

Abstract
Objective To explore quality of life (QOL) using the individualized Patient Generated Index (PGI) in young adults who were diagnosed with juvenile idiopathic arthritis (JIA) in childhood, and to examine associations between PGI ratings and standardized health-related outcome measures.
Methods Patients (N = 79, mean age 25.1 [SD 4.2] yrs, 72% female) completed the PGI and the standardized measures: Health Assessment Questionnaire–Disability Index, 12-item Short Form Health Survey (SF-12; physical and mental health-related QOL [HRQOL]), Brief Pain Inventory (pain severity and interference), 5-item Hopkins Symptom Checklist, and visual analog scale for fatigue. Information on morning stiffness, medications, and demographics was also collected. Patients were compared to 79 matched controls.
Results The most frequently nominated areas of importance for patients’ personally generated QOL (assessed by PGI) were physical activity (n = 38, 48%), work/school (n = 31, 39%), fatigue (n = 29, 37%) and self-image (n = 26, 33%). Nomination of physical activity was associated with older age, morning stiffness, and more pain interference. Nomination of fatigue was associated with current use of disease-modifying antirheumatic drugs, whereas nomination of self-image was associated with polyarticular course JIA and pain interference. Nomination of work/school was not associated with other factors. Higher PGI scores (indicating better QOL) correlated positively with all SF-12 subscales except role emotional, and negatively with disability, pain severity, pain interference, and morning stiffness. Compared to controls, patients had more pain, poorer physical HRQOL, and less participation in full-time work or school.
Conclusion Physical activity, work/school, fatigue, and self-image were frequently nominated areas affecting QOL in young adults with JIA. The PGI included aspects of QOL not covered in standardized measures.
Juvenile idiopathic arthritis (JIA) is a chronic inflammatory disease with variable course and outcome that occurs in children under the age of 16 years,1 and continues into adulthood in approximately half of the patients.2-4 A major goal of treatment is to achieve the best possible quality of life (QOL), continuing into adulthood. However, information on such long-term outcomes is scarce.
Patient-reported outcome measures (PROMs) assess outcomes reported by patients without interpretation by anyone else.5 A variety of valid and reliable standardized PROMs have found JIA to have long-term effects on pain, physical function, QOL, and other relevant outcomes.2,6-10 Although many PROMs are multidimensional, they may include factors irrelevant to patients and omit important aspects. Thus, additional QOL measures may be needed to facilitate a comprehensive perspective of important aspects in the lives of patients with JIA.
Individualized measures are generated from the patient’s own definition of the outcome being measured11 and may capture relevant aspects not assessed by standardized PROMs. The Patient Generated Index (PGI) is an individualized measure designed to capture aspects important to the individual’s QOL by letting the respondents identify their own areas of importance, rate their function in these areas, and prioritize their desire for improvements in these areas.12,13 QOL can be defined as the individual’s perception of their position in life within the context of the culture and value system in which they live, and in relation to their goals, expectations, standards and concerns.14 Studies based on an individualized approach assessing QOL outcomes in adults with JIA have been restricted to focus group interviews and open-ended questions. Such studies found employment challenges in young adults with JIA15 and reduced quality of activity engagement due to functional limitations.16 To our knowledge, validated individualized measures such as the PGI have not been used previously in adults with JIA.
Previously, we presented results from a study on patient-reported outcomes in adults with JIA based on standardized PROMs.6 However, to achieve a broader understanding of the long-term effect of JIA on patients’ lives, the aims of our present study are to explore QOL using the individualized PGI and to explore the associations between PGI ratings and standardized measures of health-related outcomes in young adults diagnosed with JIA in childhood.
METHODS
The sample was recruited from a cohort of 192 patients who participated in a longitudinal study at Oslo University Hospital between 1995 and 2003.6,17 Patients were classified according to the International League of Associations for Rheumatology criteria for JIA (based on clinical examinations during the first 3 years after the first visit) and had < 18 months disease duration at inclusion.17,18 Disease onset was defined as the day a physician documented symptoms or signs of JIA.18 Invitations to participate in this follow-up study were sent to the patients by post. Controls matched for age and gender (randomly selected from the National Registry) were included to evaluate the effect of JIA on patients’ health. The Regional Committees for Medical and Health Research Ethics approved the study (#2015/532). Informed consent was obtained in accordance with the Declaration of Helsinki and study questionnaires were delivered and returned by post.
Measures. Information regarding JIA diagnosis and age at disease onset was assessed from patients’ medical records. Use of medication, time since last rheumatologist visit, duration of morning stiffness, and number of active joints were assessed with self-report questionnaires. Physical disability was assessed by the Health Assessment Questionnaire–Disability Index (HAQ-DI), with items on dressing, arising, eating, walking, hygiene, reach, grip, and activities. Scores range from 0 to 3, with 0 indicating no disability.19,20
Personally generated QOL was assessed by the individualized PGI questionnaire and completed in 3 parts.12,13 In part 1, patients were asked to list the 5 most important areas of their life affected by their rheumatic condition. To facilitate completion, a trigger list of examples was presented: walking, completing tasks, emotions, housework, hobbies, identity, travel, sexuality, relations, self-image, socialization, pain, stiffness, sleep, fatigue, and getting started in the morning. In part 2, patients rated each area listed in part 1 on a 7-point scale ranging from “as bad as it could be” (severity score of 0) to “as good as it could be” (severity score of 6). In part 3, patients allocated 10 points among the areas listed in part 1, based on their priorities for improvement (if only 1 area is listed, it is given all 10 points). The PGI overall score is calculated as follows: [∑(area score from part 2 × assigned points from part 3/10)]/6 × 100, with an overall score ranging from 0 to 100, and higher scores indicating better QOL13 (Table 1). If patients nominated more than 1 item in the same area (eg, skiing and lifting weights, both of which are types of physical activity), the mean of the item severity ratings was used in the scoring of that area. The Norwegian version of the PGI has been found to be valid and reliable in patients with rheumatic disease (RD).13,21
Example of scoring the Patient Generated Index (PGI) based on 1 participant.
Both patients and controls answered a multiple choice questionnaire regarding age, gender, formal education, and occupation, as well as the following standardized measures: the 12-item Short Form Health Survey (SF-12; subscales: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health), summarized into physical and mental component summary (PCS and MCS, respectively) scores, with higher scores indicating better health22; Brief Pain Inventory (BPI; including pain severity and interference); 10-cm visual analog scale (VAS) for fatigue; and 5-item Hopkins Symptom Checklist (SCL-5) measuring signs of anxiety and depression. For all, higher scores indicate worse symptoms.23-25 All these standardized questionnaires are widely used and have satisfactory reliability and validity.22,24-27
Statistical analysis. Data were analyzed using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp). Descriptive statistics included absolute frequencies and percentages for categorical variables and mean, median, SD, and range for continuous variables. Comparisons between groups were performed using Fisher exact test, independent sample t tests or Wilcoxon-Mann tests. Correlations between PGI scores and scores on standardized PROMs were expressed by Pearson correlation coefficient (r): r < 0.30 was considered low, and r ≥ 0.30 to 0.49 moderate.28 Logistic regression analyses were conducted to identify correlates of the frequently nominated PGI areas of physical activity, fatigue, and self-image. Variables from the univariate analyses with P < 0.20 were included in the multiple regression analyses (manual backward regression method). P < 0.05 indicated statistical significance.
RESULTS
Study population. A total of 96 patients (50%) participated 16.5 to 21.4 (median 19.2) years after disease onset, of whom 79 (82%) completed the PGI. Demographic and clinical characteristics of participants, nonparticipants, and 79 matched controls are presented in Table 2.
Demographic and health-related characteristics of nonparticipants, participating patients, and controls, as well as clinical characteristics of patients 16.5 to 21.4 years after disease onset.
No significant differences were found between the 79 patients who completed the PGI and the 17 who did not regarding age, current use of disease-modifying antirheumatic drugs (DMARDs), physical disability (HAQ-DI) or physical HRQOL (SF-12 PCS). However, the participants had more pain (BPI severity and interference), symptoms of psychological distress (SCL-5) and fatigue (VAS), and lower scores on mental HRQOL (SF-12 MCS), presence of active joints, and > 10 minutes of morning stiffness (all P = 0.01-0.04). Females and patients with polyarticular course JIA were more likely to complete the PGI (89% of females vs 69% of males, and 93% of patients with polyarticular course JIA vs 75% without polyarticular course JIA, P = 0.02 and 0.03, respectively; Table 2).
The most common JIA categories among the 79 participants were persistent oligoarthritis (38%, n = 30), rheumatoid factor–negative polyarthritis (29%; n = 23) and extended oligoarthritis (11%; n = 9). Eighteen patients (23%) had not been examined by a rheumatologist during the last 10 years, 49 (62%) had not been examined during the last 2 years, and 46 patients (58%) reported current use of DMARDs.
Comparison of 79 patients and controls. The median HAQ-DI score was 0 (range 0-2.13) and 41 patients (52%) had an HAQ-DI score of 0 (Table 2), indicating no disability. Compared with controls from the general population, patients with JIA had more pain (BPI, pain severity, and interference) and poorer physical HRQOL (SF-12 PCS), all P < 0.001. No differences were found between patients and controls regarding mental HRQOL (SF-12, MCS), level of psychological distress (SCL-5), fatigue, level of education, or full-time participation in work or school.
JIA impact on QOL based on the individualized PGI measure. The mean (SD) PGI overall score was 47.6 (23.3; Table 2). The mean number of important areas nominated as being affected by the patients’ rheumatic condition was 4, with 38 patients listing 5 areas and 5 patients listing only 1. Three patients indicated that their RD affected no areas, and these were given the highest PGI score of 100.
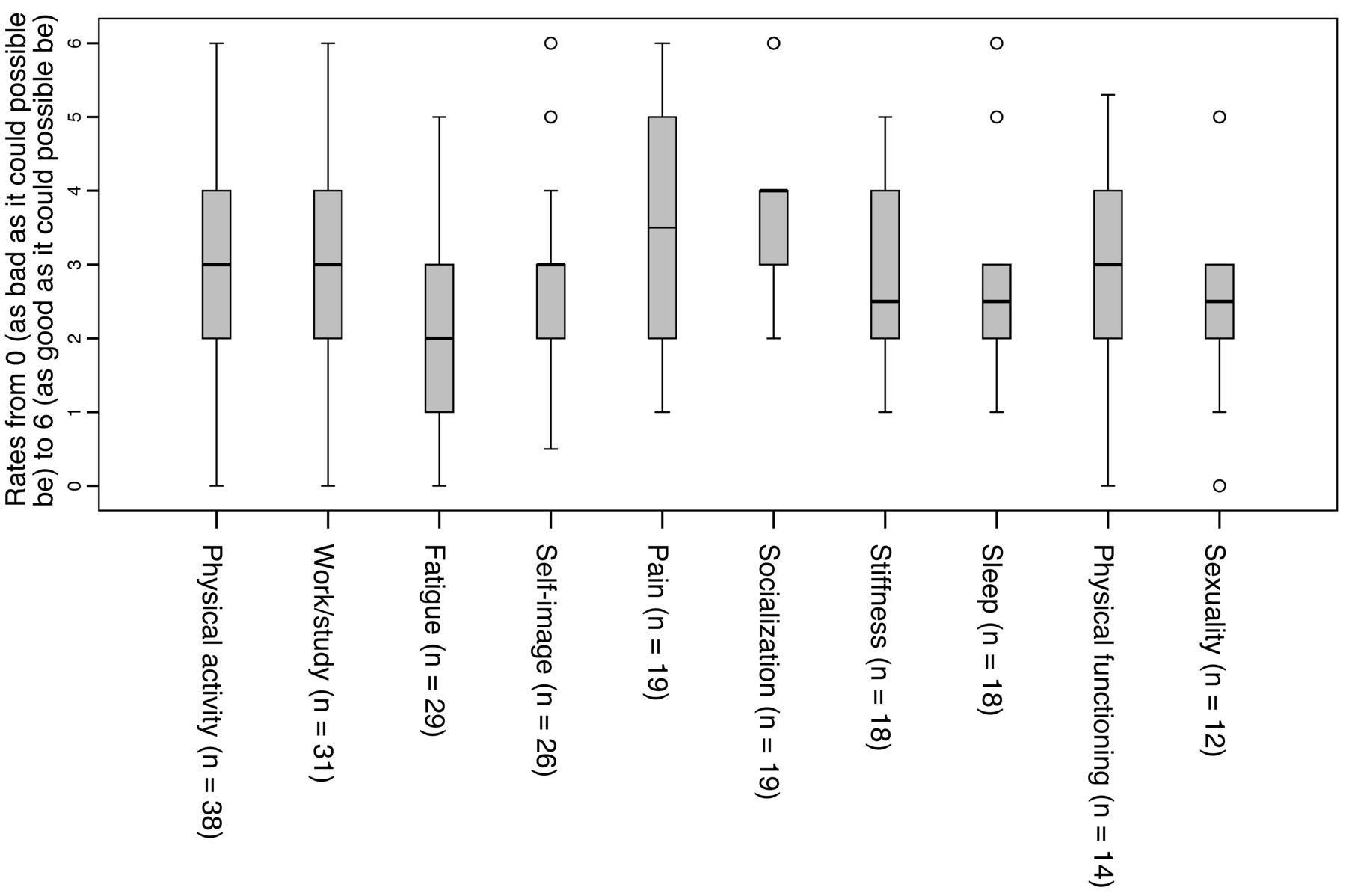
Physical activity (PA; eg, long walks, hiking, skiing, playing football, running, lifting weights) was the area affected by JIA reported most often and was reported by 38 respondents (48%), of whom 5 nominated 2 items related to PA. A total of 31 respondents (39%) reported participation at work or school was affected by JIA, of which 3 nominated 2 items related to work or school. Fatigue was reported by 29 respondents (37%) and 26 (33%) reported self-image (Figure 1). Based on the 7-point rating scale used in part 2 of the PGI, the mean (SD) severity scores for PA, work or school, fatigue, and self-image were 2.8 (0.4), 3.1(1.4), 2.3 (1.3) and 2.9 (1.2), respectively (Figure 2). In part 3 of the PGI, 12 patients (15%) reported PA to be their highest priority for improvement, 9 reported fatigue, 7 reported work or school, and 2 reported self-image.
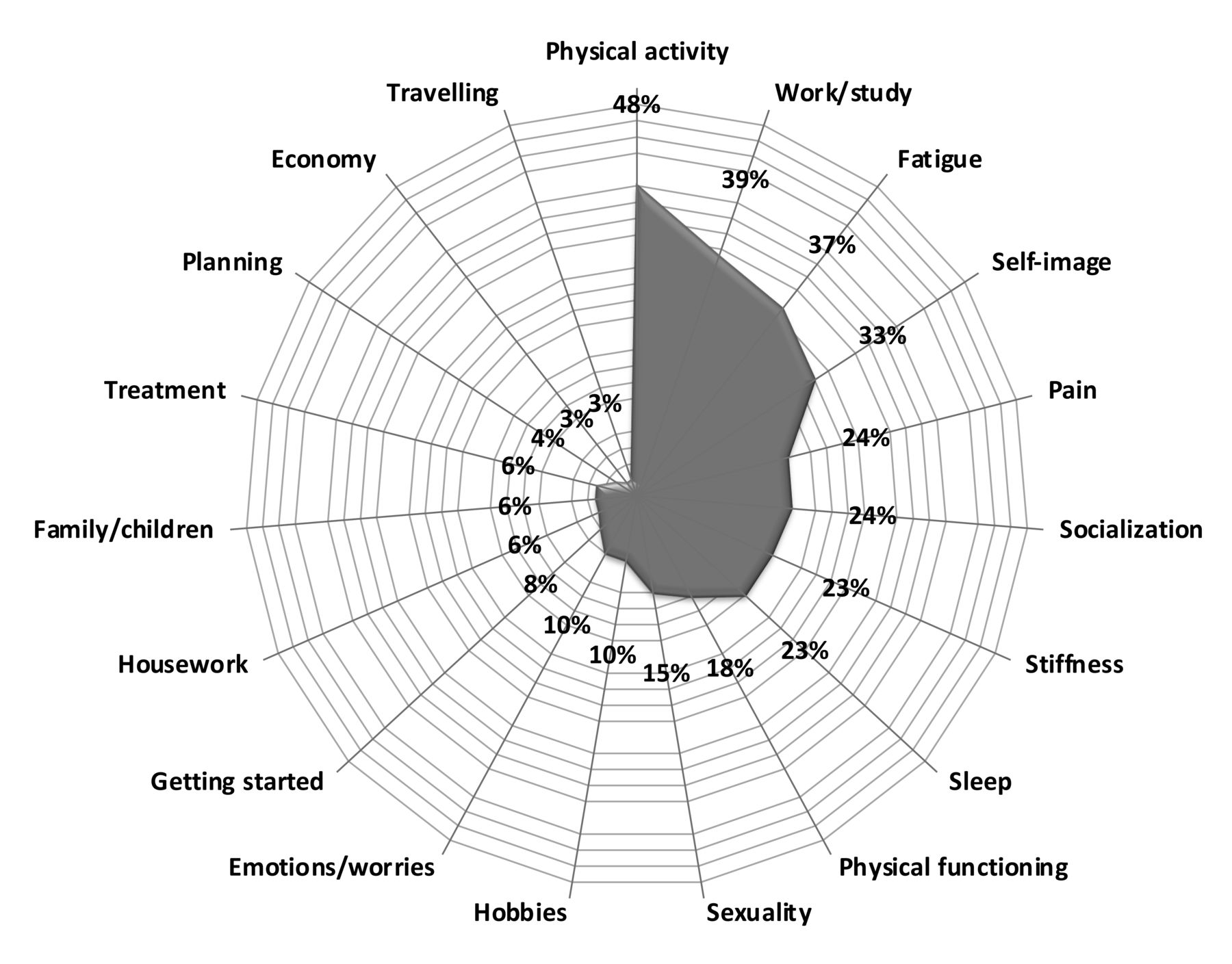
Areas of life nominated as important in part 1 of the Patient Generated Index by 79 adults with juvenile idiopathic arthritis. Numbers presented in the figure are the percentage of patients who nominated the area as being among the 5 most important areas affected by their rheumatic condition.
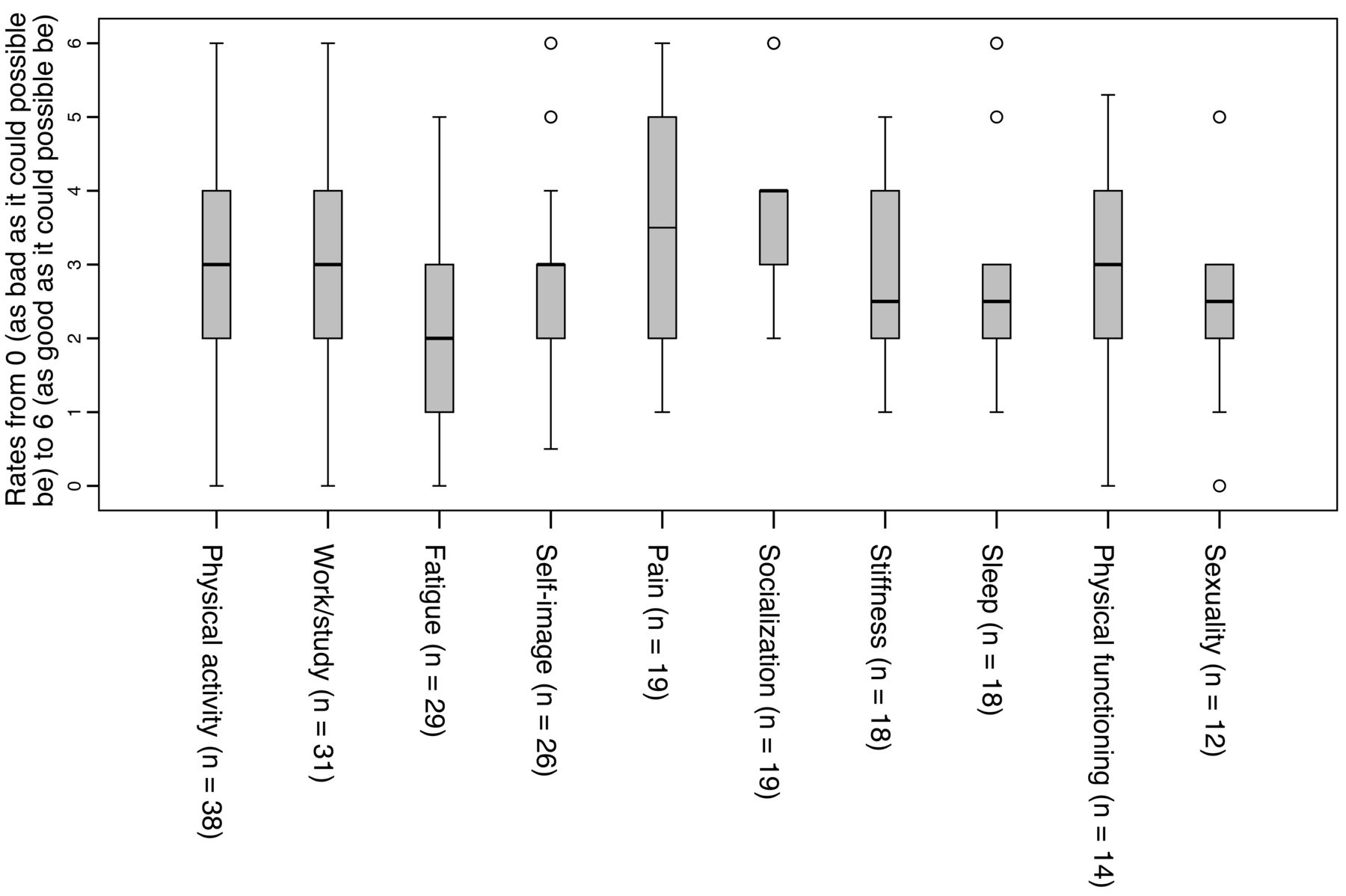
Patient Generated Index part 2 severity scores for most commonly nominated areas affected by JIA. Median severity score on commonly nominated areas affected by JIA in patients 16.5 to 21.4 years after disease onset. JIA: juvenile idiopathic arthritis.
No correlation was found between PA nomination in part 1 of the PGI and physical disability (HAQ-DI). Among the 38 patients who nominated PA as an important area affected by JIA, 21 (55%) reported no physical disability (HAQ-DI = 0), 16 (42%) did not currently use DMARDs, and 14 (37%) had not visited a rheumatologist during the last 2 years. Six of the 31 patients who nominated work or school as being an important area affected by their RD were currently receiving social benefits. A higher proportion of females compared to males nominated fatigue as being an important area (37% vs 5%, P = 0.04), but no gender differences were found in PA, work or school, or self-image nominations (P = 0.13-0.62).
Other frequently nominated areas in part 1 of the PGI were pain (n = 19, 24%), socialization (including playing with children; n = 19, 24%), stiffness (n = 18, 23%), sleep (n = 18, 23%), physical functioning (including walking, writing, carrying children, sitting on the floor; n = 14, 18%) and sexuality (n = 12, 15%; Figure 1). The PGI part 2 severity scores of the most frequently nominated areas in part 1 are presented in Figure 2.
Correlations between clinical variables, PROMs, and PGI overall scores. We found positive associations between PGI overall scores and scores on SF-12 PCS and all SF-12 subscales except role emotional (r range: 0.23-0.41, P range: < 0.001 to 0.04; Table 3). Negative associations were found between PGI overall scores and physical disability (HAQ-DI), pain (BPI severity and interference), and morning stiffness (r range: −0.338 to −0.415, P range: < 0.001 to 0.002).
Correlations between PGI overall scores and scores on standardized health- and disease-related measures in patients with JIA (n = 79).
Relationship between health- and disease-related variables and the most frequently nominated areas in PGI part 1. Results from the univariate analysis showed a positive correlation between age and nomination of PA (Table 4). In the multiple regression analyses (adjusted for age and gender), age, morning stiffness, and pain interference were associated with patients’ nomination of PA. No significant association was found between health- and disease-related variables and the nomination of work/school. Female gender and current use of DMARDs were associated with the nomination of fatigue in univariate analyses, but only current use of DMARDs remained significant in multiple regression analysis. Polyarticular disease course and pain interference were associated with patients’ nomination of self-image both in univariate analyses and multiple regression analysis (adjusted for age and gender).
Relationships between health- and disease-related variables and PGI nomination of physical activity, fatigue, and self-image as important areas affecting quality of life in 79 patients with JIA.
DISCUSSION
In this sample of young adults diagnosed with JIA as children, PA, work or school, fatigue, and self-image were the areas nominated most frequently as being affected by their RD. Age, morning stiffness, and more pain interference were associated with nomination of PA. Current use of DMARDs was associated with patients’ nomination of fatigue, whereas polyarticular course JIA and pain interference were associated with patients’ nomination of self-image. No significant associations were found regarding patients’ nomination of work/school. The PGI overall score correlated positively with all subscales of SF-12 except the role emotional subscale, and correlated negatively with physical disability, pain, and morning stiffness.
The PGI has been used previously in patients with other RDs13,21,29; however, this is the first study reporting QOL based on the PGI in patients with JIA, to our knowledge. We found that almost half the patients (48%) reported that their ability to participate in PA was affected by their RD, despite 55% of them having a HAQ-DI score indicating no physical disability (HAQ-DI = 0). However, previous studies indicate that patients with mild functional disabilities could have a HAQ-DI score of 0 due to possible floor effects.20,30 PA can be defined as “any bodily movement produced by skeletal muscles that results in energy expenditure,”31 and may include many different activities with different levels of intensity. Whether the patients had difficulty performing a certain activity or problems with the duration or intensity of the activity could unfortunately not be determined by our assessments. The effect of inflammatory arthritis on PA has been reported in previous studies on children and adolescents with JIA as well as in adults with rheumatoid arthritis (RA),32-35 supporting the findings of our study. We found an association between older age, pain interference, and morning stiffness and nomination of PA. Previous studies have found that PA level in childhood may influence PA level in adulthood,36,37 and previously recommended restrictions on PA in children with active disease could be an explanation for the effect of age.38 Today JIA children with and without active disease are encouraged to be physically active and PA is considered to be an important part of everyday life.39 Children with JIA and controls were previously reported to have comparable levels of light and moderate PA,40 and experience with PA in long-term JIA may therefore be different in the future due to improved treatment regimens and increased focus by healthcare providers on the importance of PA. Similar to other studies, we found an association between pain and PA. Bos et al34 found associations between pain and low PA in patients with JIA, and in a review article on adults with RA,41 pain was a commonly identified disease-specific barrier to participation in regular PA. We also found an association between patients’ nomination of PA and morning stiffness, which is a common symptom of JIA and associated with active disease.42 Identification of barriers to PA in patients with inflammatory arthritis have not been conclusive; previous studies have reported no association between PA and disease activity in children with JIA.32-34 However, disease-related symptoms, such as pain, fatigue, physical disability, and morning stiffness, have been identified as barriers to PA in adults with RA.41 Among the 38 patients nominating PA as an important area affected by their RD, 42% were not using DMARDs and 37% had not visited a rheumatologist during the previous 2 years. Patients’ reasons for not using DMARDs or visiting a rheumatologist are unknown, and since no physical examinations were performed at 19-year follow-up, the patients’ disease status is unknown.
Thirty-one patients (39%) nominated work or school as being affected by their RD. This result is in line with other studies of employment experiences and occupational outcome in young adults with JIA.7,9,15,43,44 In our study, no significant associations were found between nomination of work or school and demographic or disease-related variables. Possible reasons for this could be that factors other than the variables assessed in our study have a greater effect on patients’ work or school experience, as well as insufficient statistical power due to the moderate sample size.
Fatigue was also frequently nominated by the patients in our cohort (n = 29, 37%), and was associated with current use of DMARDs. This result is in accordance with a recently published study by Arnstad et al, who found fatigue to be a prominent symptom in JIA 18 years after disease onset.45 In their study, associations were found between fatigue and female sex, physical disability, and current use of DMARDs.45 Although different measures were used, this indicates that fatigue is a prominent consequence of JIA in young adults with an effect on everyday life.
Self-image can be defined as the perceptions of one’s body, personality, and capabilities,46 and a total of 26 patients (33%) reported JIA to have an effect on their self-image. Tong et al found striving for normality to have an impact on the development of self-image in children with JIA,47 and almost 20 years ago, Packham et al reported JIA to have a detrimental effect on patients’ perception of themselves 28 years after disease onset.48 In adults with RA, worse body image was found in patients than controls with a negative effect on patients’ QOL.49 We found associations between nomination of self-image as an area affected by JIA and both polyarticular disease course and patients’ pain interference scores. Similarly, associations between body image and pain have been reported in adults with RA.50 Self-image has received little attention in both children and adults with JIA and warrants further research.
The correlations between the PGI overall score and other assessed variables were moderate or weak. This might be due to the heterogeneous way that health problems affect adults with JIA or to the standardized measures omitting questions that are important to patients, which supports the use of an individualized questionnaire. Positive associations were found between PGI and SF-12 scores. Compared with the SF-12 PCS and MCS scores, the PGI scores were at the lower end of the scale. One reason for this may be that the PGI is deficit-oriented and captures areas of concerns for the respondents, whereas the respondents may not have deficits or concerns identified in connection with the preselected areas of the SF-12. The standardized questionnaires used in our study are generic or developed for adults with RDs and enable comparisons between different groups; however, they were not specifically developed for patients with JIA. There is also no defined cut-off point categorizing PGI scores into good vs poor QOL, and the overall score from our study is therefore not comparable with other studies. However, PGI scores were included to analyze the associations between this personally generated outcome and other standardized measures. Patient-nominated items are important and may contribute relevant information not necessarily reflected in standardized measures. The trigger list presented in the PGI could create a possible priming effect on patients’ nomination of areas. However, it should be noted that the most frequently nominated areas of PA and work or school were not on the trigger list; thus, these areas may be underreported.
In our study, 17 patients did not answer the PGI. Although the reasons some individuals did not complete the PGI are unknown, it is possible that they were either more or less affected by JIA than those who did complete the PGI. Despite no difference being found between the 79 participants and the 17 nonparticipants with respect to physical HRQOL, physical disability, and current use of DMARDs, the participants reported more pain, fatigue, psychological distress, active joints, and lower mental HRQOL. The experience of more health-related symptoms among the participants may have an effect on the external validity of our results. Additionally, the patients in our cohort were referral-based, with an increased probability of including participants with more severe disease compared to population-based cohorts. However, our cohort’s patient characteristics were comparable to those of population-based studies,2,10 and a large proportion of the participating patients did not use DMARDs.
The main limitations of this study are that the patients were not evaluated by a physician and blood tests were not performed as part of the long-term follow-up, so we cannot draw conclusions about patients’ disease activity. Moreover, information was not collected about patients’ comorbidities that could influence their health and QOL beyond JIA. The results of this study are based solely on patient-reported health and QOL, which are clearly important but may be subject to over- or underreporting and are likely insufficient for estimating disease activity.
Despite these limitations, this study reveals important insights on long-term outcomes for young adults with JIA by capturing aspects not included in traditional standardized PROMs. In conclusion, individualized measures can provide important information on the consequences of JIA in patients’ lives by including aspects of QOL not assessed in standardized measures. The most frequently nominated areas having an impact on QOL in young adults with JIA were PA, work or school, fatigue, and self-image. Further research should, in addition to standardized measures, include individualized measures to gain more insight and achieve a broader understanding of the effect of JIA on patients’ lives.
ACKNOWLEDGMENT
The authors thank Caryl Gay at the University of California, San Francisco, as well as the Lovisenberg Diaconal Hospital in Oslo for useful comments on the manuscript.
Footnotes
The project was supported by the Norwegian Foundation for Health and Rehabilitation and has not received financial support from any commercial source.
The authors declare no conflicts of interest relevant to this article.
- Accepted for publication May 2, 2022.
- Copyright © 2022 by the Journal of Rheumatology
This is an Open Access article, which permits use, distribution, and reproduction, without modification, provided the original article is correctly cited and is not used for commercial purposes.








{kind=link}
{kind=link}