studies have shown that > 5% of the general population have a diagnosis of ≥ 1 IMID.2,3 Patients with IMIDs are more susceptible to severe bacterial and viral infections.4,5,6 The coronavirus disease 2019 (COVID-19) raises special concerns regarding its course and outcome among patients with IMIDs. It is unclear if COVID-19–related hyperinflammatory response, commonly leading to organ failure,7 is more common among patients with IMIDs who already have dysfunctional host immune systems. Multimorbidity—in particular respiratory, cardiovascular (CV), and renal diseases—has been associated with poor COVID-19 outcomes and is prevalent among many patients with IMIDs.8,9,10,11 Finally, despite attempts to use immune-modulating agents to treat severe COVID-19, some of the medications commonly used to manage IMIDs, including corticosteroids and conventional and biologic immune-modulating agents, have been associated with a higher risk for infections.12,13,14
Despite multiple studies on COVID-19 risk in patients with IMIDs, population-based data remain scarce. A metaanalysis that included > 60 publications evaluating COVID-19 hospitalizations in patients with IMIDs found considerable heterogeneity in the estimated risk.15 The majority of included studies were limited by their small size, selected population (single site, academic centers), incomplete outcome surveillance (self-report, survey), and a lack of matched non-IMID comparators. To date, only a few population-based studies, mostly from European countries, found an increased risk of COVID-19 hospitalizations and mortality in patients with inflammatory joint diseases.16,17,18,19 However, information about the risk of severe COVID-19 among patients with IMIDs, especially in North America, remains limited. To accurately estimate COVID-19 risk in IMIDs, the use of unselected population-based data with complete reporting of hospitalizations and careful adjustment of potential confounding factors is needed.
To address this gap in knowledge, we used population-based, health administrative data from Ontario, Canada, to investigate the risk of hospitalizations for and severe complications of COVID-19 in patients with IMIDs compared with matched non-IMID individuals from the general population.
METHODS
Population and setting. We conducted a population-based, matched cohort study using health administrative data among adult residents in Ontario from January 1 to July 31, 2020. Ontario comprises almost 40% of the Canadian population, with 14.7 million individuals in 2020. The study population included adults aged ≥ 20 years who lived in the province on January 1, 2020. The first patient with COVID-19 in Ontario was reported on January 23, 2020. The Ontario Health Insurance Plan (OHIP) is a public, single-payer system that covers hospital admissions, physician services, and procedures including SARS-CoV-2 tests for all Ontario residents.20 Healthcare encounters are recorded in administrative databases, which are linked using an encoded health insurance number that is unique to each Ontarian. These data are held securely and analyzed in linked, coded form at ICES (www.ices.on.ca). The use of data in this project was authorized under section 45 of Ontario’s Personal Health Information Protection Act, and approved by ICES’ Privacy and Legal Office, and does not require review by a research ethics board.
Data sources. We used the OHIP physician service claims database to identify diagnosis codes of IMIDs and information about preexisting comorbidities. These diagnoses are coded using a modification of the International Classification of Diseases, 8th revision (ICD-8).21 The Canadian Institute for Health Information’s Discharge Abstract Database was used to identify diagnosis codes (ICD-10) of IMIDs and information about preexisting comorbidities occurring during hospitalizations, and to identify study outcomes. Information on residential income quintile was identified using Statistics Canada (www12.statcan.gc.ca) census data. Long-term care (LTC) residence was ascertained using the Complex Continuing Care LTC database (www.cihi.ca/en/continuing-care), which records the mandatory assessments on all LTC residents.
IMID case definitions. We used physician service claims and provincial hospitalization databases to assemble 10 nonmutually exclusive cohorts of patients with the following IMIDs: rheumatoid arthritis (RA), psoriasis (PsO), psoriatic arthritis (PsA), ankylosing spondylitis (AS), systemic autoimmune rheumatic diseases (SARDs; including systemic lupus erythematosus, systemic sclerosis, Sjögren syndrome, inflammatory myositis, mixed connective tissue disease), multiple sclerosis (MS), iritis, inflammatory bowel disease (IBD), polymyalgia rheumatica (PMR), and vasculitis (including giant cell arteritis and other types of vasculitides). When available, we used validated case definitions for the different IMIDs.22,23,24,25,26 For the remaining IMIDs that lacked prior case validation in Ontario, we used a similar approach that relied on a combination of physician visits for the specific IMID including ≥ 1 by a relevant specialist or ≥ 1 relevant ICD code given during a hospital admission. Of note, each patient may have been included in > 1 cohort. Detailed information about the case definitions for inclusion in each cohort is shown in Supplementary Material 1 (available with the online version of this article).
Study entry requirements included ≥ 1 of the above detailed IMIDs, being alive, age ≥ 20 years, and residing in Ontario on January 1, 2020. To ensure accurate baseline information, patients were also required to be eligible for OHIP coverage for at least 3 years prior to the study start date.
General population comparators. Each patient with IMID was matched with 5 patients without an IMID diagnosis based on age (± 5 yrs), sex, area of residence (by Local Health Integration Network), or residence in an LTC facility. All patients without IMIDs were required to be free of other IMIDs defined above.
Factors associated with hospitalizations. We assessed comorbidities reported to be associated with severe COVID-19 in the general population to determine if they were associated with COVID-19 hospitalizations in IMIDs.27 Information about individual comorbid conditions at study entry was obtained from physician service claims and provincial hospitalization databases (Supplementary Material 2, available with the online version of this article). The following comorbidities were assessed: CV diseases, chronic obstructive lung disease (COPD)/asthma, chronic kidney disease, hypertension, diabetes mellitus, pulmonary embolism or deep venous thrombosis, and dementia. Hospitalization due to respiratory tract infection (RTI) in the year prior to study entry, and the number of Johns Hopkins Aggregated Diagnosis Groups (ADGs) using the Johns Hopkins ACG System Version 10 were also evaluated. Sociodemographic predictors included socioeconomic status (defined by census neighborhood income quintiles), rurality (classified as living in urban vs rural settings), and residing in an LTC facility.
Since measures of IMID severity and activity are not available in administrative databases, we used the number of physician claims for IMID diagnoses in the year prior to cohort entry and IMID duration (defined as from first IMID encounter to cohort entry) as surrogates of disease activity and disease burden.
COVID-19 hospitalizations. Patients who were admitted at least once for COVID-19 during the study period were those who had one of the following COVID-19–related ICD-10 codes in their discharge summary: U07.1 (disease diagnosis of COVID-19 confirmed by laboratory testing) or U07.2 (clinical or epidemiological diagnosis of COVID-19 where laboratory confirmation is inconclusive or not available). These ICD-10 codes were introduced on February 24, 2020. The hospitalization outcomes were examined up to July 31, 2020. Only the first hospitalization for COVID-19 was considered for the analysis. As a secondary outcome, we assessed adverse COVID-19 hospitalization outcomes including admission to an intensive care unit (ICU), ventilation, or death during the admission. These were collectively termed complicated COVID-19 hospitalizations.
Since it was unclear whether all admissions due to COVID-19 were coded by the specific ICD-10 codes, we considered an alternative definition of COVID-19 hospitalization that included a combination of ICD codes associated with COVID-19 (eg, pneumonia, acute respiratory distress syndrome) in patients who tested positive for SARS-CoV-2 (Supplementary Material 3, available with the online version of this article). This definition was included in a sensitivity analysis only.
Statistical analysis. Descriptive statistics were computed to characterize patients among those with and without IMIDs (at the time of study entry). We calculated standardized differences between the 2 groups, with a standardized difference > 0.10 indicating a clinically meaningful difference.28 Age- and sex-standardized incidence rates of COVID-19 hospitalizations (along with 95% CIs) were reported for each IMID group and then overall using the 2016 Ontario population for direct age and sex standardization to enable comparisons across IMID groups. Patients were followed from study entry (January 2020) until they experienced any of the following outcomes (whichever came first): end of study (July 31, 2020), death, or first COVID-19 hospitalization.
We used multivariable logistic regression to model the probability of hospitalization for COVID-19 and for having complicated COVID-19 hospitalization between patients with IMIDs vs patients without IMIDs, adjusting for sociodemographic factors and comorbidities, and accounting for matching. Each regression model included membership in an IMID group as the primary covariate and the following additional covariates: age, sex, residing in LTC, number of comorbidities (by ADGs), socioeconomic status, and rurality. Then, among patients with IMIDs, we estimated adjusted odds ratios (ORs) along with 95% CI to compare COVID-19 hospitalizations among the different IMIDs, adjusting for the same covariates as above in addition to surrogates of disease activity, disease duration, and comorbidities.
RESULTS
A total of 493,499 adults with IMIDs and 2,466,946 matched non-IMID comparators who lived in Ontario in January 2020 were included in the study. Overall, the mean age of IMID patients was 58.3 (SD 17) years and 60.7% were female (Table 1).
Characteristics of the study population at baseline.
COVID-19 hospitalizations in patients with IMIDs. A total of 417 patients with IMIDs (0.08%) and 1519 matched patients without IMIDs were hospitalized for COVID-19 during the study period (0.06%). Of the hospitalizations, RA (32.1%) and PsO (27.6%) were the most common IMID diagnoses. Our sensitivity analysis using an alternative definition for COVID-19 hospitalizations identified a similar number of admissions (417 in IMIDs and 1530 in non-IMIDs); therefore, the primary definition of COVID-19 hospitalization was used for all analyses.
The overall age- and sex-standardized incidence of COVID-19 hospitalizations was higher in patients with IMIDs than in patients without IMIDs (6.44, 95% CI 5.78–7.16 vs 4.77, 95% CI 4.51–5.04 patients per 10,000 population, respectively). The highest absolute rates of hospitalizations were found in patients with vasculitis (17.99 per 10,000 population), MS (16.68 per 10,000 population), and PMR (10.06 per 10,000 population; Figure 1).

Age- and sex-standardized cumulative incidence of COVID-19 hospitalizations by IMID groups. AS: ankylosing spondylitis; COVID-19: coronavirus disease 2019; IBD: inflammatory bowel disease; IMID: immune-mediated inflammatory disease; MS: multiple sclerosis; PMR: polymyalgia rheumatica; PsA: psoriatic arthritis; RA: rheumatoid arthritis; SARD: systemic autoimmune rheumatic disease.
In our unadjusted analysis, patients with IMIDs were more likely to be hospitalized for COVID-19 than matched non-IMID patients (matched unadjusted OR 1.37, 95% CI 1.23–1.53; Figure 2). This association was somewhat attenuated after adjusting for demographic factors and comorbidities (matched adjusted OR 1.23, 95% CI 1.10–1.37). Numerically, higher odds of hospitalizations were found across all IMIDs (Figure 2). In the unadjusted model, patients with iritis, MS, PsA, RA, SARDs, and vasculitis had higher probability of being hospitalized vs with their matched non-IMID comparators. Hospitalization risk remained significantly higher in patients with RA, PsA, and MS after adjusting for demographic factors and comorbidities in the multivariable analysis.
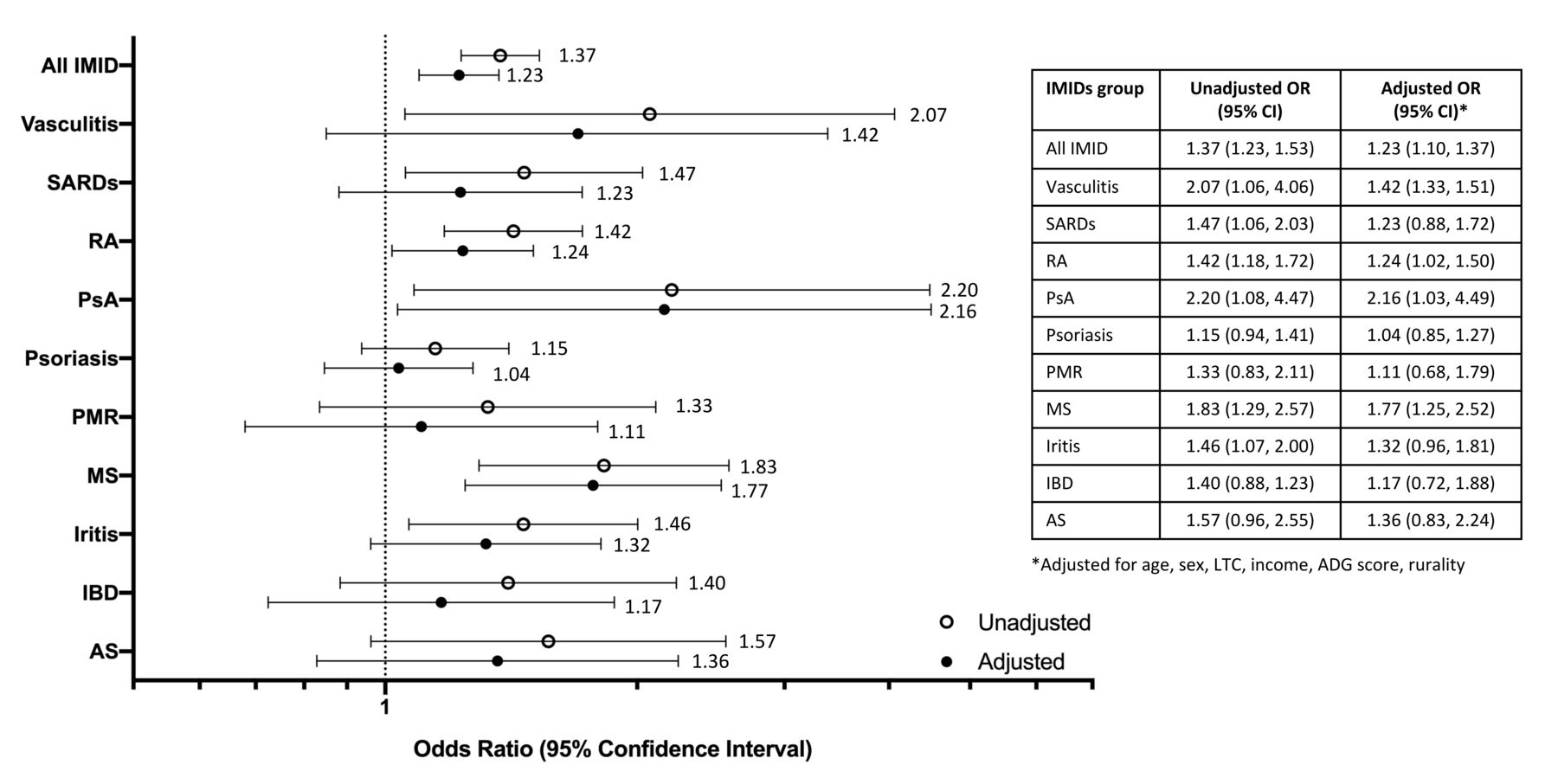
The association between IMIDs and COVID-19 hospitalizations by logistic regression showing the odds ratios and 95% CIs for the different IMID groups. ADG: Aggregated Diagnosis Group; AS: ankylosing spondylitis; COVID-19: coronavirus disease 2019; IBD: inflammatory bowel disease; IMID: immune-mediated inflammatory disease; LTC: long-term care; MS: multiple sclerosis; PMR: polymyalgia rheumatica; PsA: psoriatic arthritis; RA: rheumatoid arthritis; SARD: systemic autoimmune rheumatic disease.
Risk factors for COVID-19 hospitalizations. Risk factors for COVID-19 hospitalizations among patients with IMIDs (Table 2) included older age, male sex, residing in LTC facility, and lower socioeconomic status. In addition, the following comorbidities in patients with IMIDs were significantly associated with COVID-19 hospitalizations: dementia, chronic kidney disease, hospitalization due to RTI in the year prior to study entry, CV disease, diabetes, hypertension, and COPD/asthma. Regarding IMID-related factors, a weak but significant association was found between shorter IMID duration and hospitalization risk.
Factors associated with COVID-19 hospitalizations among patients with IMIDs by multivariable logistic regressiona.
Complicated COVID-19 hospitalizations. A total of 163 out of the 417 (39.1%) patients with IMIDs who were hospitalized for COVID-19 experienced complications during their admission. The proportion of those without IMIDs who experienced a complicated hospitalization was numerically higher however not different statistically (676 out of 1519 hospitalizations [44.5%], P = 0.05). The proportions of in-hospital deaths among those hospitalized with COVID-19 were similar in patients with and without IMIDs (IMIDs: 101 out of 417 [24.2%] vs non-IMIDs: 388 out of 1519 [25.5%], P = 0.3).
Considering the entire study population, patients with IMIDs were at higher risk for complicated COVID-19 hospitalizations (matched unadjusted OR 1.21, 95% CI 1.02–1.43) compared with their matched non-IMID comparators in our univariate analysis, which attenuated after adjustment (matched adjusted OR 1.09, 95% CI 0.91–1.29; Figure 3). In the unadjusted regression analysis, significant risk for complicated COVID-19 hospitalizations was found in patients with MS (OR 2.09) and RA (OR 1.39) compared with matched non-IMID comparators. The risk for complicated COVID-19 hospitalizations remained elevated in the fully adjusted model in patients with MS (OR 2.03). In the remaining IMID subgroup, the CIs were wide and crossed 1.

The association between IMIDs and complicated COVID-19 hospitalizations by logistic regression showing the odds ratios and 95% CIs for the different IMID groups. ADG: Aggregated Diagnosis Group; AS: ankylosing spondylitis; COVID-19: coronavirus disease 2019; IBD: inflammatory bowel disease; IMID: immune-mediated inflammatory disease; LTC: long-term care; MS: multiple sclerosis; PMR: polymyalgia rheumatica; PsA: psoriatic arthritis; RA: rheumatoid arthritis; SARD: systemic autoimmune rheumatic disease.
DISCUSSION
In one of the largest population-based studies to date, we found that patients with IMIDs were at higher risk of being hospitalized for COVID-19. This association was only partially explained by comorbid conditions, highlighting the independent risk for experiencing severe COVID-19 associated with a diagnosis of IMID.
COVID-19 continues to pose major challenges to the healthcare system, leading to high rates of hospitalizations as well as in-hospital complications and death. Patients with IMIDs, with their unique characteristics, deserve special attention that focuses on their overall risk of experiencing a severe course of COVID-19. Population-based information regarding the risk of severe COVID-19 remains limited. A metaanalysis that summarized 6 small case-control studies concluded that the risk of COVID-19 hospitalizations was similar in patients with and without IMIDs.15 In contrast, recent population-based studies from Denmark and Sweden found that the risk of COVID-19 hospitalizations was increased by 46% and 32%, respectively, in patients with inflammatory rheumatic diseases compared with the general population, with the highest risk found in patients with RA.16,17 Another study from the US that included patients who were diagnosed with COVID-19 showed that a diagnosis of IMID was associated with a 14% higher risk of being hospitalized and a 32% higher risk for ICU admission than patients without IMIDs.18 We found a 37% higher risk of hospitalizations in patients with IMIDs (23% higher after adjusting for comorbidities and sociodemographic factors); this finding is in line with previous reports from Europe. Our study results further expand on the differential risk of hospitalization across IMID subgroups. While hospitalization risk was numerically higher across all IMIDs, several disease groups were associated with significantly higher risk of being hospitalized compared with their matched non-IMID comparators. This higher risk in IMID groups, such as RA, SARDs, MS, vasculitis, PsA, and iritis, may be due to treatment with systemic corticosteroids and/or high burden of complex comorbidities. Despite their proven benefit in improving outcomes of severe COVID-19 in the general population, systemic corticosteroids have been associated with a higher risk of severe COVID-19 in patients with IMIDs.29,30,31,32 Multimorbidity was a major contributing factor to the risk of hospitalization in our study, with a number of chronic comorbid conditions, including CV, respiratory, and kidney diseases, as well as hypertension, diabetes, and dementia, contributing to this risk. These comorbid conditions tend to be associated with IMIDs directly due to the disease process or shared risk factors, or secondary to treatment used to manage IMIDs. Previous studies in the general population and among patients with IMID identified some of these comorbidities as risk factors for severe COVID-19 disease.27,29,31,33 Thus, our results suggest that an overall higher but differential COVID-19 hospitalization risk among patients with IMIDs is only partially explained by their higher comorbidity burden.
It remains controversial whether patients with IMIDs are at higher risk of experiencing in-hospital complications compared to non-IMID patients. While it has been suggested that patients with IMIDs are at higher risk for experiencing complicated hospitalizations,34 other studies have not yet found such an association.35,36 We found 21% higher odds of complicated hospitalizations among patients with IMIDs when considering the entire study population, regardless of whether they were admitted. However, among those admitted for COVID-19, the overall proportion of complicated hospitalizations was similar in patients with and without IMIDs, as were the proportions of those who required ICU admission and those dying during admission. The similar hospitalization outcomes in IMID and non-IMID patients are notable given the higher number of comorbidities in the former group. The high proportion of complicated admissions among patients with IMIDs who were admitted, reaching 39% of all admitted patients, is noteworthy. These figures are in accordance with previous studies that reported 32–48% of patients with IMID experiencing in-hospital complications and 13–22% dying during admission,17,33,34,37 reflecting the first wave of the pandemic. It remains to be seen whether the rates of these adverse outcomes have changed in subsequent waves of the disease following changes in the approach to treatment of hospitalized patients with COVID-19.
A major strength of our study is the centralized data resource in the setting of a public health system with access to hospital care for the entire population. To our knowledge, this is one of the largest studies published to date on COVID-19 hospitalizations in patients with IMIDs. We were able to avoid some of the major limitations of previous studies due to the large cohort of patients with IMIDs and matched non-IMIDs as well as the complete reporting of hospitalizations; thus, our results are both robust and highly generalizable. We acknowledge several limitations. First, the case definitions are based on diagnosis coding from physicians and hospital records used for administrative purposes, so misclassification of IMID diagnoses is possible. When available, we used validated case definitions that showed high performance in previous studies, and we used a similar approach to identify IMIDs without validated case definitions. The population prevalence and demographic characteristics of the different IMIDs in our study is in line with what would be expected, providing further face validity to the accuracy of our case definitions. Second, since outpatient prescription medications in Ontario are funded only for patients aged ≥ 65 years, social assistance recipients, and residents who have very high drug costs relative to their income, we did not include medication data in our study. Therefore, we could not evaluate the effect of these immunosuppressives or other medications on hospitalizations. Some studies suggest that the risk of severe COVID-19 is associated with the use of some immune-modulating agents, such as corticosteroids (higher risk) and tumor necrosis factor inhibitors (lower risk)29,30,31; however, other studies could not find such associations.17,33 Last, due to delays in reporting, we do not have information about patients who died outside of hospital, either before they could be admitted or after they were discharged.
In summary, we found that the risk of severe COVID-19 requiring hospitalization is increased in patients with IMIDs compared with non-IMID patients. This risk is partially explained by the higher burden of comorbidities in patients with IMIDs and varies across different IMIDs. Older age, number and severity of comorbidities, and sociodemographic factors contribute to hospitalization risk among patients with IMIDs, as they do in the general population. Our results suggest that patients with IMIDs should be considered a high-risk group for developing severe COVID-19. These data support advocacy and public health measures to reduce the risk of infection, such as promoting COVID-19 vaccinations among patients with IMIDs.38,39
Footnotes
The study was supported by ICES (formerly known as the Institute for Clinical Evaluative Sciences), which is funded by the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). Parts of this material are based on data and information compiled and provided by MOH and the Canadian Institute for Health Information. The opinions, results, and conclusions reported in this paper are those of the authors and are independent of the funding or data sources; no endorsement is intended or should be inferred. JW receives support from the Arthritis Society Stars Career Development Award (STAR-19-0610). SB is a James McGill Professor of Medicine. SRJ is supported by a New Investigator Award from the Canadian Institutes of Health Research and the Gurmej Kaur Dhanda Scleroderma Research Award.
LE received research/educational grants from AbbVie, UCB, Pfizer, Eli Lilly; and consulting fees from AbbVie, Pfizer, Novartis, UCB. BK is a rheumatology advisory board member for Pfizer, Gilead, and AbbVie. SRJ received grants/contracts from Boehringer Ingelheim and Corbus; consulting fees from Boehringer Ingelheim, Corbus; is a member of the American College of Rheumatology (ACR) COVID-19 Clinical Guidance Task Force and ACR COVID-19 Vaccination Guidance Task Force. The remaining authors declare no conflicts relevant to this article.
- Accepted for publication January 14, 2022.
- Copyright © 2022 The Journal of Rheumatology. This is an Open Access article, which permits use, distribution, and reproduction, without modification, provided the original article is correctly cited and is not used for commercial purposes.








{kind=link}
{kind=link}
{kind=link}