

Abstract
Objective. Axial spondyloarthritis (axSpA) may have an effect on work. The Ankylosing Spondylitis Work Instability Scale (AS-WIS) assesses difficulties at work. The objective of this study was to evaluate the predictive value of the AS-WIS on work impact.
Methods. This is a prospective cohort study with 2 timepoints (at baseline and after 1.5 yrs) that included patients with axSpA who had paid employment. Patients completed the AS-WIS at baseline and work instability was scored as moderate/high if ≥ 11 (0–20 scale). At follow-up, adverse work outcomes (AWO) were grouped as moderate (short-term sick leave) or severe AWO (long-term sick leave, disability, unemployment). Univariable and multivariable logistic regression analyses were performed to explain AWO.
Results. Of 101 patients, mean age 45 (SD 9) years, 52% male, disease duration was 14 (SD 8) years. The Bath AS Disease Activity Index and the Bath AS Functional Index were 34 (SD 21) and 23 (SD 23), respectively, and 69 (68%) received a tumor necrosis factor inhibitor. At baseline, 46 (46%) patients had moderate/high AS-WIS. At 1.5 years of follow-up, 37 patients (36%) had AWO: 25 patients (25%) a short-term sick leave, and 12 patients (12%, 7/100 patient-years) a severe AWO. Independent baseline factors associated with AWO were a moderate/high AS-WIS score (OR 2.71, 95% CI 1.04–7.22) and shorter disease duration (OR 0.94, 95% CI 0.89–0.99).
Conclusion. In patients with axSpA, a moderate/high AS-WIS score was predictive of AWO in this population with well-controlled axSpA. This short questionnaire can be helpful to screen for future difficulties at work.
Axial spondyloarthritis (axSpA) affects subjects of working age and has an important effect on patients’ ability to work. Studies have shown that work impact for patients with SpA ranges from 22% to 31%1,2,3 depending on the definition used for work disability, from reduced working hours, to short-term or long-term sick leave, to loss of work and unemployment. The risk of unemployment was 5% in the first year, and 31% at 20 years of disease.3 Loss of employment is associated with socioeconomic factors, comorbidities, disease status (disease duration, greater physical impairment, and pain) and psychological distress (anxiety, depression).4,5
Understanding the importance of the disease’s effect on the patient’s working capacity may be useful in order to develop preventive measures and adaptation of the work conditions. An objective tool to evaluate difficulties at work is the Ankylosing Spondylitis Work Instability Scale (AS-WIS), a 20-item questionnaire developed in 2009, which identifies patients thought to be at low (< 11 points), moderate (11–18 points), or high (> 18 points) risk of work instability.6 The initial study included 57 patients, of whom 40% had moderate to high levels of work instability.6 Other authors have confirmed the feasibility of the AS-WIS.7
However, to date no study has assessed the predictive value of the AS-WIS. This has been assessed in rheumatoid arthritis (RA), using the Rheumatoid Arthritis Work Instability Scale (RA-WIS),8 which was found useful to predict adverse work outcomes (AWO) at 1 year of follow-up.9
Thus, the main objective of this study was to evaluate the predictive value of the AS-WIS on work impact in axSpA.
METHODS
Participants and study design. This was a prospective cohort study with 2 timepoints (at baseline and after 1.5 years) in 3 centers in Paris, France. The baseline data regarding other aspects of this study have been previously published.7,10,11,12 All patients with axSpA according to the rheumatologist and the Assessment of SpondyloArthritis international Society classification criteria13 seen in a hospital or outpatient clinic, between September 2013 and February 2014, were sent a questionnaire by mail. The baseline questionnaire was sent to 240 patients.
For patients who had answered the baseline questionnaire and were currently in a paid work position, a second questionnaire was sent after 1 year, with 2 subsequent reminders if needed at 6 and 12 months.
Work instability. The AS-WIS questionnaire was used to assess the effect of the disease on work capacity. The AS-WIS had been previously translated, cross-culturally adapted, and validated in French.8 It is a 20-item simple screening tool for work instability (the consequences of a mismatch between an individual’s functional ability and their work tasks).8 The AS-WIS is scored between 0 and 20, with higher numbers indicating higher instability. In the present study, it was scored as proposed by the scale’s authors: low if the score was < 11, moderate if between 11–18, and high if > 18.6
AWO. At follow-up, 4 different events were defined as AWO: short-term sick leave (< 3 months), long-term sick leave (between 3 months and 2 yrs), work disability (state-accepted status of incapacity to work), and unemployment (loss of employment). They were grouped into moderate AWO (short-term sick leave) and severe AWO (long-term sick leave, disability, and unemployment).
Data collection at baseline. Demographic characteristics including age, sex, BMI, education level, and work status (employed, unemployed, or unable to work) were collected. Also, the patients were asked to answer the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)14 and Bath Ankylosing Spondylitis Functional Index (BASFI).15 The medical files were accessed to obtain data on the presence of HLA-B27, radiographic sacroiliitis, and presence of high C-reactive protein.
Statistical analysis. Statistical analysis included descriptive analyses of AWO, AWO per 100 patient-years (PY), and AS-WIS scores. Variables in the univariable analysis included demographic data, type of work, level of studies, and disease-related variables (BASDAI, BASFI, current tumor necrosis factor inhibitor (TNFi) treatment, radiographic sacroiliitis, and HLA-B27). Variables with a P value < 0.10 in univariable analysis were further tested in multivariable analysis, without any other selection criteria. An exploratory analysis of predictors of severe AWO was also run. There was no imputation of missing data.
Ethics and consent. This study was approved by the Pitie-Salpetriere Ethics Committee (2014_04) and patients signed written informed consent.
RESULTS
Patient population. Among the 209 patients who answered the first questionnaire, 144 were currently working and 101 (70% of 144) answered the second questionnaire. Among patients not working, most were retired (12%) or in work disability/long-term sick leave (9%). The 43 patients who did not answer the second questionnaire had similar demographic characteristics to the responders (data not shown). Mean age at inclusion was 45 (SD 9) years, 52 (52%) were male, disease duration was 14 (SD 8) years, and 62 (62%) had an education level equivalent to more than high school. More patients had white-collar jobs (n = 59, 58% of available data) than blue-collar jobs (n = 26, 25%). The BASDAI and the BASFI were 34 (SD 21) and 23 (SD 23), respectively. At baseline, 69 (68%) received TNFi treatment (Table 1).
Characteristics of 101 axSpA patients with paid employment.
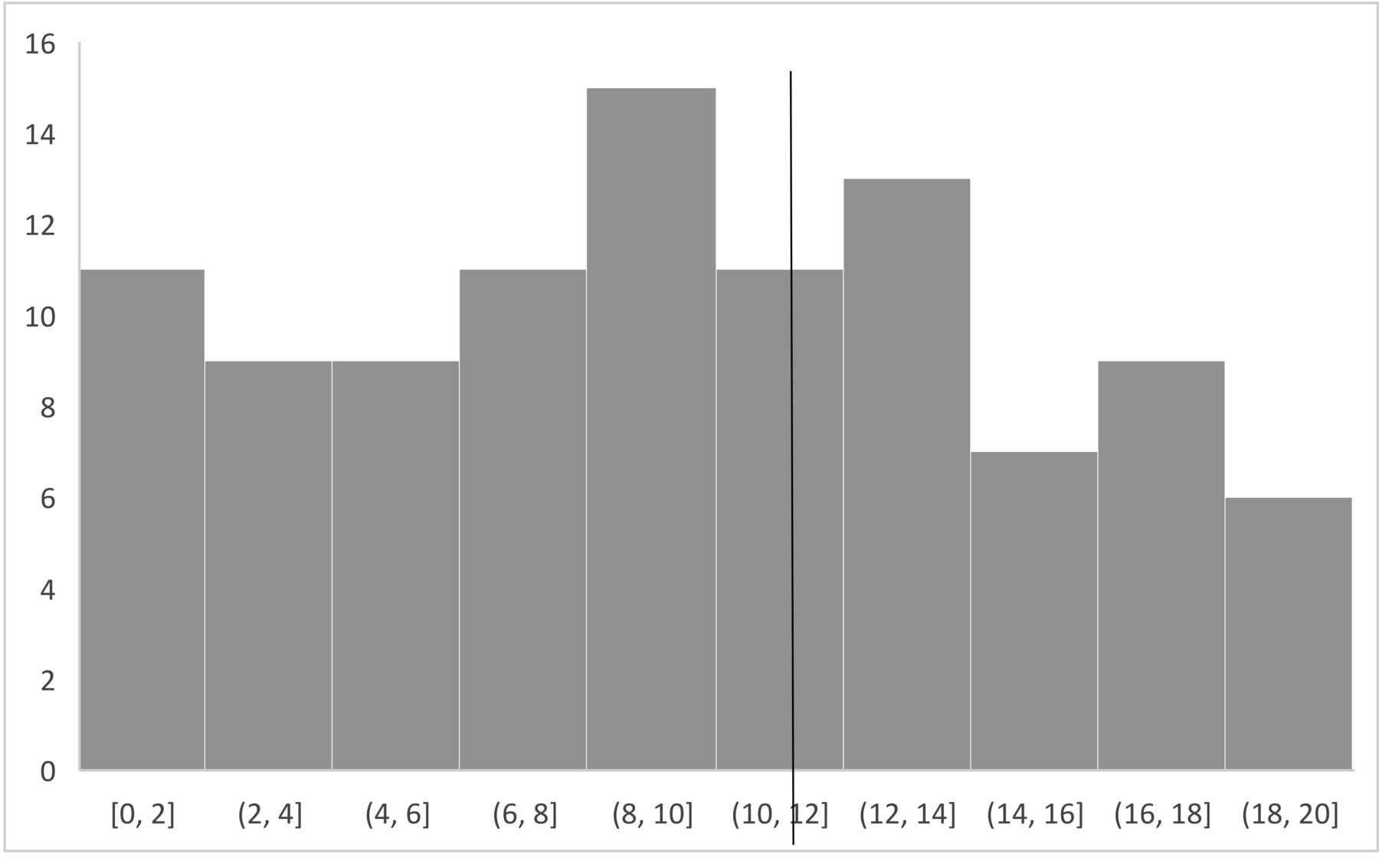
AS-WIS at baseline. The mean AS-WIS (0–20 scale) was 9 (SD 5) with a median of 10, a low-risk score was found in 55 patients (54%), and a moderate/high-risk score in 46 (46%; Figure 1). The questions that were most often scored as present in the AS-WIS referred to the relationship between pain and the patients’ ability to concentrate on tasks (question 4, 79% positive answers) and to variability across days (bad days/good days, question 9, 77%).

AS-WIS score at baseline (in intervals of 2 points). Vertical line indicates cutoff between low (< 11) and moderate/high (≥ 11) AS-WIS scores. AS-WIS: Ankylosing Spondylitis Work Instability Scale.
AWO. The mean (SD) follow-up was 1.5 (0.3) years. At follow-up, 37 patients (36%) had AWO: 25 patients (25%) had moderate AWO and 12 patients (12%) had severe AWO (4 [4%] long-term sick leave, 5 [5%] disability, 3 [3%] unemployment). All patients who reported loss of employment stated that the cause was SpA-related.
Overall, 17 (16%) patients had to adapt their workspace, 6 (6%) had to change their workspace without changing profession, 1 (1%) had to change profession, and 2 patients (2%) switched from full time to half time. Out of 46 patients with moderate/high AS-WIS, 11 (24%) patients had to adapt their workspace, 2 (4%) patients changed workspace, and 1 patient (2%) changed profession. No patient in this group reduced their working hours.
Over the follow-up of 159 PY, the rate of any AWO was 23/100 PY and of severe AWO was 7/100 PY.
Predictors of AWO. In the univariable analysis (Table 2), baseline factors associated with any AWO were a moderate/high AS-WIS score, a high BASFI, and a shorter disease duration. Apart from the BASFI, no other disease-related variables were significant. In multivariable analysis, moderate/high AS-WIS (OR 2.71, 95% CI 1.04–7.22) and lower disease duration (OR 0.94, 95% CI 0.89–0.99) were independent predictive factors of AWO. Of note, a moderate/high AS-WIS score was not predictive of severe AWO, but severe AWOs were rare (n = 12).
Variables associated with AWO after 1.5 years of follow-up.
Among patients with a low AS-WIS score at baseline (n = 55), only 13 (24%) had AWO (including only 2 [3%] with severe AWO). Among patients with a moderate/high AS-WIS score (n = 46), 24 (52%) had AWO (including 10 [22%] patients with severe AWO; Figure 2).
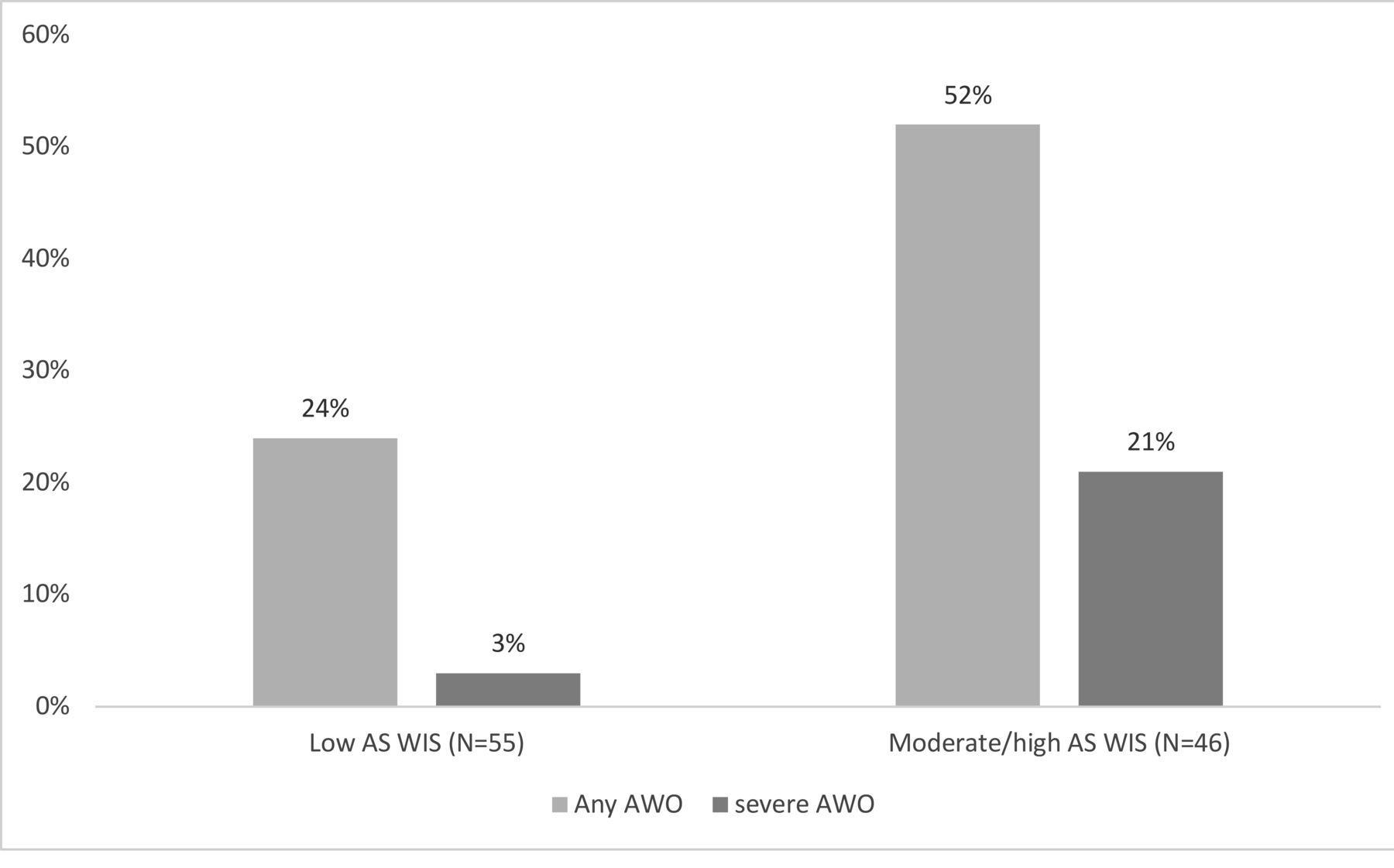
Any AWO vs severe AWO in patients with low and moderate/high AS-WIS score. AS-WIS: Ankylosing Spondylitis Work Instability Scale; AWO: adverse work outcomes.
DISCUSSION
In the present study, we demonstrated the predictive value of the AS-WIS for work impact in axSpA over a follow-up of 1.5 years. We found that the risk of AWO was relatively frequent in this population of stabilized axSpA patients, with 37 (36%) patients with AWO and 12 patients (7/100 PY) with severe AWO. Further, the risk of AWO was almost tripled by a moderate/high work instability risk, as assessed by the AS-WIS. The use of the AS-WIS might allow targeted interventions for maintaining employment status.
This study has a number of limitations. The number of patients is relatively small and the duration of the follow-up moderate.1 However, the study validating the RA-WIS in RA had a similar size and duration of follow-up,9 and our study did not lack power. There was no confirmation of the AWO (by physician or social insurance); we used patient-reported data. However, patient-reported outcomes are usually found to be reliable.16 It is possible that not all variables of interest (such as potential effect modifiers) were taken into account in the analyses. AWO and in particular, loss of work, is of course multifactorial, with elements related to socioeconomic factors on top of disease-related causes. In the present study, we did not collect enough nondisease-related variables to be able to fully assess this point. We chose to pool all AWO in the present study. It can be argued that short-term sick leave is not relevant for work instability, but it was previously shown that prior sick leave predicts future AWO.17,18 Therefore, head-to-head comparisons are difficult to make, since definitions of AWO included in these studies are different (some of the studies do not include short-term sick leave). Also, a time-to-event analysis might have brought additional information. The study dates from 2014, which may be considered a weakness, since the management options in axSpA have evolved.19 However, our study included patients from a tertiary care center, with a high rate of biologics being used. Thus, we believe the present results are relevant.
The high rate of patients experiencing AWO confirms the effect of axSpA on employment status. Previous studies have found a prevalence of AWO of 22% for a follow-up of 12 years,1 a lower rate than in our study. These results are surprising, considering that we included a more recent cohort, with a higher proportion of patients treated by biologic therapy (68% vs 14% in OASIS1). The high number of patients treated by biologics suggests that this is a cohort of patients who may have had very active disease, though activity at the time of study was low and severity was moderate (as indicated by 21% patients with syndesmophytes). The high activity of the disease at some point in time may explain the higher percentage of AWO. There are, of course, differences between countries’ health insurance systems, and it was recently shown that higher country healthcare expenditure is associated with higher likelihood of maintaining employment status.20 Another factor to be considered could be the psychological profile of the patients, which could have changed over recent years due to shifts in expectations.21,22,23,24
When exploring severe AWO, we found that only 12% of our patients (i.e., 7/100 PY) experienced severe work impact, of whom 3 (3%) were unemployed, a much lower finding than what was previously reported in the literature (around 20%).2 This could be due to the fact that our study included only patients with paid work, leading to a skewed distribution in this population. An inception cohort would allow to analyze AWO incidence taking into account disease duration and its evolution; however, to date no such studies are available.25
The main predictors for AWO in our study were moderate/high AS-WIS scores at baseline and shorter disease duration. The latter could be explained by the skewed nature of our population since to be included, patients, by definition, did not have work disability. Thus, patients with long-standing disease may have already experienced AWO (left-censoring).
The risk of experiencing AWO at 1.5 years of follow-up was increased almost 3-fold for patients with moderate/high AS-WIS scores. This suggests that a score > 11 could raise concerns for the sustainability of a patient’s current work status. Interestingly, neither the functional capacity nor the disease activity proved to be predictive for AWO, which is in contradiction to previous studies,7,18,26,27 potentially due to the skewed nature of our population. In this well-stabilized and biologic-treated cohort, it is interesting to note a rate of 7/100 PY for severe AWO. We consider that informing the patient on this finding is important and should lead to adaptation of job conditions if necessary, but also to shared decision making in terms of treatment. Targeted interventions for maintaining employment status can include psychological support for patients who score high in the questions regarding anxiety, fatigue, or burden of disease, and/or support in pain management for patients who score high in pain-related questions.
In conclusion, we have demonstrated the predictive value of the AS-WIS for AWO. The use of this score in daily practice to identify patients at risk of AWO should be further explored, with the objective to facilitate work retention in our patients.
Footnotes
The authors declare no conflicts of interest.
- Accepted for publication August 27, 2020.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}
{kind=link}