

Abstract
Objective. To examine the effects of laser moxibustion on pain and function in patients with knee osteoarthritis (OA).
Methods. A double-blind randomized clinical trial (4-week treatment, 20-week follow-up) was conducted. A total of 392 symptomatic knee OA patients with moderate to severe clinically significant knee pain were randomly assigned to laser treatment or sham laser control group (1:1). Twelve sessions of laser moxibustion or sham laser treatments on the acupuncture points at the affected knee(s) were performed 3 times a week for 4 weeks. The primary outcome measurement was change in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score from baseline to Week 4.
Results. Among the 392 randomized participants, 364 (92.86%) completed the trial. The median WOMAC pain score decreased significantly at Week 4 in the active group than in the sham group (2.1, 95% CI 1.6–2.6, P < 0.01). At Week 24, compared to the sham laser, active laser treatment resulted in significant pain reduction and function improvement (3.0, 95% CI 2.5–3.6, P < 0.01, and 14.8, 95% CI 11.9–17.6, P < 0.01, respectively). The physical component of the quality of life significantly improved in the active group vs the sham controls at Week 4 (3.2, 95% CI 1.3–5.0, P = 0.001) up to Week 24 (5.1, 95% CI 3.3–7.0, P < 0.001). No serious adverse effects were reported.
Conclusion. Laser moxibustion resulted in statistically and clinically significant pain reduction and function improvement following a 4-week treatment in patients with knee OA.
Osteoarthritis (OA) is the most common form of arthritis and the leading cause of disability among older adults. The knee is the joint most commonly affected by OA.1 The prevalence of knee OA among people aged 60 years or older in the United States is 12.1%,2,3,4 which is expected to increase in the next 20 years.5 The prevalence of knee OA among the elderly in China is nearly 30%.6 Conventional treatment of knee OA mainly aims at alleviation of pain, including pharmacological, such as nonsteroidal antiinflammatory drugs (NSAIDs)7–15 and nonpharmacological managements.11,13 NSAIDs are associated with a moderate effect on pain relief.9,10 However, evidence on their effectiveness is limited9,10,11,12,14,15 and often associated with undesirable side effects.11,14,15 A previous review showed that appropriate treatments for knee OA included biomechanical interventions, intraarticular corticosteroids, exercise (land- and water-based), self-management and education, strength training, and weight management.13
As many as 41%16 of people with OA seek out complementary and alternative medicine therapies, including traditional Chinese medicine (TCM), acupuncture, moxibustion, and laser irradiation. According to the TCM theory, joint pain is associated with coldness and dampness. Therefore, the treatment often involves thermal stimulation on acupuncture points, known as moxibustion, by burning mugwort (Artemisia vulgaris). The effect of moxibustion is believed due mainly to its thermal effect on the skin surface.17 However, moxibustion therapy produces heavy smoke with an unpleasant smell. The smoke of moxibustion is considered a biological hazard to health18 and is therefore prohibited from use in many clinics and hospitals. More recently, low-level laser therapy has been widely used to treat musculoskeletal pain, including pain due to knee OA.19,20,21,22 We have developed a laser moxibustion (LM) device of 10.6 μm wavelength, which has the thermal nature of moxibustion without smoke and smell. Our previous small studies showed that LM may be effective in alleviating the symptoms of knee OA.23,24 The LM device was patented in 2010 (China Invention Patent ZL200910056991.4) and licensed by Shanghai Municipal Food and Drug Administration, China (20162210783). The purpose of this placebo-controlled clinical trial was to validate whether a 4-week LM treatment is effective and safe in reducing pain and improving function among patients with knee OA as compared with a sham laser control.
METHODS
This is a multisite, randomized double-blind sham-controlled trial (n = 392, 1:1). The trial protocol adhered to CONSORT guidelines25 (ISRCTN registry trial identifier 15030019, doi.org/10.1186/ISRCTN15030019). It was conducted in the outpatient clinics in 6 hospitals in Shanghai, China, and was approved by institutional review board at each site: the Shuguang hospital affiliated to Shanghai University of traditional Chinese medicine (ref: 2014-341-37-01), Shanghai East Hospital affiliated to Tongji University (ref: 2013-24), Renji Hospital affiliated to Shanghai Jiaotong University (ref: 2015-001), Shanghai Changning Tianshan Traditional Chinese Medicine Hospital (2017TSKY04), and Shanghai Tongren Hospital affiliated to Shanghai Jiaotong University (ref: 2017-32). The Shanghai Hudong hospital accepted the ethics approval of the Shuguang hospital. We have obtained patients’ written informed consent to publish the materials. We established an international data and safety monitoring board (DSMB) to monitor data safety to ensure the quality of the trial and safety of patients in the trial.25
A total of 603 patients were screened between January 2015 and November 2017, primarily through print advertisements in local newspapers and on posters distributed in nearby communities (Figure 1). Participants were included if they were 50 years old or older, reported moderate or greater clinically significant knee pain on most days during the past month, had knee pain of at least 40/100 mm on a visual analog scale (VAS), and had been diagnosed with idiopathic knee OA according to the American College of Rheumatology classification criteria.26 Kellgren-Lawrence grade ≥ 1 in the tibiofemoral joint on radiograph was also an inclusion requirement.5
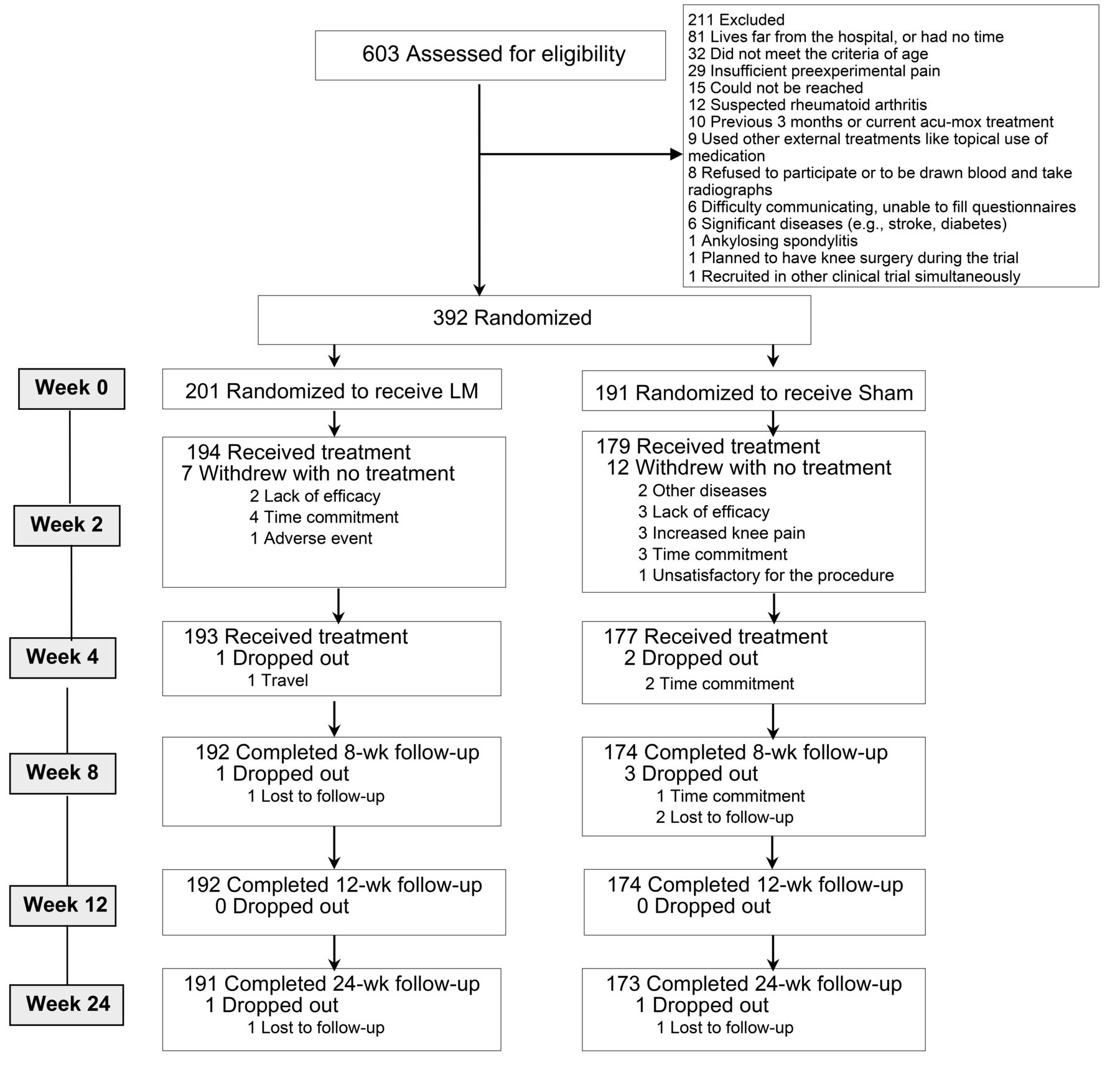
Participant flowchart. LM: laser moxibustion.
Patients with other diseases affecting the knee, such as rheumatoid arthritis, fibromyalgia syndrome, chronic fatigue syndrome, and ankylosing spondylitis were excluded. Other exclusion criteria were as follows: steroid medication or acupuncture/moxibustion treatment in the previous 3 months; intraarticular hyaluronate injection during the past 6 months; arthrocentesis or arthroscopy in the past 1 year; previous history of knee/hip replacement surgery and plans to have such surgery during the trial; use of other external treatments, such as topical medication; presence of serious medical conditions including cardiac diseases, pulmonary diseases, kidney diseases, liver diseases or malignant tumors, systemic infection or contagious diseases, and psychopathy; use of trial drugs in the past 30 days; previous participation in other laser therapies; recruitment in other clinical trial simultaneously; and inability to fill measurement questionnaires.
Randomization and blinding. The 392 eligible participants were randomly assigned to receive either active LM or sham control. Randomization sequence with random blocks was generated using computer software. Allocation concealment was ensured with disguised letter codes of the LM devices (either active or sham devices) that were generated and sent to the site coordinators by a central randomization system. After receiving the device code from the site coordinator, the device operator used the LM device labeled with that code for patient treatment. The operators were unaware of the active or sham device, as both produced the same red light. The whole procedure was supervised by the coordinators to ensure that the protocol was followed. Participants in the 2 groups were treated by trained operators. Communication among participants was discouraged and it was avoided as they were treated in separate rooms. Therefore, all involved personnel, including participants, device operators, outcome assessors, research coordinators, and statisticians, were blinded to the treatment allocation.
Interventions. LM devices were used (SX10-C1, Shanghai Wonderful Opto-Electrics Tech. Co., Ltd. and licensed by Shanghai Municipal Food and Drug Administration, China [20162210783]). The wavelength of laser irradiation was 10.6 μm, and the output power was adjusted in the range of 160–180 mW. Energy density ranged from 61.2 to 68.8 J/cm2 for 1 treatment. After the patient lay supine on a treatment table, the laser irradiation tips of the 2 LM devices were aimed to the surface of the acupuncture points. The distance from the tips to the skin surface was 2 cm, measured using a scale. Two acupuncture points were selected, namely ST35 (Dubi, located in the depression on the lateral side of the patella and the patellar ligament) and Ashi (tender point),26,27 at the affected knee. The selection of acupuncture points was based on the TCM theory used for Bi syndrome at the knee joints, and was successfully used in our previous studies.23,24 The treatments lasted 20 minutes and were performed 3 times a week for 4 weeks with a total of 12 sessions. The treatment procedure is shown in Figure 2.

Laser treatment.
The sham treatment procedure was the same as the active treatment, except no laser output irradiated from the device. However, in both active and sham devices, a red light–emitting diode with an output of 3 mW was used as visible indicator light on the skin to confirm accuracy of irradiation on the targeting acupoint. Participants were allowed to receive their usual care medications but were encouraged not to change to new drugs. In case of drug change, the name and dosage of the medication were documented.
Outcome measurements. The patients were assessed at baseline and at Weeks 2, 4, 8, 12, and 24. All assessment instruments were in the translated Chinese versions and previously validated.28,29 The primary outcomes were the change in Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)30 pain scores from baseline to 4 weeks. The WOMAC version used was in a Likert format. The WOMAC pain subscales included 5 questions, with a total of 20 points (0, no pain). For bilaterally eligible knees, only the most symptomatic knee was evaluated. Secondary outcomes included the change in WOMAC scores at Weeks 2, 4, 8, 12, and 24; health-related quality of life (Medical Outcomes Study 36-item Short Form survey [SF-36])31; VAS; and patient global assessment (PtGA). The WOMAC consists of 2 other subscales: stiffness (2 questions), 0–8 points; and physical function (17 questions), 0–68 points (the higher the scores, the worse the symptoms). VAS was used for measuring the pain, ranging from 0 mm (indicating no pain) to 100 mm (indicating worst pain). The measurements were taken at baseline and at Weeks 2, 4, 8, 12, and 24, with patients being asked, “How painful is your knee now?” PtGA of OA is evaluated on a 5-point Likert scale32,33,34 at Week 4. Patients are asked to respond to the following question: “Considering all the ways your OA affects you, how are you doing today?” (1 = very good, 2 = good, 3 = fair, 4 = poor, and 5 = very poor). Adverse events (AEs), reported by the participants and practitioners were documented at each visit, whether or not they were related to treatment. We also communicated with each participant weekly by telephone to follow up on any AE or side effect. Possible side effects of LM include skin rash, redness, and blisters. To assess the masking effectiveness of the trial, the treatment providers and participants were asked to guess their group assignment after the end of treatment at Week 4.
Blood samples were collected at baseline and Week 4 from one-third of the participants (n = 113, 56 from the LM group and 57 from the sham control group) to examine the changes in serum biochemical levels such as cartilage oligomeric matrix protein (COMP), interleukin (IL)-1β, IL-2, IL-6, IL-8, monocyte chemoattractant protein 1 (MCP-1), matrix metallopeptidase (MMP)-3, and MMP-13 (considered as important in the progress of OA). Blood samples (10 mL) were drawn at 10–11:30 am from each participant and then were stored in a refrigerator at –80°C for later analysis.
Sample size and statistical analysis. A minimum of 36% improvement in WOMAC score was considered to be clinically meaningful.35 Based on previous small-scale preliminary studies,23,24,25,36,37 a sample size of 324 participants (162 for each group) would be sufficient to detect the difference of 36% between the 2 groups to achieve a 2-sided 5% significance level with at least 80% power.38 Considering possible dropout (i.e., 17% dropout) during the trial, a total of 392 patients were thus required.
The analysis plan was determined and approved by the independent DSMB committee before the study was conducted. The primary analysis was to compare the 4-week improvement in WOMAC pain score between the treated and the controls in all randomized patients. A chi-square test was used for categorical data, and a 2-sample t test or Mann-Whitney U test was used for continuous data, to evaluate statistically significant differences in the distribution of different variables at baseline according to whether the data are normally distributed.
Two-sample t test or Mann-Whitney U test was performed for the primary (WOMAC pain) and secondary endpoints (WOMAC scores at other timepoints, SF-36, medication usage, and serum levels of different cytokines) at each timepoint. A chi-square test was performed for the categorical data (self-evaluation, credibility of the sham assessment, and safety assessment). For nonnormally distributed variables, 95% bootstrap CI, instead of large sample normal-based interval, was calculated. All statistical analyses were conducted using SPSS (version 23.0, IBM Corp.). All reported P values were 2-sided and used a significance level of 0.05.
RESULTS
After initial screening, 392 patients were randomly assigned to either the LM group (n = 201) or the sham LM group (n = 191). Three hundred and sixty-four patients (92.86%) completed the study and whose data were available for analysis (Figure 1). Of these, 193 patients in the LM group and 177 patients in the sham group completed all 12 sessions of therapy. There were no additional missing data other than from those withdrawn from the study; these data were imputed using last observation carried forward. Baseline characteristics were similar between the groups (Table 1). Most study patients were women (75%). No significant difference was found between the 2 groups in age, sex, disease course, medication use, severity of disease, WOMAC scores for knee pain or physical function, and cytokine level. This result suggests that the 2 groups were comparable.
Demographic and baseline characteristics of the participants.
Primary outcome. At Week 4, the patients receiving LM treatment reported more reduction in WOMAC pain score of 2.4 (36.4%) compared with those receiving sham LM of 0.1 (1.5%). A significant difference was found between the 2 groups (2.1, 95% CI 1.6–2.6, P < 0.01; Table 2). At Week 4, 127 patients receiving LM treatment reported more than 36% pain reduction in WOMAC pain score (63.2%) compared with 45 patients receiving sham LM (23.6%). A significant difference was found between the 2 groups (P < 0.01).
Change from baseline in WOMAC and VAS outcomes of the participants.
Secondary outcomes. WOMAC total scores including pain, physical function, and stiffness at Weeks 2, 4, 8, 12, and 24 improved significantly more in patients who received active LM than those who received sham LM (Table 2). The patients in the active LM group reported more VAS pain score reduction than those in the sham LM group at all timepoints (Table 2).
No significant differences were noted in medication usage between the 2 groups. For the medication intake, we counted the number of patients who did not need to take medicine as the measurement. Before treatment, 159 patients of the LM group and 164 patients of the sham group did not take any medicine (P = 0.061). After 4 weeks of treatment, 175 patients of the LM group and 156 patients of the sham group did not take any medicine (P = 0.98); at Week 24, 176 patients of the LM group and 155 patients of the sham group did not take any medicine (P = 0.81).
Quality of life measured using SF-36 showed that the physical component summary score significantly improved by 3.2 at Week 4 in the LM group compared with the sham control group (95% CI 1.3–5.0, P = 0.001) up to Week 24 (5.1, 95% CI 3.3–7.0, P < 0.001). No difference was found in the mental component summary score between the 2 groups (0.8, 95% CI –1.0 to 2.6, P = 0.38 at Week 4; 1.8, 95% CI –0.1 to 3.6, P = 0.06 at Week 12; 1.1, 95% CI –0.7 to 2.9, P = 0.238 at Week 24). Among the 8 components of the SF-36 assessment, the active LM group showed statistically significant improvement in 5 components including physical functioning, role physical, bodily pain, social functioning, and role emotional at Weeks 4, 12, and 24 (P = 0.025 to P < 0.001) compared with the sham LM group (Table 3). PtGA was evaluated at Week 4. The rank-sum test showed that the patients in the active LM group reported better overall satisfactory scores (230.09) than those in the sham control group (136.88, P < 0.01).
SF-36 scale scores over time.
After a 4-week treatment, among all the serum biomarkers including COMP, IL-1β, IL-2, IL-6, IL-8, MCP-1, MMP-3, and MMP-13, only COMP improved in the active LM group compared with the sham control group. At the baseline, median (Q1, Q3) of serum COMP of the LM group was 288.3 (251.0, 340.0) pg/mL, compared with the COMP of 291.0 (253.0, 414.1) pg/mL in the sham group (P = 0.42). At Week 4, COMP in the LM group was 270.2 (240.7, 305.9) pg/mL, while it was 301.0 (260.2, 364.3) pg/mL in sham group (P = 0.02; Table 4).
Changes of serum biomarkers highly related to the progress of OA in participant serum.
Assessment of patient blinding was conducted at Week 4 following treatment completion. A total of 170 patients (88.1%) in the LM group and 159 patients (89.8%) in the control group were unsure of their group allocation. Only 20 (9.95%) in the active LM group and 5 (2.62%) in the control group guessed their allocation correctly. The chi-square test showed P = 0.46, suggesting successful blinding in patients. All 21 treatment providers were unaware of the treatment types (active LM or sham LM) they had delivered.
Thirty (7.65%) AEs (24 [11.94%] in the active LM group and 6 [3.14%] in the sham control group) were reported among the 391 participants. Skin rash was the most common AE (n = 21) reported by those who received active LM, and all recovered within 3 days.
DISCUSSION
Over a 4-week treatment period of thrice-weekly treatments, 10.6-μm LM (61.2–68.8 J/cm2) showed significant efficacy in relieving knee pain and function improvement compared with sham LM measured using WOMAC scores and VAS. The effect was prolonged up to 20 weeks after the completion of laser treatment. Our findings are similar to those of previous reports.36,37 In a systematic review reported by Wyszynska and Bal-Bochenska,36 high-intensity laser therapy produces significant benefit in pain reduction and function improvement in patients with knee OA. However, most of these studies suffered from methodological flaws such as small sample size,36,38,39 insufficient treatment time,19 and inadequate follow-up time.40 The strength of our laser treatment was that our laser device used CO2 laser, which produces a far-infrared light beam of 10.6 μm, whereas previous studies used Gal-Al-As laser with wavelengths ranging from 830 nm to 1064 nm.41 The unique feature of 10.6-μm LM is that it produces potent superficial heat,42 which mimics moxibustion in TCM.
According to the TCM theory, joint pain, such as in knee OA, is considered Bi syndrome, which is caused by wind, cold, and dampness affecting the joint. Traditionally, thermal stimulation produced by burning A. vulgaris is commonly used to treat Bi syndrome to eliminate cold and dampness in the joints.27 However, traditional moxibustion has its limitations in clinical practice due to the nature of smoke and its smell. Some studies suggested that the smoke may be hazardous to health.43 The effect of moxibustion is believed to be due mainly to its thermal effect on the skin surface. In the present study, we used 10.6-μm CO2 laser beam, which produced a thermal effect similar to that of traditional moxibustion, but without smoke and smell, for treating knee arthritic pain.22,35,44
A recent systematic review41 indicated that the best available current evidence does not support the effectiveness of laser treatment as therapy for patients with knee OA. Variation in the effectiveness of laser treatment in patients with knee OA could be related to a variety of dosages, treatment schedules, energy density, outputs, and wavelengths. Soleimanpour, et al performed laser therapy in knee OA with 810 nm at 6 J/cm2 and 890 nm at 10 J/cm2, 3 times a week for a total of 12 sessions; results showed it to be effective in reducing pain.45 Hinman, et al19 used a diode laser device (measured output 10 mW and energy output 0.2 J/point), the output and energy of which was much lower than those of both the CO2 laser used in our trial (output 160–180 mW and energy output 192–216 J/point) and the recommended treatment dose for low-level laser therapy by the World Association for Laser Therapy46,47 (minimum energy output 1 J/point for 904 nm laser, minimum energy output 4 J/point for 780–820 nm laser). Energy outputs of most of laser treatment trials were lower than what we used; this may be one of the main reasons that some trials failed to detect the benefit of laser treatment.
We conducted a double-blind clinical trial achieved through active and sham laser devices that appeared the same; additionally, both patients and the operators of the laser devices were unaware of the group allocation. Further validation testing showed that the blinding was successful, and all other investigators were also blinded to the treatment allocation. Second, the patient compliance rate of the trial was high (92.86%), possibly because most of the participants were elderly and retired, with more time for treatment. Most of the participants lived near the hospitals. Third, the incidence of side effects observed during trial was low (7.65%).
Some studies suggested that serum COMP is potentially useful to be a prognostic marker of disease progression for joint injury.48,49 COMP is a large pentameric glycoprotein that interacts with multiple extracellular matrix proteins in the cartilage.50 Our study suggests that the effect of the 10.6-μm laser may be associated with protecting the cartilage from degeneration in patients with knee OA.
This study has a number of limitations. First, the trial was conducted at 6 sites and the number of subjects recruited from each site varied, which may have introduced selection and conditional bias. Second, the treatment used only 2 fixed points, whereas in real-world Chinese medicine practice, the point selections are often individualized based on the syndrome differentiation according to TCM principles. Third, although we asked patients to document any additional medicines using a medication usage log, we did not know for sure whether all the patients complied with this request. However, we hope the randomization would address this issue, as we assume both groups would have a similar number of participants who may not follow our requirement.
A 10.6-μm LM is superior to sham laser with clinically relevant benefits for 24 weeks in treating knee OA. The effectiveness of laser treatment may be related to COMP elevation, which controls inflammation and protects the cartilage. Further research is warranted to understand the long-term efficacy and the mechanism of action of laser intervention.
ACKNOWLEDGMENT
We would like to thank Drs. Jinghua Ge, Lanlan Liu, Chenhuan Ding, and Feng Yin for their assistance in patient recruitment; Dr. Lin Lin for part of the statistical analysis, and Dr. Yang Mingxiao for editorial support. The DSMB members include Prof. Jianping Liu (Chair) from Beijing University of Chinese Medicine (epidemiologist), Prof. Wolfgang Schwarz from Goethe-University Frankfurt (biophysicist), Prof. Bing Zhu from China Academy of Chinese Medical Sciences (acupuncturist), Prof. Mac Hochberg from University of Maryland School of Medicine (rheumatologist), and Prof. Guoliang Tian from University of Hong Kong (statistician). We would also like to thank Editage (www.editage.com) for English language editing.
Footnotes
This trial was supported by National Natural Science Foundation of China (81320108028) and National Program on Key Basic Research Project of China (2015CB554505).
Role of the Funder/Sponsor: The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Dr. Zhao and Dr. Cheng contributed equally to this manuscript as first authors.
XS and KC have had a patent issued for a type of laser therapy apparatus simulating the infrared radiation spectrum of traditional Chinese moxibustion (China Invention Patent ZL 200910056991.4; issued December 1, 2010). The remaining authors declare no conflicts of interest.
- Accepted for publication June 19, 2020.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}
{kind=link}