

Abstract
Objective To determine whether the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) and the Ankylosing Spondylitis Disease Activity Score (ASDAS) exhibited differences between women and men.
Methods We systematically searched MEDLINE, Embase, Web of Science, and other sources in English or Spanish from January 1, 1995, to July 31, 2020, to assess the differences according to sex in BASDAI and ASDAS. We performed a comparative analysis by sex using t test and mean difference by sex metaanalyses for BASDAI and ASDAS, as well as a random-effects model using the inverse-variance method.
Results Forty-one studies included BASDAI (6785 women, 12,929 men) and 16 of them included ASDAS (2046 women, 4403 men). Disease activity detected using BASDAI was significantly higher in women than in men (mean 4.9 vs 4.2, P = 0.02), whereas ASDAS did not detect differences between sexes (mean 2.8 women vs 2.8 men). In the metaanalyses, BASDAI detected significant differences between women and men (mean difference = 0.55 [95% CI 0.46–0.65], P < 0.00001), but ASDAS did not identify significant mean difference between sexes (0.04, 95% CI –0.05 to 0.12], P = 0.38).
Conclusion The 2 most widely used indices of disease activity in spondyloarthritis (SpA) discriminate differently according to sex by their different evaluations of peripheral disease. The different components and weights in BASDAI and ASDAS influence their values. BASDAI may be affected by fatigue, and in predominantly peripheral manifestations such as enthesitis, ASDAS may not be sensitive enough to detect activity. This may represent a sex bias unfavorable to women, because peripheral SpA is more common in women than in men.
Spondyloarthritis (SpA) is a group of diseases presenting different clinical manifestations. In 2009, the Assessment of SpondyloArthritis international Society (ASAS) developed new classification criteria based on the main clinical presentation of predominantly axial SpA (axSpA), covering patients with radiographic and nonradiographic sacroiliitis.1 Although chronic back pain is the main feature in this classification, other peripheral features may coexist. Two years later, ASAS developed criteria for peripheral SpA, for patients predominantly presenting arthritis, enthesitis, or dactylitis.2 Due to the variable nature of these manifestations, quantifying disease activity and response to treatment has been a challenge.
The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) was developed in 1994 to assess the activity of ankylosing spondylitis (AS).3 BASDAI includes 6 items reported by patients on a visual analog scale: fatigue, back pain, peripheral joint pain/swelling, enthesitis, and severity and duration of morning stiffness. In 2009, ASAS validated another tool, the AS Disease Activity Score (ASDAS),4 which includes 4 self-reported items: back pain, peripheral joint pain/swelling, duration of morning stiffness, and patient global assessment of disease activity, adding C-reactive protein (CRP) or erythrocyte sedimentation rate (ESR) as objective tests to measure inflammation. Each of the 5 elements contained in ASDAS has a different weight in the score, unlike BASDAI, in which the elements have the same weight. Both indices were developed using patients fulfilling the criteria for AS, but not peripheral forms of SpA, so their items reflect the involvement of axial forms. Figure 1 shows the weights of the different items for BASDAI and ASDAS.

Proportional contribution of the items to BASDAI and ASDAS. Comparison of the items identified by BASDAI with the equivalent items identified by ASDAS, considering their weights in each score. ASDAS: Ankylosing Spondylitis Disease Activity; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; CRP: C-reactive protein.
ASDAS is considered to cover disease activity better than BASDAI.5 The fact that ASDAS includes objective measures such as CRP or ESR increases the capacity of ASDAS to identify inflammation.6 Both BASDAI and ASDAS are commonly used and sensitive to disease improvement during the treatment of AS.7,8 They have also shown sensitivity to disease improvement in peripheral SpA.6,9 However, like BASDAI, ASDAS was validated using samples of predominantly male patients. Therefore, using these scores to determine disease activity according to sex can be regarded as controversial.10,11 BASDAI may overestimate disease activity in women12; indices for other diseases such as rheumatoid arthritis have shown similar overestimation.13 ASDAS, on the other hand, may not show differences between sexes in axSpA.12 However, 2 recently published papers diverge from the rest of the published literature, detecting differences between sexes in ASDAS, although one of them concluded that their sample was relatively small and it was not possible to carry out the stratified sex analysis for nonradiographic axSpA.14 The second paper, with no limitations described, showed that male and female patients with very high disease activity have differences in ASDAS at baseline,15 but as the ASDAS items were not described, we cannot identify which ASDAS components influence the sex differences.
Our aim in this study was thus to determine how BASDAI and ASDAS differed in their assessments of disease activity in women and men with SpA.
METHODS
Data sources and literature search. We conducted a systematic literature search using MEDLINE by way of Pubmed, Embase, and Web of Science from January 1, 1995, to July 31, 2020, to capture studies on patients with SpA that reported either BASDAI or ASDAS according to sex.
We performed a comprehensive search strategy using MeSH terms and text related to SpA, except psoriatic arthritis (PsA), combined with (“sex” OR “gender” OR “women” OR “woman”) AND (“disease activity” OR “BASDAI” OR “ASDAS”). Further, reference lists of the retrieved studies were hand-searched to identify additional potentially relevant publications. No study design restrictions were applied. The search strategies used for each database are online in Supplementary Data 1 (available with the online version of this manuscript).
Study selection. Two authors (MBB and VJ) independently reviewed and assessed the eligibility of the selected articles. A third author (MTRC) addressed potential discrepancies.
We selected studies that (1) included AS, axSpA, SpA, reactive arthritis, and enteropathic arthritis as main issues; (2) reported BASDAI and/or ASDAS according to sex; (3) were original research published in peer-reviewed journals; and (4) were written in English or Spanish. We excluded studies that did not meet the study criteria or in which (1) the main issue was PsA, as it has specific scores to measure disease activity,16 or (2) were editorials, reviews, meeting abstracts, assessments of questionnaires/scores, case studies, or involved < 10 participants of either sex.
In the case of multiple studies or samples derived from the same cohort, we selected the largest sample to avoid duplicate data.
Dealing with unsuitable and missing data. In studies where data were reported as medians and ranges, we estimated the means and SDs according to the literature.17,18 In studies that included subgroups, we combined them according to the Cochrane Handbook19 to obtain a single, larger sample. Moreover, when relevant data were missing, we contacted the authors to obtain more information.
Data extraction. We extracted the following information from each study: (1) study characteristics, including study design, sample size, patient source, country, classification criteria, and SpA type; (2) BASDAI and/or ASDAS according to sex, with baseline disease activity selected in follow-up studies; (3) patients’ characteristics according to sex, including current age in years, age at onset of the disease, age at diagnosis, disease duration, diagnosis delay, percentage of peripheral arthritis, Bath AS Functional Index (BASFI) score,20 Maastricht AS Enthesitis Score,21 CRP, percentage of HLA-B27–positive patients, BMI (kg/m2), and percentage of anti–tumor necrosis factor (anti-TNF) agents.
Quality assessment. Two authors (MBB and VJ) independently evaluated the methodological quality of the studies, and a third author (MTRC) resolved any discrepancies. We conducted the quality assessment according to the Newcastle-Ottawa Scale (NOS),22 which is a 9-item scale: 4 items evaluate the selection of the patients, 2 items the comparability, and 3 items are dedicated to the outcome or exposure. We adapted the scale to the topic of this review (Supplementary Table 1, available with the online version of this article).
Data analysis. First, we descriptively calculated means and 95% CIs for the demographic and clinical characteristics of the patients mentioned above. We compared women and men using t test after verifying their normal distribution. Statistical analysis was performed using SPSS v23.0 (IBM Corp.).
Second, we performed mean difference metaanalyses for BASDAI and for ASDAS and compared women’s mean disease activity with that of men. The inverse-variance method was used by all metaanalyses. Both the fixed- and random-effect models were assessed. RevMan v5.3 (Nordic Cochrane Centre, Cochrane, 2014) was used for these analyses.
To identify heterogeneity across studies, we assessed Cochran Q test and estimated the I2 statistic, considering values > 50% as subtantial heterogeneity in accordance with Deeks, et al.23 To detect any publication bias, we performed funnel plots and estimated the Egger regression test using Meta-Essentials v1.3 (Erasmus Research Institute of Management). To assess the robustness of the overall result, we conducted sensitivity analyses by consecutive deletion of (1) one study each time, and (2) one disease type (AS, axSpA and SpA) each time. All reported P values < 0.05 were considered statistically significant. No ethical approval was required for this study.
RESULTS
Initially, we identified 3660 records, 2 of them manually retrieved; among them, 136 full-text articles were evaluated for inclusion, and finally, 41 studies were included.14,15,24–62 Figure 2 shows the selection process. The reasons for excluding 95 articles evaluated in full text are detailed in Supplementary Data 2 (available with the online version of this article). Regarding the information obtained from authors themselves, 3 authors kindly provided us with data.29,42,53
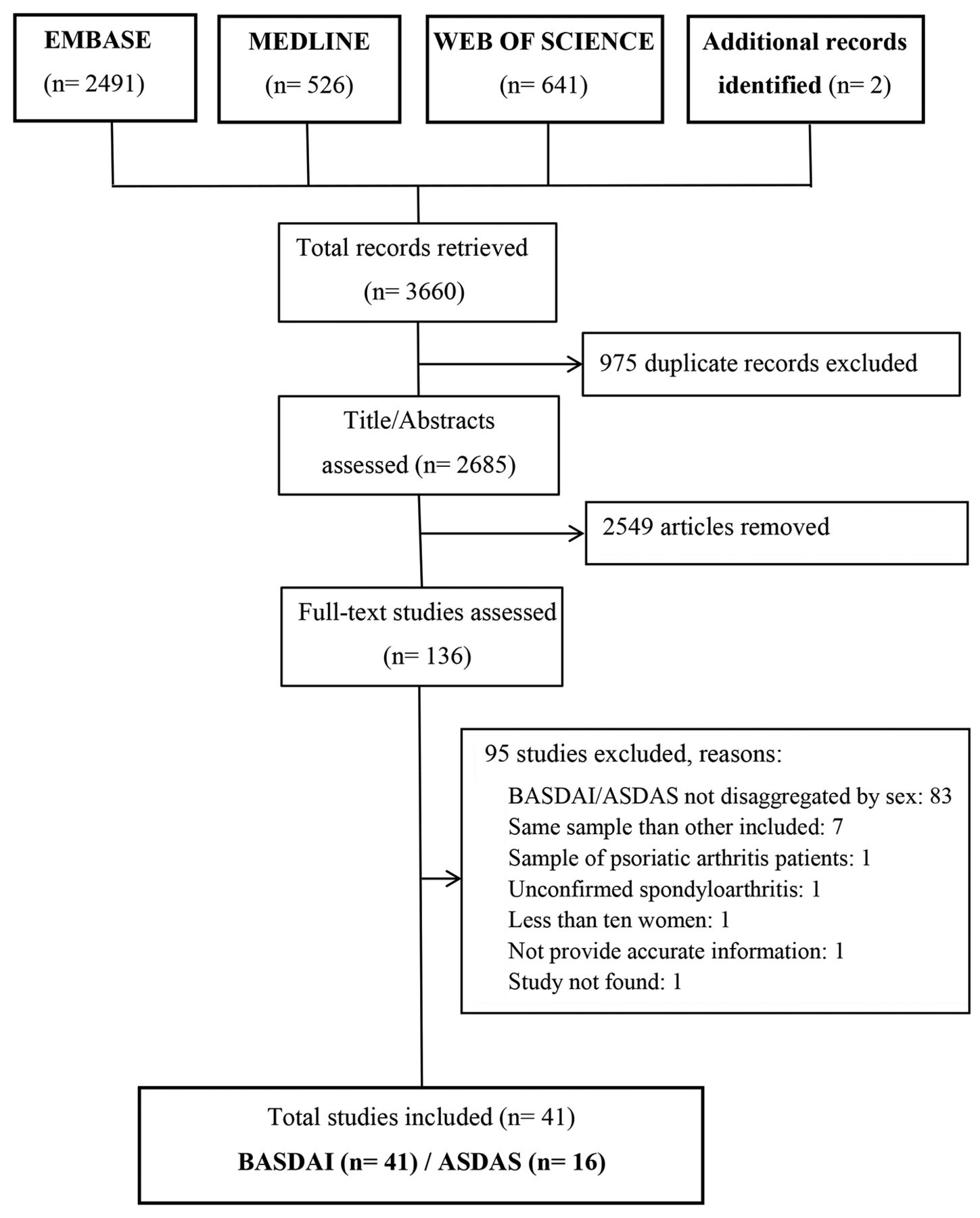
Flowchart diagram. Results of the literature search. ASDAS: Ankylosing Spondylitis Disease Activity; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index.
Study characteristics. Of the 41 included studies, all offered BASDAI by sex and only 16 of them offered ASDAS by sex.14,15,24,25,31,35,36,42,43,49,50,52,53,56,61,62 The total sample was 19,714 patients, with 6785 women (34.4%) and 12,929 men (65.6%). Nearly all the studies (n = 38, 92.7%) were published in or after 2010, with 26 of them (63.4%) in or after 2015. According to the study design, 31 studies (75.6%) were cross-sectional,14,24,27–29,31–38,40,41,44–49,53–62 9 studies (22.0%) were cohort studies,15,25,30,39,42,43,50–52 and 1 was a case-control study.26 Twenty-five studies (61.0%) included patients with AS,15,25,26,30–33,36–38,41–43,45–47,49,51,53,54,57,58,60–62 11 studies (26.8%) included axSpA,14,24,27,28,35,39,44,50,52,56,59 and 5 studies (12.2%) included SpA.29,34,40,48,55 No study targeted reactive arthritis or enteropathic arthritis alone. All participants fulfilled SpA classification criteria, excluding 2 studies32,40 that used general disease classification plus rheumatologic assessment, and 2 studies that did not identify their criteria.28,44 Regarding the patients source, 21 studies (51.2%) included primary data or records from rheumatology departments,24–27,29,31,33,35,36,38,39,41,45,47,49,50,54,55,58,59,60 8 studies (26.7%) included rheumatology patients from prospective cohorts,14,15,42,43,51,52,56,62 6 studies included rheumatology patients from registries,30,32,34,40,48,53 4 studies included patients from associations,28,37,44,57 1 study included patients from the Bulgarian population,46 and 1 cross-sectional study pooled 4 randomized controlled trials (RCTs).61 The studies involved participants from 36 different countries, and most studies (80.5%) included European patients, at least partially. The characteristics of the 41 studies are shown in Table 1.
Characteristics of the included studies with disease activity according to sex for SpA.
Quality assessment. Out of a maximum of 9 on the NOS, 11 studies were rated as 5,41,44,46,48,49,51,54,55,57,58,60 10 studies as 6,15,25,28,29,32,34,45,47,52,61 8 studies as 7,14,24,26,30,36,38,40,50 and 12 studies as 827,31,33,35,37,39,42,43,53,56,59,62 (Supplementary Table 2, available with the online version of this article). In the selection section, all studies met at least half the items on the NOS, with the loss of initially eligible subjects being the main concern. In the comparison section, 15 studies did not consider any potential confounder other than sex.15,25,29,34,36,41,45,47–49,51,54,55,57,58 In the outcome/response section, missing data were considered as possible in 8 studies.14,30,32,34,48,52,56,62
Descriptive analysis. Female patients with SpA showed a higher BASDAI than male patients (mean 4.9 vs 4.2, P = 0.02). However, ASDAS showed no differences between women and men (mean 2.8 women vs 2.8 men). Men were more frequently HLA-B27–positive than women (71.7% women vs 80.7% men, P = 0.02). No sex-related differences were identified for physical function measured with BASFI, current age, age at onset of disease, disease duration, diagnosis delay, or BMI. Peripheral arthritis and enthesitis were slightly more frequent in women than in men, although no significant differences were detected. In contrast, CRP level and anti-TNF agents were higher in men than in women (Table 2).
Comparison between women and men with spondyloarthritis according to the demographic data and clinical characteristics.
BASDAI metaanalysis of the 41 included studies. The BASDAI metaanalysis showed significant mean differences between males and females in the random-effects model (0.55 [95% CI 0.46–0.65], P < 0.00001). Women had higher BASDAI than men (Figure 3), which was similar to the findings in the fixed-effect model (0.53 [95% CI 0.47–0.60], P < 0.00001). Twenty-four14,15,27–30,32–38,40,44,48,52,53,55,56,59–62 of the 41 studies showed higher disease activity in women than men, and 17 studies24–26,31,39,41–43,45–47,49–51,54,57,58 did not detect sex-related differences. The Q test identified heterogeneity (P = 0.002), which was quantified as moderate (I2 = 44%) according to Deeks, et al.23 Regarding publication bias, the funnel plot (Figure 4) did not suggest any asymmetries, in accordance with the Egger test that did not detect publication bias (P = 0.17). Assessing the robustness of the overall result by excluding individual studies, the sensitivity analysis estimated that the pooled mean difference by sex ranged from 0.53 (95% CI 0.44–0.62) to 0.57 (95% CI 0.48–0.66). Further, the sensitivity analysis by SpA type estimated that the mean difference was 0.63 (95% CI 0.51–0.75) when excluding AS studies, 0.54 (95% CI 0.43–0.66) when excluding axSpA studies, and 0.52 (95% CI 0.42–0.62) when excluding SpA studies. The findings were therefore consistent (Supplementary Table 3, available with the online version of this article).

Forest plots showing comparison by sex of the disease activity in SpA. Mean difference metaanalyses comparing disease activity in women and men with SpA for BASDAI (41 studies) and ASDAS (16 studies). ASDAS: Ankylosing Spondylitis Disease Activity; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; SpA: spondyloarthritis.

Funnel plots. Graphic evaluation of publication bias for BASDAI and ASDAS. ASDAS: Ankylosing Spondylitis Disease Activity; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; MD: mean difference (X-axis); SE (MD): standard error of the mean difference (Y-axis).
ASDAS metaanalysis of the 16 studies included this score. The total sample of the ASDAS metaanalysis was 6449 patients, with 2046 women (31.7%) and 4403 men (68.3%). Ten studies15,25,31,36,42,43,49,53,61,62 included patients with AS and 6 studies14,24,35,50,52,56 included patients with axSpA. The ASDAS metaanalysis did not detect significant differences in means by sex in the random-effects model (0.04 [95% CI –0.05 to 0.12], P = 0.38; Figure 3), which is similar to the findings in the fixed-effect model (0.02 [95% CI –0.03 to 0.07], P = 0.54). Thirteen14,24,31,35,36,42,43,49,52,53,56,61,62 of the 16 studies did not detect differences by sex in disease activity, 2 studies15,25 showed higher disease activity in women than men, and 1 study50, by contrast, showed lower disease activity in women than men. The Q test identified heterogeneity (P = 0.007), that was quantified as substantial (I2 = 3%) according to Deeks, et al.23 Regarding publication bias, the funnel plot (Figure 4) did not suggest any asymmetries, in accordance with the Egger test that did not detect publication bias (P = 0.43). By excluding individual studies, the sensitivity analysis estimated that the pooled mean difference by sex ranged from 0.02 (95% CI –0.06 to 0.10) to 0.06 (95% CI –0.02 to 0.13); additionally, no variations were detected by excluding AS studies (0.4 [95% CI –0.12 to 0.19]) and axSpA studies (0.4 [95% CI –0.07 to 0.14]). Therefore, the findings were consistent (Supplementary Table 4, available with the online version of this article).
BASDAI metaanalysis of the 16 studies that included information on both scores. This metaanalysis identified a mean sex difference for the random-effects model of 0.57 (95% CI 0.44–0.69; P < 0.00001), which was similar to the fixed-effect model (0.55 [95% CI 0.45–0.65], P < 0.00001; Supplementary Figure 1, available with the online version of this article). Nine14,15,35,36,52,53,56,61,62 of the 16 studies studies showed higher disease activity in women than men, whereas 7 studies24,25,31,42,43,49,50 did not detect sex differences in disease activity. No publication bias was detected using the Egger test (P = 0.40) and no significant heterogeneity was identified (P = 0.20, I2 = 23%), so it was not necessary to perform a sensitivity analysis.
DISCUSSION
The results of our systematic review of 41 studies showed that SpA activity registered through BASDAI was higher in women than in men. This is in line with the metaanalysis, in which women presented higher disease activity than men. Conversely, we did not find statistical differences between sexes in the 16 ASDAS studies, consistent with the ASDAS metaanalysis that did not detect differences in means by sex. This finding was further supported by the comparison of disease activity by sex in the 16 studies that included information from both indices. The BASDAI metaanalysis of these 16 studies supports the idea that BASDAI and ASDAS measure disease activity differently.
ASDAS has shown discriminatory ability in patients with peripheral SpA included in 2 RCTs.9 Clearly, part of the ASDAS construct is capable of measuring disease activity, but not adequately for peripheral patients. If we assume that the disease is a continuum that goes from axial patients to peripheral patients, the construct will always measure the axial part (existing in most patients with SpA). Therefore, if peripheral activity is not detected, patients are at risk of not receiving the correct medication.
Both scores were developed to measure disease activity in patients with AS and have been used in RCTs of AS and axSpA, which include early nonradiographic forms of AS. This selection bias may have a notable effect on the detection of disease activity for peripheral SpA, which has a higher prevalence in women than men.
Neither the items in both scores nor their weights are the same. The element of back pain has a similar weight in ASDAS (17.3%) and BASDAI (20%; Figure 1). However, ASDAS contains a question about peripheral manifestations (tender and swollen joints), with the score having a lower weight (10.4%) than in BASDAI (20%). Further, enthesitis, which is more frequent and more severe in women than in men,25,45,48,50,57 is not included in ASDAS, whereas a question intended to capture enthesitis is included in BASDAI with a weight of 20%. Enthesitis, together with fatigue, are 2 controversial items in quantifying SpA activity. Questions about enthesitis are considered vague and difficult to answer for many patients who do not fully understand the related symptoms. It appears that omitting this question increases the validity of the measurement of SpA disease activity. In addition, pain similar to that in enthesitis can be seen in patients with fibromyalgia (FM), overweight patients, and people who play sports.63
In patients with concomitant FM, this question can also be scored in the high range, which increases (inaccurately) the overall BASDAI score.64 We know that FM is more frequent in women than men; therefore, there is an uncertainty regarding whether a higher BASDAI score in women could be due to peripheral manifestations of SpA or to a different cause.65
Fatigue is a relevant manifestation in SpA, but it is often a nonspecific variable that shares symptoms with other conditions, including various psychological disorders and sleep disturbance.66 It is also usually higher in women than in men,45,55 probably leading to sex differences in the measurement of disease activity in BASDAI. These differences may be less marked in ASDAS since the patient global assessment of disease activity was considered in this score instead of fatigue.
Another plausible explanation for the sex-related differences detected in the measurement of SpA activity between BASDAI and ASDAS might be the fact that CRP is included in ASDAS. In men, the higher CRP value may balance the lower value of the subjective ASDAS items, since male patients have higher mean baseline CRP than female patients in AS.62 However, CRP increased in only 35–50% of patients with AS,67 so the weight of CRP should not be as determining in the ASDAS estimation. In a large cohort of patients looking for sex differences in axial and peripheral SpA, males had elevated CRP more frequently than females in the axial group and no significant differences were detected between sexes in the peripheral group.68
In our study, men were more frequently HLA-B27–positive than women. However, there is no association between being HLA-B27–positive and higher disease activity, as demonstrated by Arévalo, et al, who found that HLA-B27–negative patients with AS showed significantly higher BASDAI scores than HLA-B27–positive ones.69 Regarding BMI, both women and men were slightly overweight. However, in truly obese patients, BASDAI may be influenced by BMI, as Ortolan, et al have discussed.70
Our study has several strengths. First, efforts were made to address the problem of missing data and to include as many studies as possible. In addition, we used predefined protocols for the extraction and evaluation processes. All these steps increase confidence in our findings. Finally, the quality of the studies according to the NOS was in the upper limit, from almost 5 up to 9. However, this study also has several limitations. First, the studies presented differences in their designs, data sources, sample sizes, and clinical types of SpA. Despite this heterogeneity, the results of both metaanalyses were consistent according to the sensitivity analysis. Further, we did not consider grey literature, but we conducted a prospective search of published studies from the identification of relevant meeting abstracts. Another limitation could be that the review covered publications only in English and Spanish; however, we did not identify a publication bias using both funnel plots and the Egger test. In addition, despite including patients starting anti-TNF therapy who may have a more severe disease state and higher disease activity,15,25,42,43,50,51,61 our sensitivity analysis ruled out that the inclusion of these studies modified the overall effect for both BASDAI and ASDAS. All studies in the ASDAS metaanalysis included axial patients,14,15,24,25,31,35,36,42,43,49,50,52,53,56,61,62 as did 90.2% of the studies included in the BASDAI metaanalysis.14,15,24–28,30–33,35–39,41–54,56–62 This could offer a partial viewpoint; yet, if our results had been biased due to the lack of representation of peripheral patients, it would be expected that BASDAI would have detected greater differences between the sexes and ASDAS would continue without detecting differences by sex, due to an overestimation of items such as fatigue and a lack of sensitivity regarding peripheral features, respectively.
We were unable to perform a subgroup analysis by sex specifically for predominantly axial and predominantly nonaxial patients due to the lack of information in most of the studies reviewed. No efficacy endpoint has been specifically developed and validated for a patient population with predominant pauciarticular joint and enthesis involvement.9 Interestingly, deleting data from patients with AS in the sensitivity analysis increased the sex differences in BASDAI; conversely, no sex differences were found in ASDAS across all SpA types, supporting the idea that the different measure between indices is related to how each SpA type, and its manifestations, is represented within each index (Figure 1).
Gender bias has been evidenced by the diagnostic delay and misdiagnosis of SpA.71,72 The higher diagnostic delay and misdiagnosis in women than in men with SpA could be due to methodological reasons, when the disease model is based on the male prototype and female presentations are not recognized. The results of this review cast a reasonable doubt on the existence of another gender bias in SpA that occurs when a score, developed mainly using men who are sensitive to axial presentations, is extrapolated to other nonaxial presentations more frequent in women. In future research, it would be desirable to develop a new score to measure disease activity in patients with nonaxial SpA. Such a score should be sensitive to both women and men with a predominance of peripheral manifestations in order to identify the included variables, together with their weights, resulting in a more well-rounded index to estimate peripheral presentations.
To conclude, our metaanalyses provide robust evidence of the differences between BASDAI and ASDAS in measuring disease activity by sex. Women had higher disease activity compared to men using BASDAI, but these differences disappeared when using ASDAS. The different components and weights in BASDAI and ASDAS influence their values. Based on the already known sex differences in the presentation of SpA, BASDAI may be affected by fatigue, but in predominantly peripheral manifestations such as enthesitis, ASDAS may not be sensitive enough to detect activity. This may represent a sex bias unfavorable to women, because peripheral SpA is more common in women than in men.
ACKNOWLEDGMENT
We thank Dr. Theodore Pincus for helping us plan this study. We also thank Dr. Eduardo Collantes Estévez, Dr. Rafaela Ortega Castro, and Dr. Pilar Font Ugalde on behalf of the REGISPONSER Working Group, and Dr. Adrian Ciurea on behalf of the Swiss Clinical Quality Management for kindly providing us with additional data.
Footnotes
\MBB has received 2 scholarships from the Instituto Universitario de Investigación en Estudios de Género (Universidad de Alicante, Spain) and the Facultad de Ciencias de la Salud (Universidad de Alicante, Spain) to support this study as her doctoral training. No commercial support has been received to carry out this study.
The authors declare no conflicts of interest relevant to this article.
- Accepted for publication March 16, 2021.
- © 2021 by the Journal of Rheumatology
REFERENCES
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.








{kind=link}
{kind=link}
{kind=link}
{kind=link}