

Calcinosis is a well-known manifestation of systemic sclerosis (SSc) and is hypothesized to arise from sites of chronic inflammation and tissue hypoxia1. Calcinosis associated with connective tissue disease has been treated with calcium channel blockers, colchicine, bisphosphonates, warfarin, intravenous Ig, and sodium thiosulfate, albeit with no consistent benefits shown in studies2. Palliative cases have also been treated with CO2 laser3 and shock wave lithotripsy4 with mild symptomatic relief.
An 80-year-old female with Raynaud phenomenon presented with dysphagia resulting in weight loss of 20 pounds over 1 month. Examination revealed a large anterior neck protrusion, extensive calcinosis over both hands, scattered telangiectasias, dilated nailfold capillary loops, and soft skin. Bloodwork showed normal cell counts, creatinine, calcium, phosphate. Antinuclear antibody and rheumatoid factor were negative.
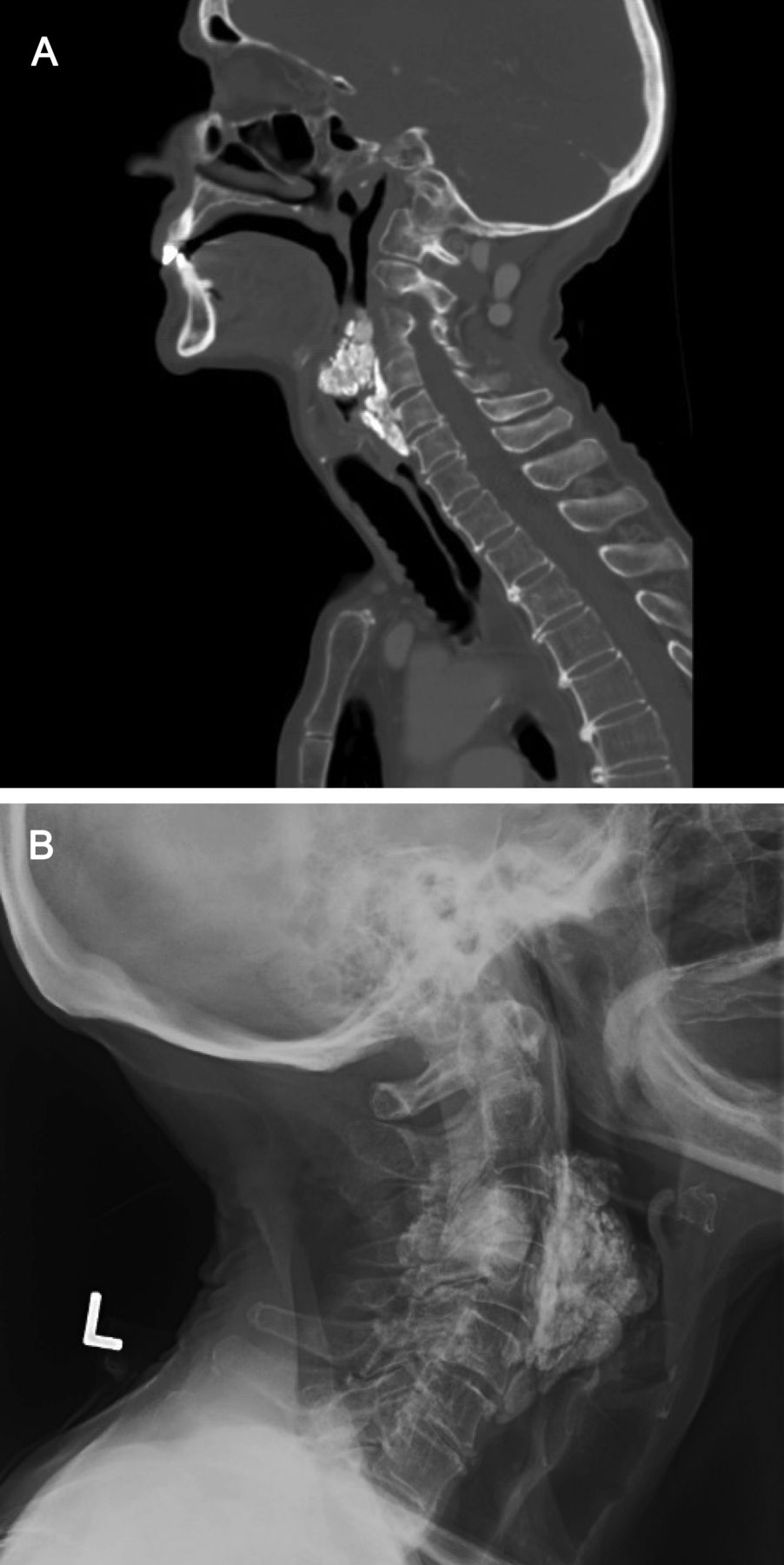
Hand radiographs showed tumoral calcification in both hands and wrists. Computed tomography demonstrated interstitial pneumonitis at both lung bases. In addition, there were multifocal large calcific masses at the C3-4 facet articulation and in the parapharyngeal/retropharyngeal neck spaces compressing the esophagus (Figure 1A); this was also seen on neck radiograph (Figure 1B). Based on her clinical findings and history of never having had sclerodactyly, she was diagnosed with SSc sine scleroderma.

(A) Computed tomography showing multifocal large calcific masses at the C3-4 facet articulation and in the parapharyngeal/retropharyngeal neck spaces compressing the esophagus, which is also seen on (B) neck radiograph.
Ultimately, our patient’s dysphagia was managed with a gastrostomy tube, and calcinosis was treated with amlodipine and colchicine, unfortunately with minimal response. Surgery was not performed due to her comorbidities and patient preference. Although dysmotility is a common cause of dysphagia in SSc, this is, to our knowledge, the first report of esophageal obstruction secondary to massive tumoral calcinosis.
ACKNOWLEDGMENT
The authors would like to sincerely thank Dr. Euan Stubbs, musculoskeletal radiologist at St. Joseph’s Healthcare in Hamilton, Ontario, Canada for supplying the images and for his time and expertise in interpretation.
Footnotes
Written consent has been provided by the patient for her case to be published anonymously. Ethics board approval was not relevant in this work and thus has not been sought.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}