

Abstract
Objective. The modified Rodnan skin score (mRSS) remains the preferred method for skin assessment in systemic sclerosis (SSc). There are concerns regarding high interobserver variability of mRSS and negative clinical trials utilizing mRSS as the primary endpoint. High-frequency ultrasound (HFUS) allows objective assessment of cutaneous fibrosis in SSc. We investigated the relationship between HFUS with both mRSS and dermal collagen.
Methods. Skin thickness (ST), echogenicity, and novel shear wave elastography (SWE) were assessed in 53 patients with SSc and 15 healthy controls (HCs) at the finger, hand, forearm, and abdomen. The relationship between HFUS parameters with mRSS (n = 53) and dermal collagen (10 patients with SSc and 10 HCs) was investigated. Intraobserver repeatability of HFUS was calculated using intraclass correlation coefficients (ICCs).
Results. HFUS assessment of ST (hand/forearm) and SWE (finger/hand) correlated with local mRSS at some sites. Subclinical abnormalities in ST, echogenicity, and SWE were present in clinically uninvolved SSc skin. Additionally, changes in echogenicity and SWE were sometimes apparent despite objectively normal ST on HFUS. ST, SWE, and local mRSS correlated strongly with collagen quantification (r = 0.697, 0.709, 0.649, respectively). Intraobserver repeatability was high for all HFUS parameters (ICCs for ST = 0.946–0.978; echogenicity = 0.648–0.865; and SWE = 0.953–0.973).
Conclusion. Our data demonstrate excellent reproducibility and reassuring convergent validity with dermal collagen content. Detection of subclinical abnormalities is an additional benefit of HFUS. The observed correlations with collagen quantification support further investigation of HFUS as an alternative to mRSS in clinical trial settings.
Aberrant tissue remodeling is a pathological hallmark of systemic sclerosis (SSc), resulting in fibrosis of skin and organs. SSc skin pathology is complex, comprising 3 distinct pathological phases.1,2 An early inflammatory phase with cutaneous edema1,3,4 often manifests as “puffy fingers.” This evolves into a longer indurative phase,1 where increased dermal collagen deposition causes thickened fibrotic skin.5 The indurative fibrotic phase typically plateaus clinically before entering an atrophic stage, characterized by natural regression of fibrosis.4 At this stage, lesional skin may be thinner than the skin of healthy controls (HCs), but tethering to the underlying subcutis can render the skin immobile, confounding clinical judgement of skin thickness.1
The modified Rodnan skin score (mRSS)6 is a quick, noninvasive clinician assessment that correlates with histological grading of skin fibrosis.7 The mRSS is used in routine clinical practice and is associated with functional disability8 and survival.9,10 It remains the preferred method for assessment of skin involvement in clinical trials. The method is subjective and, while the intraobserver variability is acceptable,11 there is poor interobserver agreement,11,12 which has implications on its reliability and sensitivity to change as an outcome measure in clinical trials. A number of recent trials of promising antifibrotic interventions have failed to demonstrate statistically significant improvements in mRSS despite encouraging preclinical data and apparent improvement in composite clinical endpoints.13,14 The mRSS also lacks the sensitivity to differentiate between clinically indistinguishable pathological phases such as inflammatory edema vs established fibrosis, which may also influence trial findings.15
Ultrasound (US) was proposed as an objective method for assessing skin > 40 years ago.16 There has been more recent research interest in US for assessing quantitative and qualitative changes in SSc skin, including skin thickness (ST),17–24 stiffness (elastography),21,25,26 and edema (low echogenicity).3,18,19 The objective nature of US potentially overcomes limitations of the mRSS. Nonetheless, studies have reported poor agreement between local mRSS assessment and objective ST using high-frequency US (HFUS; > 15 MHz).22 Most previous studies of US elastography used manual displacement of the skin (prone to procedural variation) to assess strain elastography. Newer shear wave technology measures the propagation of a “pushing” pulse generated by the US transducer through the tissue, providing consistency and reducing influence from subcutaneous tissues.27,28,29 The interrelationship between ST, echogenicity, and elastography has not been fully explored. Further, no previous studies have directly correlated US assessment with histological analysis of dermal collagen deposition. The aim of this study was to further explore the potential of HFUS as a noninvasive tool for assessing SSc skin involvement. Specifically, we have examined the interrelationship between HFUS parameters, local mRSS, and histological dermal collagen content.
METHODS
Detailed methodology is available in Supplementary Material 1 (available with the online version of this article). Patients fulfilling the 2013 American College of Rheumatology/European League Against Rheumatism classification criteria30 were enrolled from the SSc clinic at the Royal National Hospital for Rheumatic Diseases, Bath, UK. HCs were recruited from members of staff and relatives of participants with SSc. All participants underwent clinical and HFUS assessments.
Ethical approval. Regulatory approval was granted from the NHS Research Ethics Committee (reference 14/SW/1165). All study procedures were undertaken in line with the Declaration of Helsinki with written informed consent prior to study enrollment.
Clinical and US assessment. All study investigations were performed by the same observer (VAF). The total and local mRSS1 at each US region of interest (ROI) were assessed by a single observer (VAF). US was performed using standardized settings on the same device (Toshiba APLIO A500) for shear wave elastography (SWE; 14 MHz), ST, and echogenicity (both 18 MHz) at 4 ROI: proximal middle finger, dorsal hand, distal dorsal forearm, and abdominal epigastrium. Variability of HFUS was assessed for each parameter, at each ROI, in all participants.
US image analysis. ST (mm) at the hand, forearm, and abdomen was measured as the distance between the external surface of the epidermis and dermo-subcutis interface. Due to challenges identifying the dermo-subcutis junction in some participants with SSc, the distance between the external surface of the epidermis down to the finger extensor tendon (clearly visible in all participants) was used to measure ST in the finger, consistent with previous studies.31 Dermal echogenicity was recorded as the mean brightness of grayscale (scale 0–255) using Image J (https://imagej.nih.gov/ij), such that low echogenicity suggested tissue edema and increased echogenicity was suggestive of fibrosis. Images were analyzed for ST and echogenicity in batches and without reference to mRSS scores. For SWE, the APLIO A500 built-in software calculated the mean SWE (kPa).
Skin biopsy and semiquantification of collagen density. Optional skin biopsies were obtained from the forearm at the site of HFUS assessment in accordance with a purposive sampling framework that aimed to capture a mix of early/late and limited/diffuse SSc. Formalin-fixed, paraffin-embedded tissue sections were stained for collagen with Masson trichrome (Sigma) and quantified using Image J to calculate a mean intensity (grayscale, 0–255) of blue color across the tissue section, integrated density (mean intensity × blue pixel area), and total sum of the grayscale (total sum of the intensity of each blue pixel). Histological ST was measured on the same tissue sections using Image J.
Statistical analysis. Statistical analyses were performed using SPSS (v24; IBM Corp.). Normally distributed patient demographics were compared using parametric tests including independent t test and chi-square test. Statistical comparison of ultrasound data between patients with SSc (whole group) and HCs utilized Mann-Whitney U test (presented as group median [IQR]). Comparisons made with grades of local mRSS utilized Kruskal-Wallis tests. Posthoc analysis (Dunn test) was applied for comparison between 2 individual groups when Kruskal-Wallis achieved significance.
Repeat assessments were used to calculate intraclass correlation coefficient (ICC) for intraobserver variability. SSc HFUS data for skin thickness at each site was subcategorized according to atrophic skin (< mean +2 SD of controls), thickened skin (> mean +2 SD of controls), or normal skin thickness. Multiple linear regression analysis for the 3 HFUS parameters and mRSS to predict skin collagen content was performed using backwards exclusion (for echogenicity).
RESULTS
Participants. Fifty-three patients with SSc were enrolled (45 with limited cutaneous SSc [lcSSc] and 8 with diffuse cutaneous SSc [dcSSc]) alongside 15 HCs. A summary of the demographics and group median HFUS findings of the participants with SSc and HCs is presented in Table 1. Mean SSc disease duration was 11.7 years, with 26% (14 SSc, including 10 lcSSc) being within 5 years of disease onset or lcSSc to dcSSc transition. Patients with SSc were significantly older and were more likely to be administering vasodilator therapies compared to HCs. Across the whole cohort, skin thickness and SWE were generally higher at each ROI in patients with SSc compared to HCs (Table 1). Dermal echogenicity was lower at the finger but higher at the forearm in patients with SSc compared to HCs. HFUS data values according to mRSS are illustrated in Supplementary Table 1 (available with the online version of this article).
Demographic and ultrasound data for SSc and healthy control groups.
Relationship between HFUS assessment of ST and clinical assessment using mRSS. There was a linear relationship between HFUS median ST and the local mRSS at the hand (P = 0.034) with significantly higher skin thickness in patients with mRSS = 1 and mRSS = 2 compared with HCs (P = 0.043 and P = 0.015, respectively; Figure 1). Similar trends were evident at the finger (P = 0.137, not significant [NS]) and forearm (P = 0.012; Supplementary Table 1, available with the online version of this article). For example, the skin thickness at the forearm in patients with mRSS = 1 was significantly higher than in patients with mRSS = 0 (P = 0.009). These relationships are further illustrated by weak–moderate correlation of HFUS ST with local mRSS at the hand and forearm (Table 2), but not finger or abdomen. Similar correlation with ST is extended to the total mRSS (Table 2).
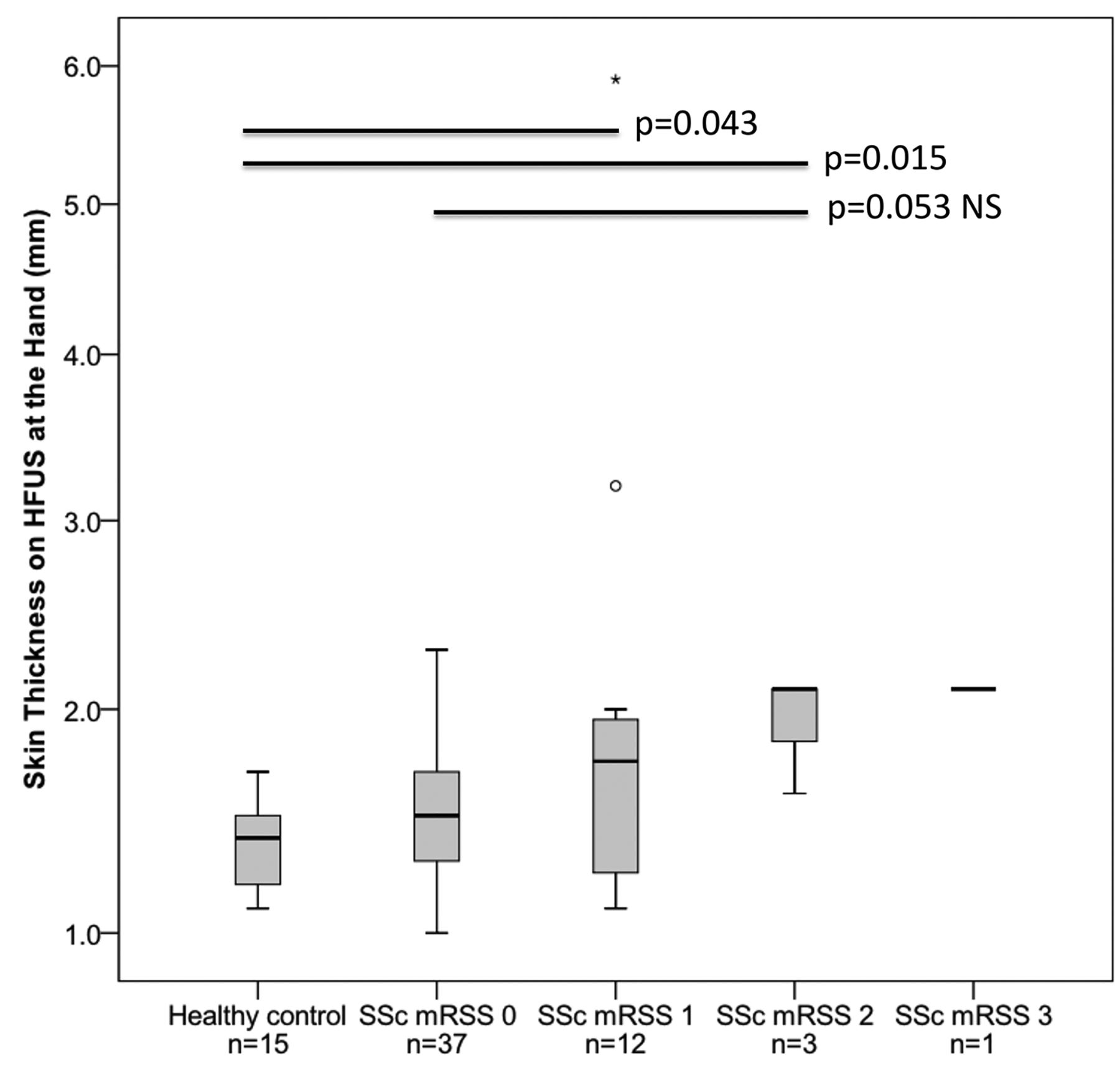
Objective HFUS assessment of skin thickness according to local mRSS at the hand. There were strong trends for objective hand skin thickness on HFUS to increase from normal HC skin across increasing skin scores in patients with SSc (P = 0.034, Kruskal-Wallis). P values shown in between 2 groups represent posthoc analysis (Dunn test). Circle and asterisk illustrate group outliers. HC: healthy controls; HFUS: high-frequency ultrasound; mRSS: modified Rodnan skin score; NS: not significant; SSc: systemic sclerosis.
Correlation between clinical, histological, and ultrasound assessment of skin.
When mRSS = 0, the median ST at the forearm (P = 0.046) and abdomen (P = 0.026) was actually lower in patients with SSc compared with HCs, reflecting atrophic skin. Skin thickness at the hand and fingers was similar in patients with SSc and HCs when mRSS = 0 (Supplementary Table 1, available with the online version of this article).
With consideration for the influence of age on skin, ST correlated only with age in the control group at the forearm ROI (r = –0.390, P = 0.001), a site at which there was no significant difference between diagnostic groups (Table 1). There was no correlation between ST and age at any site for patients with SSc, or finger, hand, or abdomen in HCs. Additionally, there was no correlation between echogenicity or SWE with age for either HCs or patients with SSc.
Relationship between US assessment of skin stiffness and clinical assessment using mRSS. There was a linear relationship between median skin stiffness (SWE) and local mRSS at the finger and hand (P = 0.039 and P = 0.007, respectively; Figure 2, Supplementary Table 1, available with the online version of this article). Correlation between SWE and local mRSS confirmed these relationships (Table 2). There was a similar trend for median SWE at the forearm and abdomen (P = 0.062 NS and P = 0.035, respectively; Supplementary Table 1). Correlation with local mRSS did not achieve significance (although numbers of patients with higher skin scores at these sites were low; Table 2). Correlation between SWE and total mRSS was not significant.

Ultrasound assessment of skin quality according to local mRSS at the finger and hand. Echogenicity (white) and SWE (gray) are shown for the (A) finger and (B) hand. Skin stiffness on SWE increased progressively at each region of interest from controls across increasing local skin scores in patients with SSc (P = 0.039 at the finger, P = 0.007 at the hand; Kruskal-Wallis). At the finger and hand, echogenicity tended to progressively reduce from HC across mRSS = 0 and mRSS = 1, suggesting cutaneous edema followed by an increase in echogenicity at higher mRSS grading (P = 0.008 at the finger, P = 0.234 at the hand; Kruskal-Wallis). Numbers for mRSS = 3 were small at both finger and hand. P values shown in figure for comparisons between 2 groups represent posthoc analysis (Dunn test). mRSS: modified Rodnan skin score; SSc: systemic sclerosis; SWE: shear wave elastography.
SWE values at both the abdomen (P = 0.035) and hand (P = 0.023; Figure 2) were significantly higher in patients with SSc with mRSS = 0 compared to HC. Further, when skin thickness was objectively normal on HFUS, there was still evidence of increased SWE at both the finger (71.2 kPa [49.0–80.8] vs 33.3 kPa [21.8 40.6]; P < 0.001) and hand (36.2 kPa [30.7–42.5] vs 27.0 kPa [15.9–40.4]; P = 0.042) compared to HCs. Taken together, these findings indicate that HFUS is capable of identifying aberrant tissue remodeling, even when the dermis is of objectively normal thickness and clinically normal to palpation. We noted that in patients with SSc with high local skin scores at the finger, it was sometimes difficult to obtain an accurate SWE reading on the first attempt. Iagnocco, et al, reported similar problems for finger elastography in all participants, including controls, and thus concluded that this may be due to interference from the closely underlying bone.25 In our study, this practical difficulty did not occur with HCs or the patients with SSc with lower local mRSS. Thus, we concluded that it likely occurred due to the severity of pathology within the soft tissues rather than bony interference, which may limit its application for more severe skin lesions. Despite this, overall we still obtained high-quality reproducible data by this technique.
Relationship between HFUS assessment of dermal echogenicity and clinical assessment using mRSS. Unlike ST and SWE, there was not a linear relationship between median echogenicity and local mRSS at any ROI, reflected in a lack of correlation with local mRSS. Total mRSS only correlated with echogenicity at the forearm (r = –0.337, P = 0.014), which might have occurred by chance due to repeated testing. Echogenicity was, however, significantly lower at the finger in patients with SSc with mRSS = 0 (P = 0.028), mRSS = 1 (P < 0.001), or mRSS = 2 (P = 0.023) compared to HCs, suggesting more edema in the former (Figure 2). Further, there was a trend toward reduced echogenicity in patients with SSc when ST was objectively normal on HFUS at the finger (52.0 [48.0–69.0], n = 7 vs 67.0 [55.0–81.0], P = 0.087). It is possible that this reflects tissue edema within this cohort of predominantly lcSSc. We were unable to identify differences in echogenicity (or SWE) between early and late SSc (</> 3 yrs since first non–Raynaud phenomenon symptom) or correlation with disease duration (data not reported). This may be due to small numbers of participants with early SSc and few treatment-naïve participants (both vasodilator and disease-modifying antirheumatic drugs). Further work is required to explore the potential relationship between HFUS echogenicity and the edematous phase of SSc. Nonetheless, our findings suggest the capacity of HFUS to identify changes in skin quality when skin thickness is otherwise objectively and clinically normal.
Interrelationship between US parameters. There was no correlation between echogenicity and either SWE or ST. Only a small number of weak correlations between ST and SWE were identified (hand: r = +0.454, P = 0.001; finger: r = –0.366, P = 0.007), although this might have been a consequence of multiple testing and was therefore not considered relevant. The general lack of consistent relationships between the 3 parameters may reflect the complex and nonlinear evolution of SSc skin pathology. For example, an area of normal ST in SSc may reflect the early edematous change prior to overt thickening or regression of fibrotic skin.
Histological validation of US and mRSS for assessing skin fibrosis. There were strong correlations between objective measurements of ST on HFUS and each of the following: the area, integrated density, and sum of the grayscale for collagen staining for both the overall cohort (SSc + HC) and the SSc group alone (Table 2). The same patterns of strong correlations were observed between SWE and collagen staining for participants with SSc (Table 2, Figure 3). Of note, SWE associations did not achieve significance for the overall cohort (P = 0.056). There was no relationship between echogenicity and collagen content at the forearm, suggesting that increased echogenicity may reflect other features of skin fibrosis.
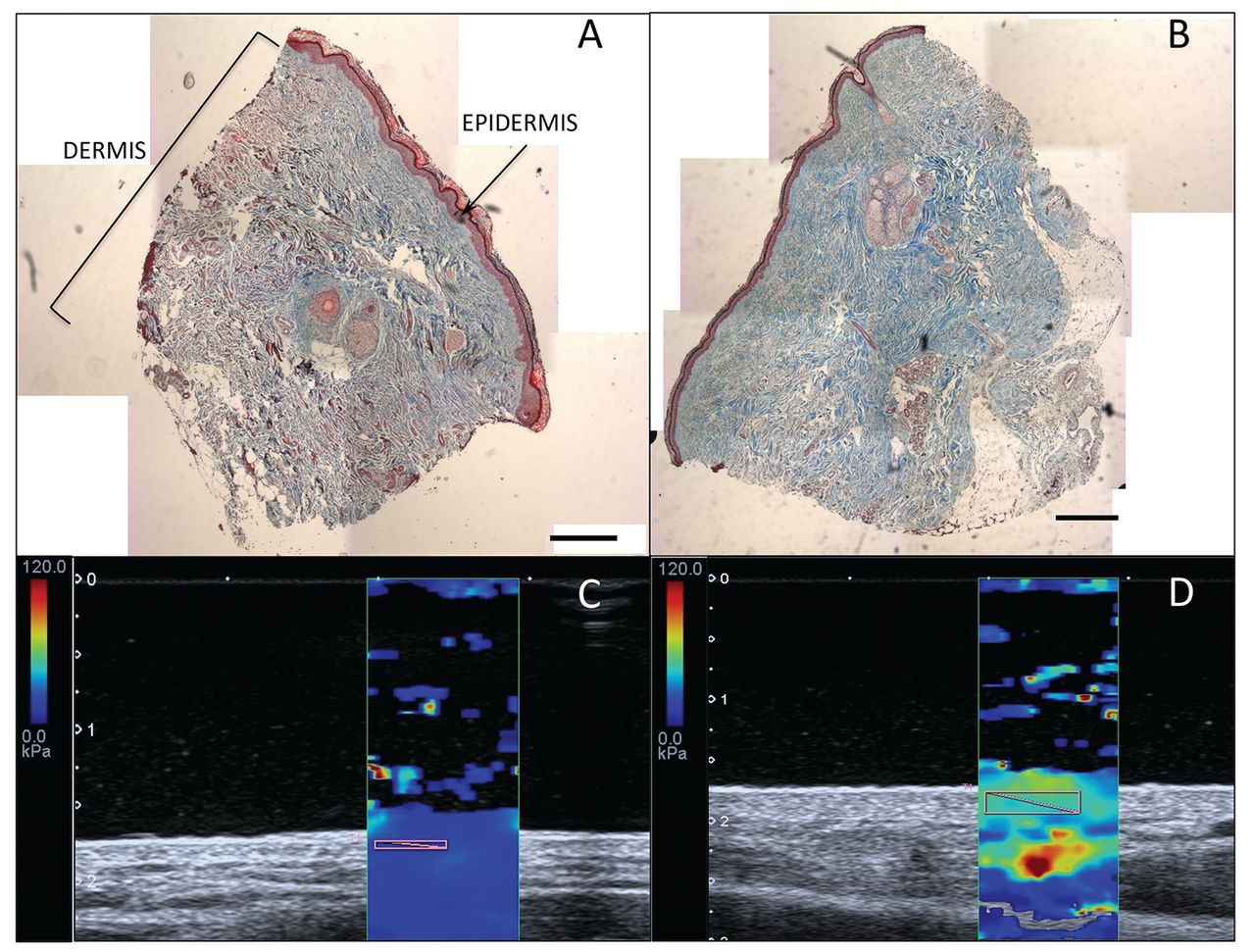
Assessment of skin fibrosis by Masson’s Trichrome and elastography. (A, B) Histological collagen content (blue) of forearm skin biopsies are shown by Masson trichrome staining (C,D) with paired shear wave elastography (SWE) assessment at the same site for respective participants, demonstrating skin stiffness. A HC representative of the control group mean for integrated density of collagen staining (A) has low skin stiffness on SWE (C). The participant with SSc with the maximum integrated density of collagen staining for the SSc group shows visibly increased collagen staining in the dermis (B) with increased skin stiffness (D). Scales: trichrome scale bar (500 μm). SWE color scale: stiff (red) to soft (blue). Ultrasound white numeric scale: depth (cm). HC: healthy controls; SSc: systemic sclerosis.
Local mRSS at the forearm (but not total mRSS) also correlated strongly with collagen quantification in patients with SSc (Table 2). Multiple linear regression analysis confirmed HFUS ST, SWE, and local mRSS at the forearm as significant predictors of local collagen deposition (integrated density) in SSc (R2 = 0.891, P = 0.001).
HFUS and histological ST shared a moderate but nonsignificant correlation (whole cohort [n = 20]: r = +0.417, P = 0.067; and SSc group only [n = 10]: r= +0.483, P = 0.157).
Variability of HFUS measurements. Overall, reproducibility was very good, with very strong correlation between paired measurements for ST (ICC 0.946–0.978) and SWE (ICC 0.953–0.973) and strong correlation for echogenicity (ICC 0.648–0.865; Table 3).
Intraobserver variability in ultrasound parameters.
DISCUSSION
We have demonstrated for the first time, to our knowledge, that ST and SWE on US correlate strongly with dermal collagen deposition. Confirmation of excellent reproducibility reported in earlier studies17,19,20,21,23,25,26 also suggests that the technique is reliable for such an application with appropriate training. Only 1 previous HFUS study undertook paired skin biopsies, which reported binary normal or abnormal skin based on thickening of collagen bundles32 but made no direct correlation with HFUS data. One other study reported an association between expression of extracellular matrix markers and increased HFUS ST and echogenicity, but histological analysis was not performed.18 The lack of correlation between echogenicity and collagen staining in our data suggests that increased echogenicity may reflect other dermal components of fibrotic skin, such as perhaps fibrillin and elastin rather than collagen alone, but may also be influenced by the shorter disease duration in the former study.
Recent work has described distinct gene expression signatures in SSc skin pertaining to the inflammatory and fibroproliferative phases.33 HFUS may be able to differentiate between such molecular subsets through examination of ST, SWE, and echogenicity. While the technology for efficient machine learning is advancing,33 gene expression profiling relies on invasive tissue sampling and is not practical to repeat throughout the disease course. Further studies incorporating paired genetic profiling alongside HFUS analysis would be valuable in further developing HFUS as a noninvasive method for assessing SSc skin involvement.
The convergent validity between collagen quantification with ST and mRSS suggests that both noninvasive measures reflect skin fibrosis (at least at the examined forearm). The disparity between the strong correlation of collagen with SWE despite a nonsignificant relationship between SWE, and local mRSS may be a reflection of small numbers of patients with mRSS ≥ 2. This may also account for the nonsignificant relationship between HFUS and histological ST.
We identified HFUS abnormalities in SSc skin quality when ST was either clinically or objectively normal. Previous studies have demonstrated similar findings with ST3,24,32 and more recently with SWE,27,34 although we are the first to demonstrate such abnormalities using dermal echogenicity. The overlap and wide ranges of our HFUS data across mRSS groups has been demonstrated previously3,23 and may be due in part to mixed cohort subtypes and disease duration, but speaks further to the discriminant validity of HFUS over mRSS. The incorporation of HFUS as a surrogate endpoint for skin involvement in SSc clinical trials may overcome issues around the subjectivity and poor interrater reliability of mRSS, potentially allowing treatment efficacy to be assessed in smaller single-blinded studies. Other noninvasive imaging modalities, such as optical coherence tomography, have been proposed as potentially attractive methods for objectively assessing skin involvement in SSc.35,36,37 The major limitations of all such methods are the need for expensive equipment as well as labor-intensive image acquisition and analysis, particularly if assessment is required at multiple sites.
The lack of correlation between US parameters across the ROI in our data is in contrast to Hesselstrand, et al, who reported a relationship between echogenicity and ST,18 which may be due to shorter disease duration and proportionally more dcSSc in their cohort. Larger studies are needed for more sensitive subgroup analyses to further explore the relationship between HFUS parameters at different anatomic sites and within different subgroups of SSc. Elastography may be additionally supportive by confirming the dermal interfaces and improving the accuracy and reproducibility of ST measurement.21
There are limitations to our study. Notably, the SSc group in our study had a statistically significantly older mean age, which could be considered to have an influence on skin thickness and elasticity. However, normal values for ST according to age have been described using 20 MHz HFUS and shown only 0.04–0.09 mm difference between 50–59 and 60–69 year age groups at our ROI.38. Additionally, SWE appears to reduce with aging skin,34 in contrast to the higher values in our older SSc group. We acknowledge that this is a weakness of the study, but do not feel that it lead to false-positive results. We have demonstrated excellent intraobserver reliability but further work should examine interobserver reliability that may be optimized using defined anatomical landmarks or transient skin surface markings. Additionally, the assessor was not truly blinded to the mRSS scores when performing HFUS, which may influence manual placement of the electronic calipers for ST measurement. We have assessed HFUS in a comparatively large number of subjects with SSc compared to previous studies, but with a minority of patients with early SSc and dcSSc in a single-center, cross-sectional study. SSc is a heterogeneous disease and larger longitudinal studies with greater numbers of treatment-naïve patients with early SSc and dcSSc will be important in defining HFUS parameter evolution, in allowing greater between-group comparisons, and in considering the application for clinical trials. It was surprising that our cohort of largely established patients with SSc demonstrated reduced finger echogenicity. While transition from the edematous to fibrotic phase is generally considered an early event in SSc, the natural history and timing of such transitions has not been fully described and may differ between limited and diffuse subsets. Further longitudinal studies are needed to interrogate this.
US has some limitations as a skin-assessment tool. Ultrasonography requires focused learning of both basic physics and procedural skill. As such, ultrasonography would require standardized assessor certification and standardized protocols if it were to be applied as an outcome in SSc clinical trials. Nonetheless, US is increasingly part of rheumatologists’ training,39,40,41 and acquiring the skills to assess skin is arguably easier than assessing the synovium or major organs.
At 18 MHz, the dermo-subcutis junction at the proximal finger was not easily distinguishable, which we hypothesized may be due to a combination of sclerodermatous changes in the dermis creating a similar echo to the hypodermis, thus reducing the echo interface, as well as pathological subcutaneous fat atrophy in the disease group at a site that naturally has little fatty tissue, even in healthy subjects. Similar issues have been reported in studies using optical coherence tomography, with reduced clarity of the dermoepidermal junction and papillary-reticular dermis interface in the scleroderma disease state.37 This is further reflected by previous reports of increased interobserver variability in HFUS dermal thickness measurement at the finger compared to other anatomical sites.19 Higher frequencies of HFUS may provide better skin assessment than those in the lower end of the high-frequency range and improve sensitivity for identifying proximal skin thickening in lcSSc,24 although additional work is necessary to determine the optimal frequency.
SWE of skin reports a mean quantitative value across the region of interest, which does not reflect the heterogenicity within that tissue, potentially increasing error. The HFUS technology utilized in this study calculates an SD for SWE across the region of interest, but its meaning is easily lost by group analysis under statistical interrogation. This value is perhaps more useful when paired with a visual assessment of the regional color map (Figure 3), to make a subjective interpretation of tissue heterogeneity. Similar reflections are also relevant for echogenicity. Additionally, the relationship between shear wave propagation and the Young modulus makes some assumptions about tissue properties,29 the exploration of which is beyond the aim of this study. However, our results, combined with recent studies examining pathological skin,27,42 suggest SWE can be considered a reasonable reflection of fibrotic change.
In conclusion, the observed correlations with collagen quantification support further investigation of HFUS as an alternative to the mRSS. Skin thickness and SWE are highly reproducible parameters and have good convergent validity with local collagen burden. Further, HFUS identifies changes in SSc skin quality at both clinically lesional and nonlesional skin, which may be of benefit in clinical trials. Further studies are needed to include larger numbers of patients with early SSc and dcSSc, with biopsies from additional anatomical locations. Comparison between HFUS parameters and paired genenetic signatures may further support the development of HFUS as a noninvasive tool for assessing SSc skin involvement.
Footnotes
This work was supported by Scleroderma & Raynaud’s UK.
JDP has received speaker’s honoraria and research grant support (> $10,000) from Actelion Pharmaceuticals and has undertaken consultancy work for Actelion Pharmaceuticals and Boehringer Ingelheim. SLB has received educational support and has undertaken consultancy work for Boehringer Ingelheim. ABM has received funding from UCB, Janssen, and Pfizer; and holds shares in Ikusda Therapeutics. SGW has received funding from UCB, Pfizer, Novartis, GSK, and Boehringer Ingelheim. VAF, DJH, and JAS have no conflicts of interests.
- Accepted for publication October 16, 2020.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}
{kind=link}
{kind=link}