

Abstract
Objective This systematic literature review determined whether there is clinical utility for dual-energy computed tomography (DECT) to inform on prognosis for patients with gout. With DECT, individualized treatment plans could be developed based on the patient’s unique urate burden, with DECT being used as a clinical outcome measure in gout management.
Methods To evaluate DECT as a reliable, valid, and sensitive prognostic instrument, a librarian-assisted search was undertaken in PubMed and Embase for articles on gout and DECT informing on reliability; content, construct, and criterion validity; sensitivity to change; and minimum clinically important changes.
Results This systematic literature review showed that DECT has high intra- and interrater reliability. Tophus burden correlates with functional loss to show content validity. DECT volume is positively correlated with death, cardiovascular risk factors, and the risk for future gout flares. DECT has excellent sensitivity to change with effective urate-lowering therapies.
Conclusion DECT is a promising prognostic tool based on its high reliability, sensitivity to change, and emerging validity. Additional large, well-designed, prospective cohort studies are needed to fully evaluate its prognostic utility. This systematic review suggests that DECT very likely has additional prognostic information beyond clinical tophi assessment alone.
Gout has a rising global prevalence, with the highest rates among the Pacific Island populations and a higher burden in the developed world; its regional prevalence varies from 0.1% up to 10.0%.1 The United States has an estimated 9 million individuals with gout.2 The current gold standard for a gout diagnosis is detection of monosodium urate (MSU) crystals in joint fluid.3 Joint aspiration can be a painful, invasive process,4 which not all healthcare providers are able to perform. Dual-energy computed tomography (DECT) scans are a noninvasive technique that may be an alternative diagnostic tool, especially in patients with more established gout,5 as DECT scans have excellent reliability.6
The gout disease process is a continuum, starting with asymptomatic hyperuricemia, progressing to acute gouty attacks, and then to persistent arthritis, joint destruction, and subcutaneous tophi as urate deposits build.6 Crystals can deposit in multiple locations, including joints, tendons, cartilage, and skin.7 Higher urate burdens are associated with diabetes, hypertension, cardiovascular (CV) disease, and chronic kidney disease.8-10
DECT scans provide an individualized volumetric urate burden and are a longitudinal outcome measure. DECT should be recommended as a standard clinical assessment if it can be proven to provide additional prognostic information beyond tophi counts alone. Tophi and DECT volumes are known independent predictors of mortality,11 and DECT reliability is better than clinical tophi assessment.12
To have prognostic value, DECT should be reliable and valid, including content validity (ie, the results should represent the truth), construct validity (ie, the results should move in predictable ways with other clinical measures of similar concept, like erosions), and criterion validity (ie, the results should predict disease features, like death, disability, and distress). DECT should provide more prognostic information than clinical tophi alone to warrant routine clinical use. DECT should also be sensitive to change with effective urate-lowering therapy (ULT), with these changes correlating to other important health measures.13 The goal of this systematic review is to inform on the reliability and validity of DECT to understand its prognostic value in patients with gout.
METHODS
A systematic search was undertaken in PubMed and Embase databases from inception to February 29, 2022. Medical Subject Headings (MeSH) used for the search were as follows: (“dual energy computed tomography” OR “DECT”) AND (“gout”) AND (“urate burden” OR “monosodium urate volume” OR “monosodium urate crystals”). The following keywords were used with the MeSH terms: (“dual energy computed tomography” OR “DECT”), (“gout, tophaceous gout, chronic gout”), and (“monosodium urate crystals” OR “monosodium urate burden” OR “tophi” OR “monosodium urate volume” OR “flares” OR “pain” OR “distress” OR “death” OR “disability” OR “function”). Titles and abstracts identified were screened by both authors. A manual search of secondary sources included personal holdings, conference abstracts, and review of the references of identified articles.
Inclusion criteria were original research on DECT and its reliability, validity, relationship to clinical outcomes, and ability to detect change. Participants must have had gout diagnosed by the American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/EULAR) classification and/or crystal confirmation. Excluded papers included the following: editorials, narrative reviews, case reports, letters to the editor, and conference abstracts without complete methods and results. Nonhuman and non-English studies were excluded. Data selection and extraction were performed independently by both authors, and final data presentation was based on consensus.
To assess study quality, 2 approaches were implemented. For systematic reviews of DECT reliability, the AMSTAR 2 (A Measurement Tool to Assess Systematic Reviews–revised) was used,14 which was designed to critically appraise systematic reviews of randomized and nonrandomized studies based on 16 elements. An overall summary score is not provided, but each systematic review is rated based on weaknesses in critical domains. In the interest of space limitations, only the highest quality metaanalyses are represented in Table 1. For all other studies, we used the approach of the International League of Associations for Rheumatology 2000-2010 Decade of the Bone and Joint Neck Pain Task Force.15 Methodological quality was evaluated by considering selection bias, information bias, and confounding to inform on a study’s internal validity. No formal grading scale was used. No articles were excluded based on predefined cut points. Methodologic features of the included studies are summarized in Table 1 and Table 2.
Summary of the reliability and diagnostic performance characteristics of DECT imaging in patients with gout.
Death and predictors of mortality.
Disability.
Distress, as assessed by gout flares.
Reliability was interpreted based on generally accepted standards, such as intraclass correlation coefficient (ICC) estimates, where values of 0.00 to 0.39 represent poor agreement, 0.40 to 0.59 represent fair agreement, 0.60 to 0.74 represent good agreement, and 0.75 to 1.00 represent excellent agreement.16 Validity was assessed by construct and criterion validity. Construct validity is described by OMERACT (Outcome Measures in Rheumatology) as follows: “Do the results of the instrument agree with expected results of other instruments measuring the same construct/concept?”17 Criterion validity is described by OMERACT as follows: “Does the result of the instrument predict or correlate with long term outcomes (e.g. death, disability, perhaps X-ray damage)?”17
RESULTS
MEDLINE and Embase searches yielded 393 potential citations. Full manuscripts of interest were retrieved and reviewed for 98 abstracts (24.9%). A total of 49 out of 98 manuscripts (50%) were found to be relevant to our goals. A complete list of articles considered, along with the rationale for final selections, is available from the authors. Articles on gout and DECT first appeared in English in 2007, denoting a nascent literature.
DECT is highly reliable, with excellent ICCs varying from 0.86 to nearly 1.00 for both intrarater and interrater reliability, as summarized in Table 118-33 along with DECT performance characteristics (ie, sensitivity, specificity, and area under the curve [AUC]). Systematic reviews of the highest quality are presented in descending order based on year of publication, followed by selected primary studies describing intrarater reliability and then DECT studies in early gout showing the heterogeneity of DECT performance by gout duration.
Metaanalyses that scored the best on the AMSTAR 2 tool were authored by Gamala et al,19 Chen et al,21 Newberry et al,23 Ogdie et al,24 and Zhang et al.30 The review by Ogdie et al24 is among the oldest, and Newberry et al23 included only 3 studies. The Gamala et al19 and Chen et al21 metaanalyses differ in their inclusion of studies with and without a joint aspiration gold standard. Chen et al21 summarized 6 articles and showed a pooled sensitivity of 0.88 (95% CI 0.90-0.96), a pooled specificity of 0.85 (95% CI 0.67-0.78), and a pooled AUC of 0.93 (no 95% CI given), with joint aspiration used as the gold-standard assessment. Gamala et al19 did not require joint aspiration to confirm gout in their included articles, and they included 10 articles with a pooled sensitivity of 0.81 (95% CI 0.77-0.86) and a pooled specificity of 0.91 (95% CI 0.85-0.95). In total, 2 studies that used aspiration for gout diagnosis had a pooled sensitivity of 0.92 (95% CI 0.81-0.97) and a pooled specificity of 0.81 (95% CI 0.69-0.90). A total of 2 studies using the ACR 1977 clinical criteria had a pooled sensitivity of 0.89 (95% CI 0.85-0.92) and a pooled specificity of 0.88 (95% CI 0.80-0.93), suggesting similar diagnostic performance with aspiration or clinical criteria.19
Singh and colleagues34 studied a clinic-based cohort that confirms the comparable DECT test performance with either joint aspiration or a clinical diagnosis. In 147 patients with a mean gout duration of 9 years and a mean age of 65 years, DECT and ultrasound were contrasted against joint aspiration (ie, the gold standard) and ACR/EULAR 2015 clinical classification (ie, the silver standard).34 DECT of feet and ankles had a sensitivity of 0.87 (95% CI 0.82-0.92) and a specificity of 1.00 (95% CI 1.00-1.00) vs joint aspiration. Against ACR/EULAR clinical criteria, DECT had a sensitivity 0.82 (95% CI 0.79-0.85) and a specificity 0.76 (95% CI 0.72-0.80), similar to joint aspiration. Singh et al34 found that DECT of feet and ankles was only preferred to DECT of feet, ankles and knees combined, or knees alone, based on better AUCs. In fact, DECT of feet and ankles outperformed ultrasound against the gold standard of joint aspiration.
DECT in patients with early gout has lower sensitivity, as suggested by Gamala et al,19 Odgie et al,24 Zhang et al,30 and others. Zhang et al30 examined patients with early gout (ie, < 1 year from first symptoms) and contrasted DECT sensitivity to patients with middle gout and late gout. DECT scans showed a sensitivity of 4 out of 15 (0.27) in early gout, 8 out of 12 (0.67) in middle gout, and 9 out of 10 (0.90) in late gout against joint aspiration.30 Ultrasound sensitivity was higher in early-stage gout compared to DECT at 0.66 vs 0.27 (P < 0.050).30 For patients with early gout, Lee et al31 showed sensitivities from 0.51 and 0.53 for 2 readers, with a specificity of 1.00 for both. Early gout was determined by excluding patients with tophi, erosions, or use of ULT, with 103 patients with 115 painful joints included, while DECT was read by 2 experienced radiologists. Gout diagnosis was based on consensus of 2 rheumatologists using the ACR/EULAR 2015 criteria. Kravchenko et al33 suggested that early gout had more false negatives with DECT. Among 36 subjects, DECT confirmed that positive cases had a median disease duration of 43 (IQR 5-103) months, whereas false negatives had a median duration of 4 (IQR 2-33) months.33 Shang et al18 defined early gout as a disease duration of less than 1 year, middle gout as a duration from 1 to 3 years, and late gout as a duration of more than 3 years in a 196-subject cross-sectional study. The 49 early gout cases had a DECT sensitivity (feet and ankles) of 0.38 (95% CI 0.18-0.62), with a specificity of 0.96 (95% CI 0.82-0.99); late gout had a sensitivity of 0.78 (95% CI 0.68-0.85) and a specificity 0.88 (95% CI 0.84-0.99).32 DECT reliability was not influenced by gout duration, with interreader agreements of 0.87 and 0.86 in early gout and late gout, respectively.32 In a separate study, Shang et al18 performed a metaanalysis of 28 studies with DECT and ultrasound, including early gout, defined as disease duration of less than 2 years. The DECT pooled sensitivity in early gout was 0.75 (95% CI 0.60-0.86) and the pooled specificity was 0.85 (95% CI 0.75-0.91); ultrasound had a pooled sensitivity of 0.93 (95% CI 0.72-0.99) and a pooled specificity of 0.80 (95% CI 0.71-0.86) when positive findings included the double contour sign and ultrasound detected tophi.18 DECT was a better diagnostic test overall compared to ultrasound when all disease durations were combined; the DECT pooled sensitivity was 0.89 (95% CI 0.80-0.94) and the pooled specificity was 0.91 (95% CI 0.88-0.94), as compared to the ultrasound pooled sensitivity of 0.84 (95% CI 0.73-0.91) and the pooled specificity of 0.84 (95% CI 0.78-0.89).18 Collectively, early-stage gout appears to have reduced sensitivity (ie, more false negatives) with preserved specificity (ie, fewer false positives) compared to later gout.
Construct validity for DECT was demonstrated by its correlation with radiographic erosions in 4 studies.35-38 Dalbeth et al35 reported a cross-sectional study of 92 patients with tophaceous gout undergoing radiographs and DECT of feet. An experienced rheumatologist scored 920 metatarsophalangeal (MTP) joints. DECT volume was correlated to radiographic damage, with a correlation coefficient of 0.70 (P < 0.001).35 Shi et al36 studied 27 patients with gout in a retrospective cross-sectional study; the patients had a median age of 52 years and a median disease duration of 84 months. Total erosions were defined on computed tomography (CT) as a focal area of cortex loss with sharply defined margins in 2 planes and bone cortex breach in more than 1 plane. Total erosions, defined as above, positively correlated with DECT volume (rs = 0.55, P = 0.003) in 52 individual foot joints across all participants.36 Pecherstorfer et al37 studied 20 patients with gout with a mean age of 59 years and a mean gout duration of 12 years. The MTP1 joint, the phalangeal base, and 2 sesamoid bones were assessed by DECT and CT. Erosions were defined as pathological juxtaarticular cortical breaks in at least 2 successive slices and vertical planes on CT. DECT volume correlated with erosions (r = 0.60, P = 0.005).37 Yokose et al38 studied 153 patients with a mean age of 59 years and a mean disease duration of 15 years. DECT and CT scans of the hands and wrists, feet and ankles, and knees alone showed that subcutaneous tophi were more likely when bone erosions were present (83.0% vs 67.0%, P = 0.040), with erosions 8 times more likely with abnormal DECT scans of the ankles and feet vs normal DECT scans (43.6% vs 8.6%, odds ratio [OR] 8.10).38
Importantly, DECT has been shown to detect urate deposition in patients without clinical evidence of urate abnormalities. Dalbeth et al12 collected DECT scans from 152 patients with and without palpable tophi. Patients were treated with allopurinol doses of > 300 mg/day for 5 years, and DECT of the hands and wrists; feet, ankles, and Achilles; and knees alone were collected. DECT abnormalities were present in 47.0% of patients with normal serum uric acid (< 6.0 mg/dL) without palpable tophi, and this increased to 90.0% when serum uric acid was > 6.0 mg/dL and tophi were palpable.12 Therefore, DECT volume correlates with bone erosions, whereas DECT deposits exist in the absence of clinical urate abnormalities.
Evidence for criterion validity is summarized in the Figure and in Table 2A-C. Dalbeth et al39 found that tophaceous joint disease strongly predicts loss of hand function. The number of joints with overlying tophi was found to be the single best predictor of Sollerman hand function, with a correlation coefficient of 0.59 (P < 0.050).39 No studies have examined DECT volume against hand or foot function or overall disability, but since joint erosions are a direct consequence of tophus invasion, such a relationship would be expected.35
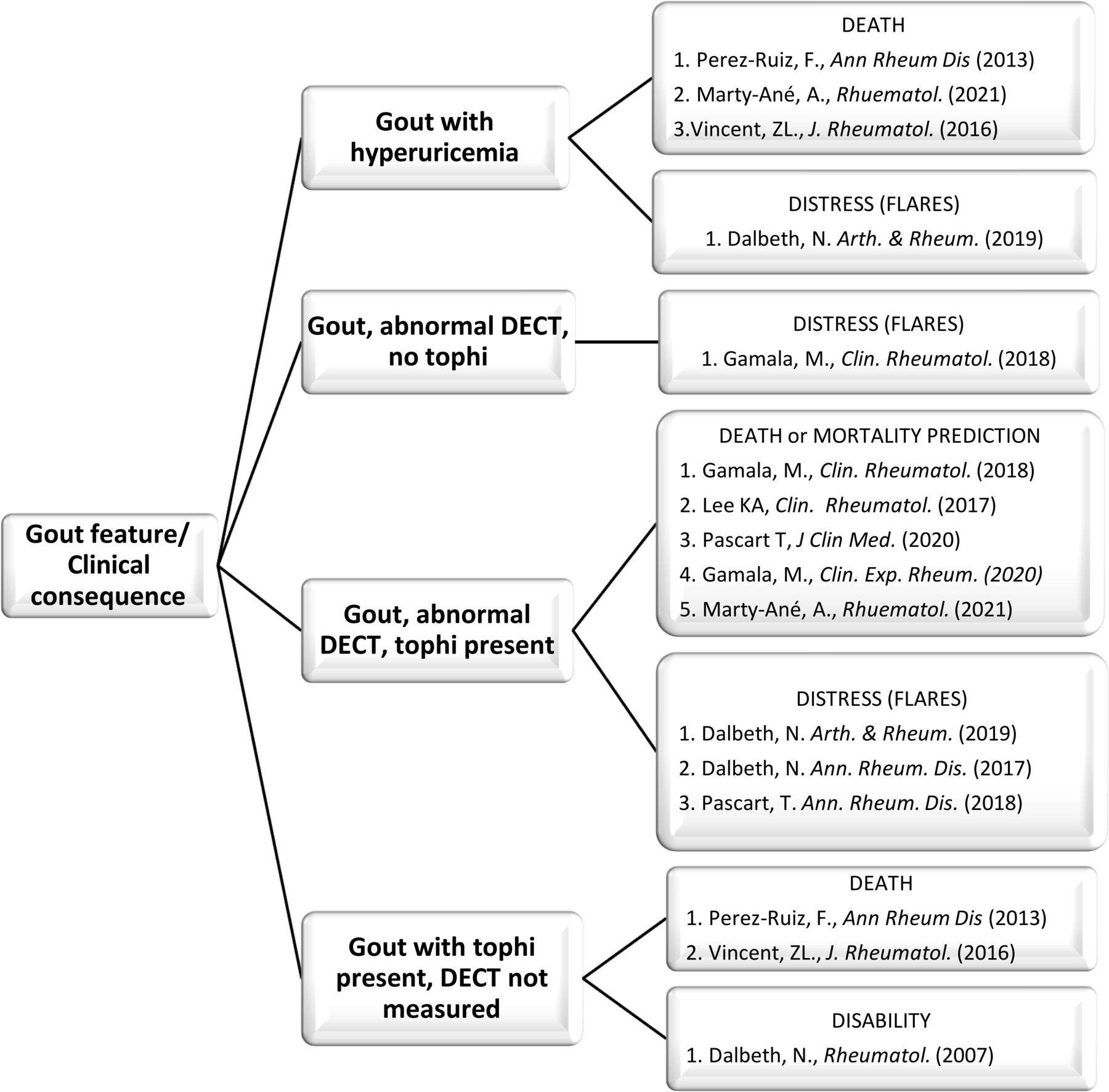
Criterion validity for DECT in patients with gout based on stage of gout, with and without tophi and with and without DECT for death and mortality prediction, disability, and distress (ie, gout flares). DECT: dual-energy computed tomography.
Perez-Ruiz et al40 studied a large clinical cohort and found that patients with gout with an increasing burden of clinical tophi had a proportional increased risk of death (hazard ratio [HR] 2.05, 95% CI 1.29-3.28). Vincent et al11 found that clinical tophi were the best predictors of all-cause and CV mortality in patients with gout. Greater urate deposition on DECT also correlates with mortality and predictors of CV mortality. Marty-Ané et al41 followed a cohort of 128 patients with gout for 3 years; the cohort had a mean age of 66 (SD 14) years and a mean gout duration of 11 (SD 10) years. Baseline DECT scans of feet, ankles, and knees showed that DECT volumes were the single best predictor of mortality (HR 1.02, 95% CI 1.01-1.03).41 Survivors had smaller DECT volumes, on average, as compared to nonsurvivors (0.20 vs 0.40 cm3, P = 0.045); in addition, DECT volume was associated with mortality, but baseline clinical tophi were not (P = 0.060).41 DECT volume and predictors of CV mortality were assessed in 6 studies, with 5 reporting a positive association.8,10,41-43 A retrospective cross-sectional study by Gamala et al8 reported that a positive DECT scan was associated with the presence of CV disease (OR 3.07, 95% CI 1.26-7.47).
A 2020 study by Gamala et al42 showed a positive, nonsignificant relationship using multivariate logistic regression between positive DECT volume and predicted CV events; ORs for mortality risk increased as DECT volume increased, from the first to the third quartile (OR 4.80, 95% CI 0.60-42.00; P = 0.100) and from the first to the fourth quartile (OR 6.40, 95% CI 0.70-63.00; P = 0.100). Lee at al43 performed a clinical case study and found a significant univariate association between DECT volume and the American Heart Association 10-year CV risk score (r = 0.22, P = 0.040). A multivariable analysis showed DECT scores to be one of the strongest predictors (total model fit R2 = 0.76, P < 0.001).43 Pascart et al44 initially found no significant association between DECT volumes of the knees, feet, or both and CV risk on the Framingham Risk Score, with P values of 0.180, 0.010, and 0.130, respectively.
In a second study, Pascart et al10 studied 91 patients with gout who were not previously on ULT with baseline DECT scans of the feet, ankles, and knees. DECT volumes of ≥ 1 cm3 were statistically associated with CV risk factors, including age, gout duration, clinical tophi, hypertension, diabetes, and chronic heart failure.10 The median DECT volumes were 1.01 (IQR 0.18-2.66) cm3 for patients with hypertension and 0.38 (IQR 0.10-0.62) cm3 for those without (P = 0.020). For diabetes, the median DECT volumes were 1.09 (IQR 0.29-2.63) cm3 for patients with diabetes vs 0.41 (IQR 0.09-2.11) cm3 for those without (P = 0.050). The median DECT volumes were 2.04 (IQR 0.70-2.95) cm3 for patients with chronic heart failure vs 0.42 (IQR 0.12-1.96) cm3 for those without (P = 0.030).10 The median DECT volumes were 1.01 (IQR 0.22-3.00) cm3 for those with a gout disease duration of > 2 years vs 0.25 (IQR 0.10-0.70) cm3 for those with a disease duration of ≤ 2 years (P = 0.007). In multivariable analysis, chronic heart failure was retained as a factor explaining DECT volume (adjusted R2 = 0.21, F = 5.60, P = 0.0002). Thus, DECT volume has been associated with CV mortality in a prospective cohort,41 with predictors of CV mortality in 5 out of 6 studies.
Criterion validity includes the concept of distress, with measures including pain and disability associated with gout flares. Gout flare rates were shown to be positively correlated to DECT volume in 4 studies.8,12,45,46 Dalbeth at al45 followed patients over 2 years and found that those with flares had mean DECT volumes of 2.60 (95% CI 2.30-3.00) cm3 vs 2.10 (95% CI 2.00-2.20) cm3 among those without flares (P < 0.001). Pascart et al46 found that DECT volume predicted future gout flares. Patients with ≥ 1 flare between 0 and 6 months had a mean DECT volume of 2.40 (SD 2.1) cm3 vs those without flares whose mean DECT volume was 0.90 (SD 1.30) cm3 (P = 0.006).46 Dalbeth et al12 demonstrated that 83.3% of patients with abnormal DECT scans had flares in the past month, as compared to 63.6% of patients with abnormal DECT scans who did not have flares (P = 0.019). Greater DECT volumes were associated with more palpable tophi, serum urate levels ≥ 6 mg/dL, > 1 gout flare, and allopurinol doses of > 300 mg/day.12 A retrospective analysis by Gamala et al8 showed that a positive DECT scan was associated with more gouty attacks per year (OR 1.23, 95% CI 1.07-1.42) compared to patients without abnormal DECT scans.
DECT is sensitive to changes in urate volumes. Araujo and colleagues47 measured the tophus volume on DECT before and after pegloticase intravenous treatments. A clinical cohort study of 152 patients with gout assessed DECT of the hands, wrists, feet, ankles, and knees. The mean DECT volume pretreatment was 9.15 cm3, and the mean DECT volume posttreatment, after a mean of 12 months, was 1.89 cm3, representing a 95% reduction.47 Modjinou et al48 showed that DECT scans detected a 100% resolution of urate deposition in 3 index tophi over 6 months in a single-patient clinical study. Oral ULT was shown to reduce the DECT urate burden in 4 prospective studies.45,49-51
In a study with 29 patients with tophaceous gout, Chui et al49 demonstrated that DECT volume declined from a mean of 10.94 (SD 10.59) cm3 at baseline to a mean of 2.87 (SD 5.27) cm3 after being on allopurinol therapy for a mean of 20 months (P < 0.001), representing a 75.0% reduction. When serum urate values were > 0.43 mM/L (7.00 mg/dL), dissolution times approached infinity; when serum urate values approached zero, DECT dissolution was modeled to take 4 to 8 months.49 In the NOR-Gout (Gout in Norway) 2-year clinical cohort study, DECT of the feet and ankles was measured in 187 patients diagnosed by aspiration.50 The patient sample was 95.0% male with a mean age of 57 years, a mean disease duration of 8 years, and a mean baseline serum urate of 501 (SD 80) mM/L.50 Using allopurinol and febuxostat in a treat-to-target approach, mean serum urate values declined to 311 (SD 48) mM/L at 12 months and to 322 (SD 67) mM/L at 24 months. The percentage of patients with clinical tophi declined from 16.6% at baseline to 11.3% at 1 year and to 9.1% at 2 years; DECT volumes declined in parallel, with study-specific DECT scoring at 1 year and 2 years (P < 0.010 for both). Dalbeth et al45 studied patients receiving allopurinol in a randomized trial comparing immediate titration to maintain serum urate of < 0.36 mM/L to standard allopurinol dosing for 1 year then titration from year 1 to 2. DECT of the feet and ankles was read by 2 independent readers who were blind to treatment; DECT was evaluated in 87 subjects at baseline and at year 2. There was a substantial reduction in serum urate, with > 69.0% of patients reaching serum urate targets of < 0.36 mM/L, with DECT volume declining over 20.0% across the 2 years (P < 0.001).45 Sun et al51 studied 44 patients with gout who were treated with allopurinol or febuxostat with or without probenecid. Among 42 men and 2 women with a gout duration between 1 and 9 years, baseline and follow-up DECT scans of the feet were obtained up to 24 months after baseline. In concert with serum urate decreases from a mean value of 516 µM/L to 360 µM/L, DECT volumes decreased approximately 50.0% from baseline (P < 0.020); treatment duration was a significant predictor of DECT resolution (P < 0.010).51
Limited information is available on the definition of a clinically important DECT volume. Pascart et al10 estimated the minimum DECT volume related to excess mortality risk in patients with a disease duration of 11 years; in that study, they showed that survivors had a mean DECT volume of 0.20 cm3, whereas nonsurvivors had a mean DECT volume of 0.40 cm3. They also reported that DECT volumes > 1 cm3 predicted a higher burden of comorbid conditions (AUC = 0.84). The 1-cm3 threshold separated patients with gout into groups with and without hypertension, diabetes, and chronic heart failure.10 Pascart et al46 showed that DECT volume was related to future gout flares; mean DECT volumes were 2.40 (SD 2.10) cm3 for patients with ≥ 1 flare and 0.90 (SD 1.30) cm3 among those without flares (P = 0.006). From these results, the authors suggested that the minimum DECT volume predicting flares was 0.81 cm3. Dalbeth et al45 found that patients with flares over a 2-year interval had a mean DECT volume of 2.60 cm3 (95% CI 2.30-3.00) as compared to those without flares who had a mean DECT volume of 2.10 cm3 (95% CI 2.00-2.20; P < 0.001). Thus, a DECT volume difference of 0.50 cm3 may be important at a population level. Rajan et al52 has shown that the smallest detectable difference in DECT of the feet over 12 months is 0.91 cm3. Since the minimum important volume of DECT must be larger than the smallest detectable difference, a value of 1.00 cm3 is tentatively proposed as the minimum important difference for DECT. The minimum clinically important DECT volume for improvement or worsening of disability has not been reported.
DISCUSSION
This systematic review showed that DECT images are reliably interpreted to a great extent with intrarater ICCs from 0.86 to 1.00. The stage of gout (ie, early, middle, or late) does not influence this level of reliability. DECT overall has very good sensitivity and specificity in established gout when compared with joint aspiration, with ranges from 0.78 to 0.89 and 0.84 to 1.00, respectively. DECT also performed very well against clinical criteria, with a pooled sensitivity and specificity of 0.81 (95% CI 0.77-0.86) and 0.91 (95% CI 0.85-0.95).19 Singh and colleagues34 reported that DECT of the ankles and feet performed as well as, or better than, DECT of multiple locations, such as the ankles and the feet and knees combined. This is consistent with Mallinson et al53 who showed that DECT is most likely to be abnormal at the ankles and feet. Further work should confirm whether DECT of the feet and ankles alone is preferred over scanning additional areas that are involved clinically.
DECT in early gout has reduced sensitivity but its specificity is preserved, as compared to established gout. Lee et al31 reported sensitivities from 0.51 and 0.53 for 2 readers, with early gout defined by the absence of signs of established gout or lack of ULT. Zhang et al30 defined early gout as less than 1 year from first symptoms, with DECT sensitivities of 0.27 for early gout, 0.75 for middle gout, and 0.90 for late gout. Zhang et al30 suggested that ultrasound had better sensitivity than DECT in early gout, with values of 0.67 and 0.27, respectively, using the gold-standard clinical procedure of joint aspiration. Shang and colleagues18 showed that DECT of early gout cases had a pooled sensitivity of 0.75 (95% CI 0.60-0.86) and a pooled specificity of 0.85 (95% CI 0.75-0.91), whereas ultrasound had a pooled sensitivity of 0.93 (95% CI 0.72-0.99) and a pooled specificity of 0.80 (95% CI 0.71-0.86). It may be beneficial for future studies of early gout to use a standard definition, such as time from first symptoms or the absence of clinical signs and symptoms. More head-to-head studies of DECT and ultrasound in early gout are needed to confirm benefits. Ahn and colleagues54 suggested that DECT is less sensitive in early gout since MSU crystals in synovial fluid have a low density, reducing resolution. To illustrate this, Ahn et al54 collected patient-derived solid and liquid tophi from 3 patients at surgery. DECT did not detect urate deposition in liquid tophi at any urate concentration, whereas solid tophi were easily detected.54 Based on the lower sensitivity of DECT in early gout and considering that more studies of ultrasound in early gout are needed, when symptoms are less than 2 years in duration, it is recommended that clinicians aspirate joints preferentially, including when a DECT scan is negative.
Clinical tophi predict excess CV and all-cause mortality,11,40 and DECT scans also predict41 CV and all-cause mortality in prospective cohorts. Since up to 50.0% of patients without clinical tophi or abnormal serum urates have abnormal DECT scans, confirming the mortality relationship to DECT is important. DECT was shown to be associated with CV risk scores in 5 out of 6 studies examining this relationship.8,10,41-43
Clinical tophi correlate with hand disability.39 We did not find studies on the relationship of DECT volumes and disability for the hands, feet, ankles, or knees, although a relationship seems probable. These studies should be performed.
A relationship between DECT volume and future gout flares was found in 4 studies8,12,45,46; DECT volume predicted flares at 6 months46 and 2 years.45 No studies were found on DECT volume and its relationship to chronic gouty arthropathy.
This systematic review found DECT volume to be very sensitive to change with effective ULT, supporting DECT use in clinical studies and in the clinic as an outcome measure. The minimum important volume of DECT is tentatively set at 1.00 cm3, a value that seems to predict death, CV risk factor burden, and future gout flare risk; however, this threshold only considers DECT volume in the feet and ankles and not in areas such as the hands, wrists, and knees. Further work on defining the minimum important value should be undertaken.
To the best of our knowledge, there are no prior systematic reviews of DECT volume and its prognostic ability. Still, this systematic review has several limitations. The conclusions are limited by the quantity and quality of the current literature. Most of the literature relating to DECT reliability has shown it to be excellent. The diagnostic performance of DECT and ultrasound in early gout requires more study where DECT sensitivity appears lower. The prognostic value of DECT abnormalities in the absence of clinical tophi is not fully defined but is important, as up to 50.0% of patients with gout have an abnormal DECT scan without clinical tophi or abnormal serum urate levels. We found limited literature on the relationship of DECT to disability. We also found limited literature on the minimum important change in DECT.
A large, properly powered, prospective cohort study should be performed that includes early and established gout, patients with and without clinical tophi, patients with and without abnormal DECT scans, both males and females, and patients with and without controlled hyperuricemia to better understand DECT’s prognostic potential. DECT scans of the feet, ankles, knees, hands, and wrists could inform on near-term outcomes, such as joint pain (ie, chronic pain and acute flares) and hand and foot disability. Better characterization of the relationship of DECT-measured urate volume with mortality would be welcome; a large New Zealand gout cohort saw separation in mortality rates between participants with and without tophi in as early as 1 year.11 Ideally, DECT and ultrasound would be contrasted further to better understand their respective prognostic abilities.
DECT is a promising prognostic tool in gout. It has excellent reliability with good diagnostic test performance in established gout. It is very sensitive to change with effective ULTs, supporting its use as a clinical outcome measure. DECT appears to have a reduced sensitivity in early gout, and joint aspiration should be undertaken preferentially when disease duration is less than 2 years, including when DECT is negative. Based on current evidence showing that DECT volumes predict mortality and gout flares, DECT should be used to stage patients with gout, especially in established disease, as 50.0% of patients have abnormal DECT scans with normal serum urate levels and no clinical tophi.
ACKNOWLEDGMENT
Editorial assistance was provided by Amy Cohen, PhD, a Horizon employee.
Footnotes
This study was supported by Horizon Therapeutics plc, Deerfield, IL, USA. Horizon Therapeutics funded the collection of retrospective deidentified chart data and contributed to the analysis, data interpretation, and writing, review, and approval of the manuscript.
PMP is a former employee of Horizon Therapeutics plc and holds company stock. SKS declares no conflicts of interest relevant to this article.
- Accepted for publication June 30, 2022.
- Copyright © 2022 by the Journal of Rheumatology
This is an Open Access article, which permits use, distribution, and reproduction, without modification, provided the original article is correctly cited and is not used for commercial purposes.








{kind=link}