

Abstract
Objective. To identify shared and distinct features of giant cell arteritis (GCA) and coronavirus disease 2019
(COVID-19) to reduce diagnostic errors that could cause delays in correct treatment.
Methods. Two systematic literature reviews determined the frequency of clinical features of GCA and COVID-19 in published reports. Frequencies in each disease were summarized using medians and ranges.
Results. Headache was common in GCA but was also observed in COVID-19 (GCA 66%, COVID-19 10%). Jaw claudication or visual loss (43% and 26% in GCA, respectively) generally were not reported in COVID-19. Both diseases featured fatigue (GCA 38%, COVID-19 43%) and elevated inflammatory markers (C-reactive protein [CRP] elevated in 100% of GCA, 66% of COVID-19), but platelet count was elevated in 47% of GCA but only 4% of COVID-19 cases. Cough and fever were commonly reported in COVID-19 and less frequently in GCA (cough, 63% for COVID-19 vs 12% for GCA; fever, 83% for COVID-19 vs 27% for GCA). Gastrointestinal upset was occasionally reported in COVID-19 (8%), rarely in GCA (4%). Lymphopenia was more common in COVID-19 than GCA (53% in COVID-19, 2% in GCA). Alteration of smell and taste have been described in GCA but their frequency is unclear.
Conclusion. Overlapping features of GCA and COVID-19 include headache, fever, elevated CRP and cough. Jaw claudication, visual loss, platelet count and lymphocyte count may be more discriminatory. Physicians should be aware of the possibility of diagnostic confusion. We have designed a simple checklist to aid evidence-based evaluation of patients with suspected GCA.
Giant cell arteritis (GCA) is the most common form of systemic vasculitis and typically affects patients over the age of 50. GCA is still little known among the general public and the diagnosis is usually first suspected by a physician, most frequently in evaluating new-onset headaches. Laboratory tests typically show an acute-phase response and rheumatologists play a key role in diagnostic confirmation. This is one of the most time-critical decisions in rheumatology: Failure to treat may result in blindness, but misdiagnosis of GCA can lead to inappropriate immunosuppression and a missed opportunity to treat the real underlying cause of the symptoms. The coronavirus disease 2019 (COVID-19) pandemic has presented new challenges in the evaluation of patients with suspected GCA, including the need to direct patients by either “hot” or “cold” pathways to minimize inadvertent transmission of SARS-CoV-2.
During much of the current pandemic, the incidence of COVID-19 in the community has been higher than that of GCA in many places. Early public health messages emphasized fever, cough, and shortness of breath as COVID-19 indicators, with alteration in taste/smell having been subsequently added. Anecdotally, we saw patients referred for evaluation of GCA who turned out to have COVID-19–related headaches while, conversely, patients with persistent fever who were initially thought to have COVID-19 were only suspected to have GCA after prolonged investigations for infection. Guidelines advise specialist evaluation of suspected GCA within 24 hours and confirmation of the diagnosis by vascular ultrasound or temporal artery biopsy (TAB), but during the COVID-19 pandemic, the close, sustained personal contact with a healthcare practitioner during either of these procedures carries potential risk for both individuals. There is now an imperative for physicians to differentiate between GCA symptoms and COVID-19 symptoms and to conduct a risk assessment before the ultrasound scan takes place. We reviewed the literature to gather the best available evidence on features that may discriminate between the 2 conditions.
METHODS
We performed 2 systematic literature reviews. Searches were carried out by 2 independent reviewers and discrepancies were resolved by wider consensus.
For the GCA literature review, a general search strategy for the diagnostic features of GCA had already been devised for a previous systematic review and metaanalysis (Supplementary Methods, available with the online version of this article) and was updated on April 5, 2020. We searched PubMed, Embase, and the Cochrane Database of Systematic Reviews to identify studies recruiting consecutive patients with suspected GCA. The preferred reference standard was TAB or vascular imaging, but studies using a reference standard of clinical diagnosis were included if ≥ 75% of the patients clinically diagnosed with GCA had positive TAB or vascular imaging to confirm this diagnosis. For this review, we selected the 4 largest studies that reported the frequency of each symptom. However, for less typical GCA features and laboratory tests with limited data available, we also performed a directed search in PubMed to obtain data from other study types reporting these features in patients with GCA.
For the COVID-19 review, we identified all cohorts or case series published between January 1, 2020, and April 5th, 2020, that described patients diagnosed with COVID-19. We excluded retrospective case series of < 50 patients, and reports in which the patients had all died, were all in the intensive care unit, or had a particular comorbidity (e.g., cancer). PubMed, Embase, and the Cochrane Database of Systematic Reviews were all searched. References from included studies as well as the NCBI database LitCovid (www.ncbi.nlm.nih.gov/research/coronavirus) were searched to identify other potentially eligible studies. We did not review the frequency of hypoxemia and tachypnea since, in the context of our review, these symptoms would have been likely to prompt further investigation and treatment for respiratory pathology.
For each selected publication, we extracted the reported frequencies of each symptom, sign, or laboratory feature, and determined the median and range for the publications reviewed. Comparing the 2 diseases, we divided the features into those more typical of GCA, those more typical of COVID-19, and those observed in both. Risk of bias assessment was performed independently by 2 authors using the Institute for Health Economics quality appraisal checklist for case series studies (IHE, Edmonton, Alberta, 2014: www.ihe.ca/research-programs/rmd/cssqac/cssqac-about), which can be found in the Supplementary Material (available with the online version of this article). Any differences were adjudicated by a third author.
RESULTS
A general search strategy for diagnostic features of GCA and additional directed searches yielded 1666 unique hits (Supplementary Methods, available with the online version of this article). Of these, 35 studies were included for analysis, of which 30 studies were selected from the general search strategy and the remaining 5 studies had been identified by the additional directed searches. Limited or no published data on the frequency of lymphopenia or thrombocytopenia in GCA were found; therefore, 2 coauthors reanalyzed raw data from a previously published study1.
From the COVID literature review, 211 studies were identified. After screening the title and abstract of each paper, 33 full texts were selected for review. Of these, 29 studies comprising 5623 patients were included in this analysis. One additional study2, published after the updated search was concluded, was identified and included to provide information on the frequency of altered sense of smell or taste that had not been identified through the general search strategy. This study also included data regarding vision impairment.
The main findings are presented in Table 1 and summarized in Figure 1. The overall risk of bias in the included studies1–67 was moderate; details can be found in the Supplementary Material (available with the online version of this article). The main issue identified in the COVID-19 studies was that these studies were almost all restricted to hospitalized patients who were at various stages of disease. Since the most common reason for hospitalization is respiratory symptoms, these may have been overrepresented in the literature, and nonrespiratory symptoms underrepresented, compared to patients with COVID-19 presenting from the community. With regard to the GCA studies, the majority of studies were retrospective and involved collection of data from medical records, sometimes over many decades. In addition, the stated aim of many of the GCA studies was not to describe the features of the disease, but instead focused on a particular research question. The description of GCA features appeared to be largely intended to show that the “core” GCA features were similar to those in previously published studies. The frequency of headache was always reported in the GCA studies, for example, but the frequency of cough was rarely reported. In the COVID-19 studies, the frequency of cough was reported in 26/29 studies and headache in 17/29 studies, but some symptoms, such as myalgia/arthralgia, were less precisely defined than in the rheumatology literature.
Frequency of symptoms, physical signs, and laboratory abnormalities in GCA and COVID-19.

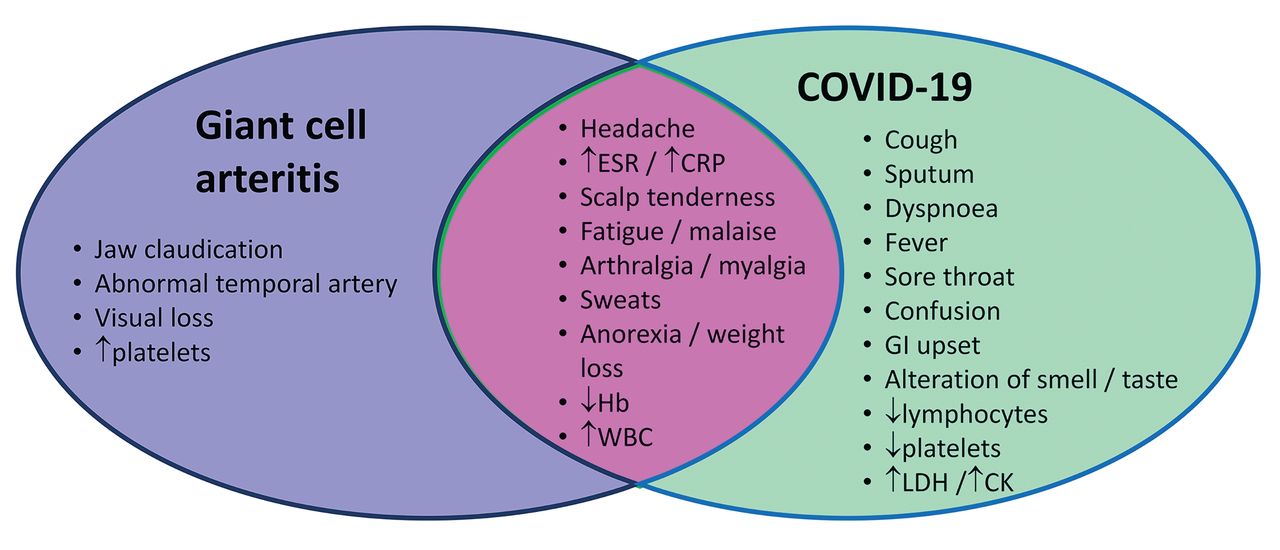
Features of giant cell arteritis and COVID-19 based on reported frequencies. This Venn diagram represents features that are more commonly reported in GCA or COVID-19, and features that may be seen in both conditions (overlapping section). Headache and elevated inflammatory markers (in the dotted box), often considered the cardinal features of GCA, may be observed in both GCA and COVID-19. CK: creatine kinase; COVID-19: coronavirus disease 2019; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; GCA: giant cell arteritis; GI: gastrointestinal (diarrhea or vomiting); Hb: hemoglobin; LDH: lactate dehydrogenase; WBC: white blood cell count.
DISCUSSION
In the > 50 age group, GCA and COVID-19 may initially present with similar symptoms. As reported in a recent systematic review and metaanalysis68, only around 2 of 3 patients with GCA report headache, while around 1 of 4 report fever. In the COVID-19 studies we identified, headache is reportedly present in 2–34% and fever in 83% of patients. Acute-phase response is common in both conditions. Thrombocytosis may point more towards GCA, and lymphopenia towards COVID-19.
The possibility of reporting bias is important when interpreting these data: in large, single-disease cohorts, structured data collection tends to focus on features considered typical of the disease in question. Historically, dry cough has been underrecognized as a symptom of GCA, and it was reported in only a minority of studies we identified11,32,59,60,61,65,67. Patients presenting with new-onset GCA should be evaluated for cough, since this might be associated with involvement of the aorta and its proximal branches, which is a potential risk factor for relapse or aortic aneurysm in GCA; however, this hypothesis requires testing.
We were limited by not being able to stratify GCA by symptom duration. The average reported symptom duration in GCA is 9 weeks, but this is highly variable. On average, symptom duration is somewhat longer in nonheadache presentations, and shorter in those with isolated cranial symptoms69. The average duration of COVID-19 symptom onset to admission was typically 1–2 weeks in these studies20,22,37,58, but this may differ outside of China.
Most of the COVID-19 data in our review came from hospitalized cases in China. According to the World Health Organization–China Joint Mission report, published February 28, 2020, even mild COVID-19 cases were compulsorily removed to either Fangcang shelter hospitals or acute hospitals designated for COVID-19. Patients > 65 or with a comorbidity such as hypertension were not eligible for care in Fangcang hospitals and instead were admitted to acute hospitals. The average age of patients in the studies we identified was 53.6 years. At that time, anosmia was not universally recognized as a COVID-19 symptom and so it appears in few publications from this period. This illustrates that it cannot be assumed a symptom not reported in a disease is always absent. We surmise, however, that it is likely that the most prominent features of any disease will be the ones reported; therefore, our findings are likely to remain clinically relevant. For features less typical of GCA, if larger studies did not report the frequency of these features, a compromise was reached by including additional small studies, one of which also included polymyalgia rheumatica66.
Our review raises new research questions that are testable by prospectively collecting data during the current pandemic. First, in patients presenting with headache due to COVID-19, what is the frequency of “GCA-like” features, such as scalp tenderness, temporal artery tenderness, difficulty chewing, transient visual loss, weight loss, dysphagia, or trismus in patients? Second, in patients presenting with GCA, what is the frequency of “COVID-19–like” features such as dry cough, sore throat, dyspnea, confusion, anosmia or alteration in sense of taste2,70, lymphopenia, thrombocytopenia, elevation in lactate dehydrogenase, or elevation in creatine kinase? Third, given that most of the data on COVID-19 symptom patterns identified in this review come from China, is there variation in the clinical presentation of COVID-19 according to ethnicity or culture? Fourth, how does the clinical picture of GCA patients presenting with a short symptom duration (days–weeks) differ from those presenting with a long symptom duration (months–years)? Last, is cough at presentation of GCA associated with an increased relapse risk?
It has always been true that most new-onset headaches will not be due to GCA, and many will be due to minor viral infections; however, the novel situation at the time of writing is that currently, many new-onset headaches may be due to COVID-19. Based on the evidence we identified in our literature search, we have designed a simple clinical checklist (Figure 2) that could aid clinicians in assessing patients with suspected GCA during the COVID-19 pandemic, as well as in generating data that might answer some of the research questions identified here.
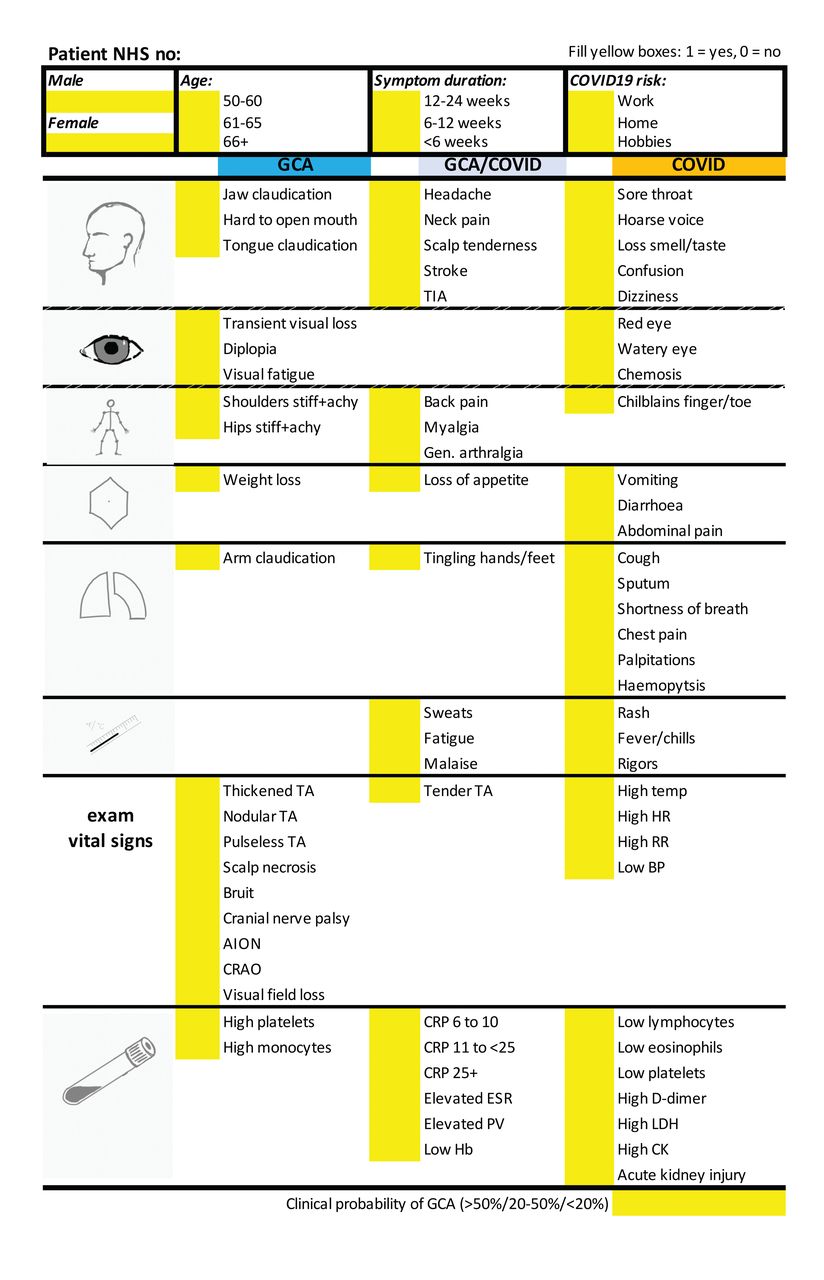
A checklist to support evidence-based history and examination in evaluation of patients with suspected giant cell arteritis. This checklist was constructed in an Excel spreadsheet, informed by the findings of the literature review presented here. The checklist is primarily intended to aid clinicians who are conducting a telephone consultation with a patient referred with suspected giant cell arteritis, prior to their face-to-face appointment during the COVID-19 pandemic. There is also space for relevant physical examination findings and laboratory test results to be added, if provided by the referrer. This checklist has been piloted in Leeds, UK, where it has been further customized to allow the automated generation of relevant alerts (by conditional formatting) and risk scores (based on local audit data and the published literature) to support clinical decision making. AION: anterior ischemic optic neuropathy; BP: blood pressure; CRAO: central retinal artery occlusion; CK: creatine kinase; COVID19: coronavirus disease 2019; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; GCA: giant cell arteritis; Gen: general; Hb: hemoglobin; HR: heart rate; LDH: lactate dehydrogenase; NHS: National Health Service (UK); PV: plasma viscosity; RR: respiration rate; TA: Takayasu arteritis; TIA: transient ischemic attack.
Footnotes
PM is a clinical training fellow within the Medical Research Council— GlaxoSmithKline (MRC-GSK) Experimental Medicine Initiative to Explore New Therapies network and receives project funding unrelated to this work. PM also receives cofunding from the National Institute for Health Research (NIHR) University College London Hospitals Biomedical Research Centre. MP is supported in part by Grant Number T32 AR007611-13 from the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). SES received funding from the Vasculitis Clinical Research Consortium (VCRC)/Vasculitis Foundation Fellowship. The VCRC is part of the Rare Diseases Clinical Research Network, an initiative of the Office of Rare Diseases Research, National Center for Advancing Translational Science (NCATS). The VCRC is funded through collaboration between NCATS, and NIAMS (U54 AR057319). SLM receives infrastructure support from the MRC TARGET Partnership Grant (MR/N011775/1/MRC_/Medical Research Council/United Kingdom) and from the NIHR Leeds Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
P. Mehta, S.E. Sattui, and K. van der Geest made equal contributions to this work.
KSMvdG received a speaker fee from Roche (2019) paid to the UMCG. EB received consultancy and speaker fees from Roche (2017 and 2018) paid to the UMCG. PR reports no competing interests related to this work, outside of this work he reports personal consulting and/or speaking fees from AbbVie, Eli Lilly, Janssen, Novartis, Pfizer and UCB and travel assistance from Roche. SLM received consultancy fees from Roche (2015) and was supported by Roche to attend EULAR 2019. She has acted as investigator on clinical trials in GCA for Sanofi, Roche and GSK. Consultancy fees from Roche (2016, 2018) and Sanofi (2017) were paid to her institution. She is Patron of the UK charity Polymyalgia Rheumatica & Giant Cell Arteritis UK. RC, PM, MSP, SES have no conflicts of interest declared.
Full Release Article. For details see Reprints and Permissions at jrheum.org.
- Accepted for publication September 29, 2020.
- Copyright © 2021 by the Journal of Rheumatology
Free online via JRheum Full Release option








{kind=link}
{kind=link}