

Abstract
Objective In a large series of White patients with refractory uveitis due to Behçet disease (BD) being treated with infliximab (IFX), we assessed (1) long-term efficacy and safety of IFX, and (2) IFX optimization when ocular remission was achieved.
Methods Our multicenter study of IFX-treated patients with BD uveitis refractory to conventional immunosuppressant agents treated 103 patients/185 affected eyes with IFX as first biologic therapy in the following intervals: 3–5 mg/kg intravenous at 0, 2, 6, and then every 4–8 weeks. The main outcome variables were analyzed at baseline, first week, first month, sixth month, first year, and second year of IFX therapy. After remission, based on a shared decision between patient and clinician, IFX optimization was performed. Efficacy, safety, and cost of IFX therapy were evaluated.
Results In the whole series (n = 103), main outcome variables showed a rapid and maintained improvement, reaching remission in 78 patients after a mean IFX duration of 31.5 months. Serious adverse events were observed in 9 patients: infusion reactions (n = 4), tuberculosis (n = 1), Mycobacterium avium pneumonia (n = 1), severe oral ulcers (n = 1), palmoplantar psoriasis (n = 1), and colon carcinoma (n = 1). In the optimization subanalysis, the comparative study between optimized and nonoptimized groups showed (1) no differences in clinical characteristics at baseline, (2) similar maintained improvement in most ocular outcomes, (3) lower severe adverse events, and (4) lower mean IFX costs in the optimized group (€4826.52 vs €9854.13 per patient/yr).
Conclusion IFX seems to be effective and relatively safe in White patients with refractory BD uveitis. IFX optimization is effective, safe, and cost-effective.
Ocular involvement is one of the most severe manifestations of Behçet disease (BD) and occurs in 35–90% of patients, leading to visual loss in 13–74% of cases1,2,3,4,5. Nevertheless, biologic therapy has improved the ocular prognosis of these patients. Anti–tumor necrosis factor-α (anti-TNF) drugs, especially adalimumab (ADA) and infliximab (IFX), have been the most studied group6. ADA has been approved by the European Medicines Agency (EMA) and the US Food and Drug Administration (FDA) for noninfectious nonanterior uveitis, based on 2 phase III trials (VISUAL I and VISUAL II)7,8. However, the number of patients with BD included in these studies was scarce, with 12 patients (11%) in the VISUAL I study and 10 patients (9%) in the VISUAL II study.
Although IFX has not been approved in the US or Europe for noninfectious uveitis, it has been successfully used for treating uveitis refractory to conventional immunosuppressive therapy9-21. Therefore, according to expert panel recommendations, the efficacy of IFX is supported by high-quality evidence and should be considered in the early management of BD patients with vision-threatening ocular manifestations22. Moreover, in Japan, IFX has been approved for uveoretinitis due to BD, with a dosage of 5 mg/kg at 0, 2, and 6 weeks, then every 8 weeks23,24. In recent years, several retrospective observational studies have been performed with relatively large samples of patients with BD uveitis treated with IFX25,26,27,28,29.
On the other hand, an increased risk of relapse when IFX treatment is withdrawn, even in patients with sustained remission, has been reported29. Further, biologic therapy optimization in systemic diseases has shown a reduction in the number and severity of adverse events and in the cost of treatment30,31. A study on the efficacy and safety of ADA optimization in patients with refractory uveitis secondary to BD has been previously published30. However, to the best of our knowledge, there is no information on IFX therapy optimization in patients with BD and refractory uveitis30,31.
Taking these considerations into account, our aims were to evaluate (1) the long-term efficacy and safety of IFX therapy, and (2) whether optimization therapy can be successfully performed when ocular remission is achieved, in a large series of White patients with BD and refractory uveitis.
MATERIALS AND METHODS
Design, enrollment criteria, and definitions. Our study is part of a broader open-label multicenter study that included 177 White patients with refractory uveitis due to BD who were treated with IFX and ADA as first-line biologic therapy32. IFX was used in 103 patients and ADA in 74. The objectives of this study were (1) to evaluate the long-term efficacy and safety of IFX, and (2) to establish whether IFX optimization is equally effective, safe, and cost-effective. Patient follow-up was conducted at 35 uveitis units from different Spanish hospitals.
BD was diagnosed according to the International Clinical Criteria for BD proposed by the International Study Group in 199033. Anatomical classification of uveitis was performed according to the Standardization of Uveitis Nomenclature (SUN) Working Group34. All patients had uveitis refractory to corticosteroids and had previously received at least 1 conventional synthetic immunosuppressive drug32.
Malignancy or systemic infectious diseases were excluded before anti-TNF onset, as previously described9,10,20,35,36,37,38,39,40.
The conventional immunosuppressive drugs and dosages used before IFX onset were as follows: cyclosporine A (CSA; 3–6 mg/kg/day oral), methotrexate (MTX; 7.5–25 mg/week oral or subcutaneous [SC]) azathioprine (AZA; 100–150 mg/day oral) and mycophenolate mofetil (2–3 g/day oral). The therapeutic schedule included 3 consecutive pulses of methylprednisolone (MP), 500–1000 mg/day, in cases of severe uveitis.
IFX was administered as follows: a loading intravenous (IV) dose of 3–5 mg/kg at weeks 0, 2, and 6, and then a maintenance dose every 4–8 weeks until remission was achieved. Remission was established if there were no signs of intraocular inflammation for at least 3 months. Relapses were defined as the occurrence of a new flare of uveitis in a patient who had reached remission41.
Based on a shared decision between the patient and the physician, IFX was optimized once ocular remission was achieved. Only those patients with an initial standard maintenance dose of 5 mg/kg every 8 weeks were selected for the subanalysis of IFX optimization. Optimization was performed by prolonging IFX dosing interval and/or reducing IFX dose. The nonoptimized group included those patients with BD uveitis who reached remission after IFX therapy with the dose and interval remaining unchanged.
Before IFX onset, all patients signed written informed consent, since prescription of IFX was based on an off-label indication by the EMA for the treatment of noninfectious and nonanterior uveitis. In addition, the approval of the corresponding ethics committee was obtained (2018.081).
Outcome variables. To determine efficacy, the intraocular inflammation, macular thickness, visual acuity, sparing effect of glucocorticoids (GC), and total immunosuppression load were assessed. These variables were recorded at baseline (IFX onset), first week, second week, first month, third month, sixth month, first year, and second year, consecutively. Intraocular inflammation included the following features: anterior or posterior chamber inflammation, vitritis, retinal vasculitis, papillitis, and macular thickness. The degree of intraocular inflammation was evaluated according to the SUN Working Group criteria34. Vitritis was assessed by the Nussenblatt scale41.
Fluorescein angiography (FA) was performed to assess the presence of retinal vasculitis. Retinal vasculitis was defined as retinal angiographic leakage, staining, and/or occlusion on FA5.
To assess the macular thickness, high-definition optical coherence tomography (OCT) was performed using a Cirrus HD-OCT (Carl Zeiss). Scans were obtained using the 512 × 128 scan pattern. Macular thickening was defined as a macular thickness > 250 μm.
The best-corrected visual acuity (BCVA) was estimated using the Snellen chart.
Immunosuppression degree was calculated according to the semiquantitative scale proposed by Nussenblatt, et al42. The grading scheme provided a combined, single numeric score for the total immunosuppression load per unit of body weight and per day. Grades for each agent (i.e., prednisone, cyclosporine, AZA, methotrexate, and chlorambucil) ranged on a scale from 0–9, whereas mycophenolate mofetil ranged from 0–7. For patients receiving multiple medications, the sum of the grading score for each drug was used to calculate the total immunosuppression score on a scale of 0–15.
Statistical analysis. Results were expressed as mean ± SD or as median and IQR, as appropriate. Normality of data was assessed by the Kolmogorov-Smirnov test. Continuous variables were compared with the 2-tailed t-test or the Mann-Whitney U test. Chi-square, Fisher exact, and McNemar tests were used to compare dichotomous variables, and Wilcoxon signed-rank test was used to compare continuous variables before and after IFX therapy.
Variables assessed and compared with baseline, and evaluated at first week, first month, third month, sixth month, first year, and second year, were the following: BCVA, anterior chamber (AC) cell count, vitritis, vasculitis, OCT, and GC sparing effect. Additionally, the same variables were analyzed and compared at baseline, at the time of optimization, and at the last visit, separately in each group (i.e., optimized and nonoptimized patients). The probability of improvement of ocular variables and the occurrence of adverse events during the study period were compared using unadjusted Kaplan-Meier survival analysis and log-rank tests. To adjust for the possible within-eye and between-eye correlation, we used a repeated measures general linear model (variables were log-transformed before analysis). Bonferroni procedure was carried out to test for multiple comparisons. Statistical significance was considered as a P < 0.05 in all the calculations. Statistica software (StatSoft) was used for data processing.
RESULTS
Demographic and clinical features at baseline. Out of a series of 177 White patients with refractory uveitis due to BD, IFX was used as the first biologic agent in 103 (55 male, 48 female) patients. The mean age was 40.4 ± 10.1 years. The median duration of uveitis before IFX onset was 36 (12–72) months. In most cases, uveitis was bilateral (79.6%). The main demographic and clinical data for the whole series have been previously published32 and are summarized in Table 1.
Main general features and long-term follow-up of a series of 103 patients with refractory uveitis due to Behçet disease (BD) treated with IFX.
Besides oral GC (mean maximum prednisone daily dosage: 54.4 ± 15.8 mg/d) and before the onset of biologic therapy, patients had received the following immunosuppressive agents: CSA in 77 patients (4.9 ± 0.8 mg/kg/d), AZA in 58 patients (137.2 ± 32.3 mg/d), MTX in 45 patients (16.7 ± 3.6 mg/wk), and IV pulses of MP in 30 patients (Table 1). The immunosuppression load score was 9.1 ± 4.1.
Efficacy of IFX therapy. The main outcome variables assessed in our study (intraocular inflammation, macular thickness, and BCVA) showed rapid and maintained improvements throughout the study (Figure 1).

Rapid and maintained improvement following the onset of TNF-α IFX. (A) BCVA; (B) macular thickness (OCT); (C) retinal vasculitis (% affected eyes); (D) percentage of patients with improvement on anterior chamber cells and vitritis according to SUN Working Group criteria; (E) glucocorticoid-sparing effect following IFX therapy (mg/day). AC: anterior chamber; BCVA: best-corrected visual acuity; IFX: infliximab; OCT: optical coherence tomography; SUN: Standardization of Uveitis Nomenclature; TNF-α: tumor necrosis factor-alpha.
A statistically significant improvement was observed in all the variables analyzed since the first week. The mean BCVA increased from a mean value of 0.44 ± 0.28 before the onset of biologic therapy to 0.63 ± 0.28 at second year (P < 0.0001). At the same time, all patients had a progressive improvement in intraocular inflammation. The percentage of eyes with improvement in AC cell count according to the SUN Working Group criteria was increased to 80.4% at 2-year follow-up. With respect to eyes with vitritis, an improvement was seen in 84.4% at the second year. A significant decrease in the percentage of eyes with retinal vasculitis (58% at baseline vs 2% at 2-yr follow-up) was also observed. In addition, OCT mean value (μ) decreased from 337.7 ± 121.8 at the onset of IFX therapy to 267.8 ± 52.9 at second year (P = 0.006; Figure 1).
The immunosuppression load score was also reduced by almost half (from 9.1 ± 4.1 to 4.8 ± 3.5 at 2-yr follow-up) 1 year after starting IFX. Further, the daily median dose of prednisone was reduced from 30 (20–45) mg/day at baseline to 1.25 (0–5) mg/day at 2-year follow-up (Figure 1).
Follow-up and safety of IFX therapy. After a mean follow-up period of 31.5 ± 23.5 months, 78 patients (76.5%) achieved ocular remission. IFX was withdrawn in 57 (55.3%) patients, with 20 due to maintained remission and in the remaining 37 because of inefficacy (n = 18), preference of change to SC administration (n = 9), toxicity/side effects (n = 9), and pregnancy (n = 1). In 34 of the 37 patients in whom IFX was withdrawn, the switch was made from IFX to ADA in 32 cases (18 because of treatment failure, preference of subcutaneous administration in 9, and in the remaining 5 because of toxicity/side effects), to rituximab (RTX) in 1 case due to side effects, and to etanercept (ETN) in another patient due to side effects (Table 1). Additionally, further switching to golimumab (n = 1) and RTX (n = 1) was necessary for 2 patients due to ADA inefficacy.
Severe complications leading to discontinuation of IFX therapy were observed in 9 patients and included the following: infusion reactions (n = 4), tuberculosis (n = 1), Mycobacterium avium pneumonia (n = 1), severe oral ulcers (n = 1), palmoplantar psoriasis (n = 1), and colon carcinoma (n = 1; Table 1).
IFX optimization: subanalysis of efficacy, side effects, and cost. Ocular remission was achieved in 78 of the 103 IFX-treated patients (76.5%) after a mean of 31.5 ± 23.5 months of therapy (Table 1). A subanalysis was performed in a group of 60 patients who achieved ocular remission with the standard dose of 5 mg/kg at weeks 0, 2, 6, and then every 8 weeks (standard dose). The dose was optimized in 18 patients (optimized group) while in the remaining 42, the dose of 5 mg/kg every 8 weeks was maintained until the end of the follow-up period (nonoptimized group).
Optimized patients did not show significant demographic or clinical differences at IFX onset when compared with the nonoptimized group. Ocular features at IFX onset were similar in both groups, as well as previous use of conventional immunosuppressants, number of patients receiving oral GC or MP pulses, and mean dose of prednisone (Table 2).
Main general features and follow-up of a subgroup of patients (n = 60) with refractory uveitis due to Behçet disease (BD) who achieved remission after the standard dose of IFX therapy (5 mg/kg at 0, 2, 6 wks, then every 8 wks); differences between optimized and nonoptimized patients.
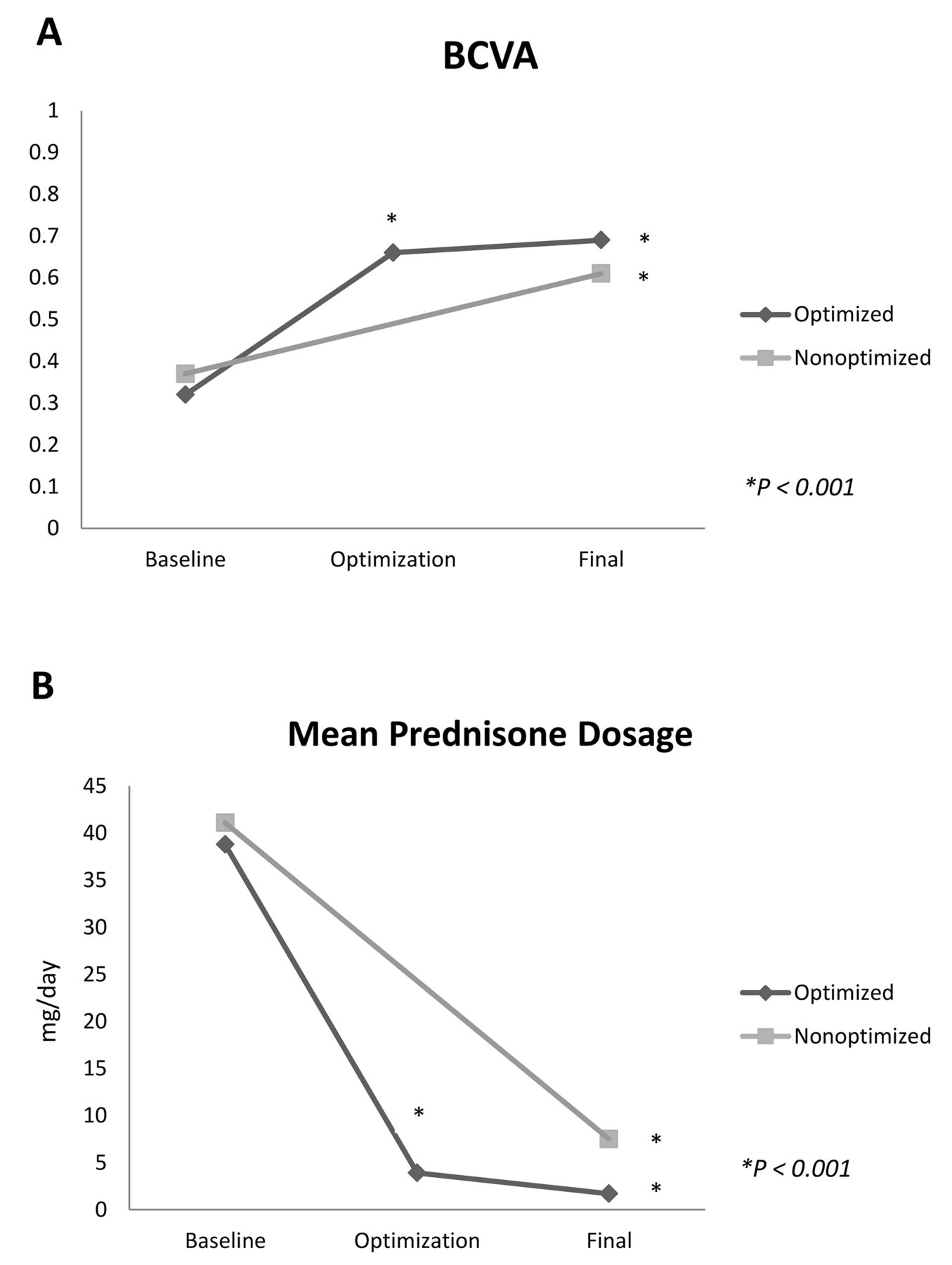
Following IFX onset, the intraocular inflammation, macular thickness, visual acuity, and the sparing effect of GC was assessed in both groups. In the optimized group, the BCVA increased progressively from baseline to the time of IFX optimization (0.33 ± 0.21 vs 0.68 ± 0.28; P < 0.0001). This improvement was maintained at the last visit when compared with baseline values (0.70 ± 0.29; P < 0.001; Figure 2A). Also in the optimized group, mean OCT (μm) decreased from 303.5 ± 23.3 (IFX onset) to 276.5 ± 34.6 (last visit; P = 0.18; data not shown).

Rapid and maintained improvement following the onset of IFX regardless of further optimization. No significant differences between optimized and nonoptimized patients were seen. (A) Mean BCVA; (B) successful glucocorticoid-sparing effect following the onset of IFX therapy. P values for panels A and B show the differences between baseline findings and those observed at each period of time, including the time of optimization and the last visit. The assessment was performed in optimized and nonoptimized patients. BCVA: best-corrected visual acuity; IFX: infliximab.
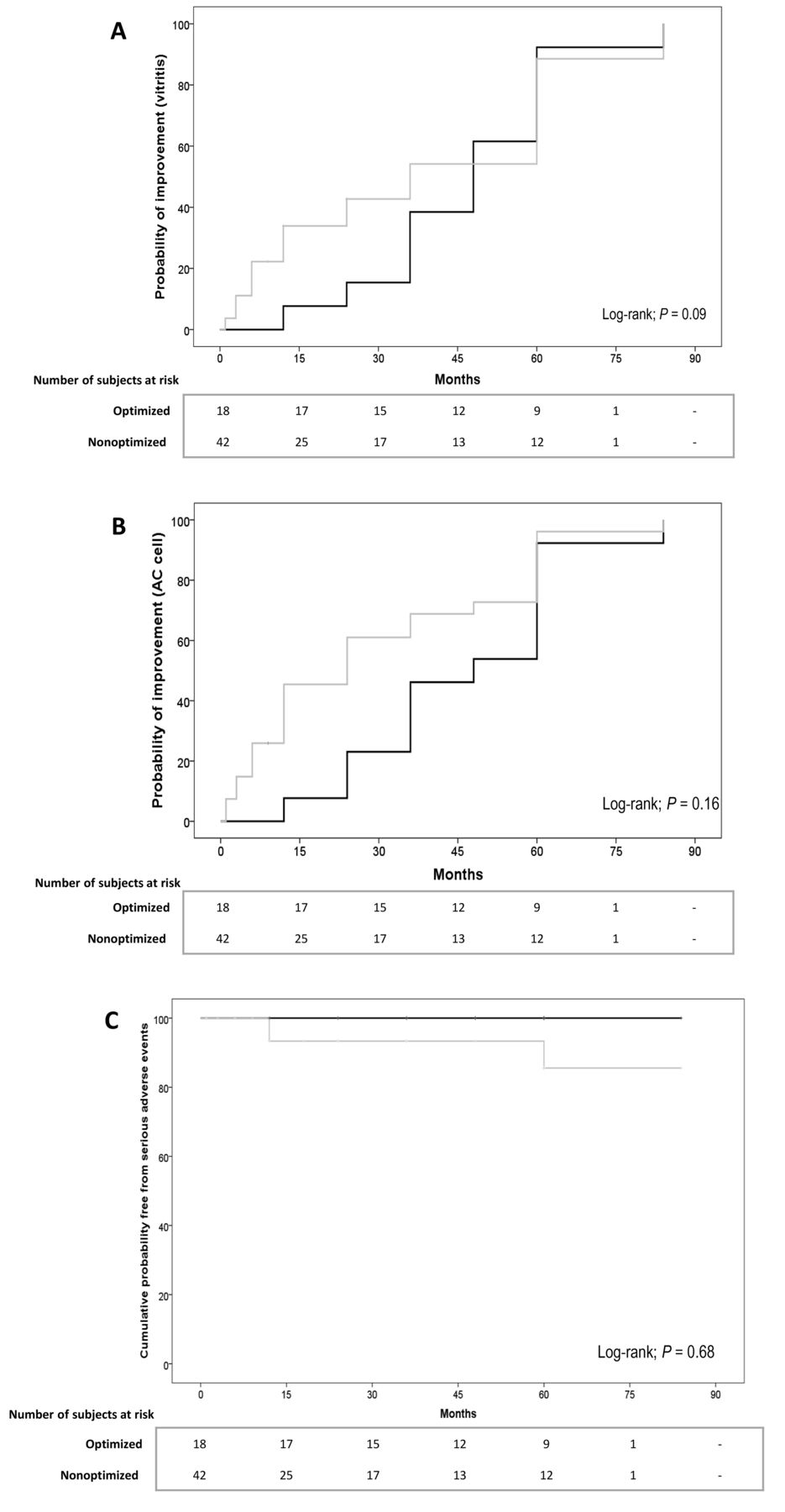
Improvement of intraocular inflammation also persisted with optimization. Thus, the percentage of eyes with an improvement in AC cells and vitritis (according to the SUN criteria) increased from 50% and 45.5% (IFX onset), respectively, to 100% for both between the time of optimization and at the last follow-up visit. A significant decrease in the percentage of patients with retinal vasculitis (44.4% at baseline, 0% at time of optimization, and 0% at final visit) was also observed. Improvement in all ocular variables was also observed in the nonoptimized group. Because of this, most ocular outcomes were similar in the optimized and nonoptimized groups after a mean follow-up period of 46.6 ± 18.4 and 27.9 ± 24.8 months since the onset of IFX therapy in optimized and nonoptimized patients, respectively. Using the data for the last observation carried forward (LOCF) in the follow-up period in both groups, the percentages were as follows: AC cell improvement in 18/18 vs 39/42 patients (100% vs 96.3%; P = 0.99); vitritis improvement in 18/18 vs 31/42 patients (100% vs 74.1%; P = 0.07); and retinal vasculitis (absence) in 18/18 vs 42/42 patients (100% vs 100%). Kaplan-Meier curves for both groups regarding the probability of improvement in AC cells and vitritis and the corresponding results of the log-rank tests are shown in Figures 3A and 3B.

Kaplan-Meier curves showing the probability of AC cells improvement (A); the probability of vitritis improvement (B); and the cumulative probability of being free from serious adverse events (C) in optimized (black lines) and nonoptimized (gray lines) patients. AC: anterior chamber.
Regarding the optimized group, the dose schedule and maintenance intervals of IFX were as follows: 3 mg/kg every 8 weeks (n = 2), 3 mg/kg every 10 weeks (n = 4), 5 mg/kg every 10 weeks (n = 6) and 5 mg/kg every 12 weeks (n = 6). In 6 patients, IFX was successfully withdrawn. The immunosuppressive load in optimized vs nonoptimized patients at LOCF in the follow-up was 11 (8.0–14.0) vs 8 (5.8–12.3; P = 0.06; data not shown).
We also observed a sparing GC effect in both groups. Dosage at LOCF in optimized vs nonoptimized patients was 5 mg/d (0.0–8.8) vs 2.5 mg/d (0.0–5.0; P = 0.57; Figure 2B).
We found no statistically significant differences in the outcome variables (baseline vs final values), between optimized and nonoptimized patients, when repeated measures general linear models were built and adjusted by age, sex, and duration of BD, in previous use of AZA, or in the presence of vitritis at baseline. Concerning BCVA, P value was 0.36 (P for interaction = 0.20). The corresponding figure for prednisone dosage was P = 0.17 (P for interaction = 0.63).
Moreover, when we analyzed the number of relapses, we observed that both groups had very similar medians (0 [0–1] in optimized and 0 [0–2] in nonoptimized patients), without statistically significant differences between them (P = 0.85; Table 2).
No serious adverse events (SAE) were observed in the optimized group, but they were found in 3 patients (7.1%) from the nonoptimized group (P = 0.55), all being infusion skin reactions (Table 2). For this reason, IFX was permanently withdrawn in these patients. Figure 3C shows the Kaplan-Meier analysis concerning the cumulative probability of being free from SAE in optimized and nonoptimized patients.
Finally, the mean IFX treatment costs were much lower in the optimized group than in the nonoptimized group (€4826.52 vs €9854.13 per patient/yr), achieving an overall annual cost reduction of 51%.
DISCUSSION
To the best of our knowledge, our multicenter study represents the largest series of White patients with refractory uveitis due to BD undergoing IFX therapy. This therapy seems to be effective and relatively safe, both short- and long-term. After remission, IFX optimization, a therapeutic scheme of similar efficacy but safer and less expensive, was successfully performed in 18 (30%) out of 60 patients.
Although the incidence of ocular sequelae due to uveitis in patients with BD has decreased, it still remains unacceptably high3,5,43. Therefore, different targeted therapies have been studied, with high-serum TNF-α in aqueous humor of patients with uveitis, including those with BD-related uveitis, being reported44,45.
IFX is a human/mouse chimeric monoclonal IgG1 anti-TNF antibody widely used in immune-mediated diseases, including uveitis; however, randomized phase III studies with IFX in uveitis have not yet been published. Nevertheless, in patients with severe uveitis related to BD, IFX has demonstrated efficacy in observational studies9,11,25,26,27,28,46.
In our present study, we describe one of the largest series of patients with uveitis due to BD refractory to conventional immunosuppressive drugs undergoing IFX therapy in a real-world setting, and the largest series in a White population. All patients had received high doses of GC and at least 1 conventional synthetic immunosuppressive agent before biologic therapy was started. In all patients, IFX was prescribed because of poor control of ocular inflammation with conventional therapy. IFX was effective in most cases, with a statistically significant rapid and maintained improvement of all ocular parameters during a 2-year follow-up. In addition, we observed a GC-sparing effect, showing a significant decrease in the median oral prednisone dose from 30 mg/day at IFX onset to 5 mg/day after 2 years of therapy. In the last 3 years, several studies reported by Fabiani, et al support our results, with high drug retention rates, remarkable GC-sparing effect, and very similar long-term efficacy and safety data25,26,27,28.
IFX therapy was discontinued in 20 patients after reaching a sustained remission, which is similar to data published by several authors47,48. However, IFX was withdrawn in 18 (17.5%) patients due to inefficacy. Whether this fact could be related to the development of long-term antidrug antibodies remains speculative, since we did not perform such tests.
In our present study, the number of patients on IFX who experienced SAE at 2 years was lower than in other series11 and most of them were mild infusion reactions. Nevertheless, SAE leading to discontinuation of the biologic treatment was observed in 1 patient who had a reactivation of latent tuberculosis, as described in several studies with other anti-TNF drugs49. The incidence of neoplasms in patients with biological treatment still remains a controversial issue. Nevertheless, a previous metaanalysis did not demonstrate an increased risk of cancer in rheumatoid arthritis patients treated with anti-TNF agents compared to placebo50. In our series, 1 patient developed a colon carcinoma, but we cannot establish that the tumor was related to IFX therapy.
Optimization of long-term biologic therapy in patients who achieve remission is of great relevance in terms of efficacy, side-effect reduction, and cost. Several studies have shown that intensive outpatient strategies involving tight control and frequent monitoring of disease activity, as well as treatment adjustments to meet therapeutic goals, can produce better outcomes than traditional strategies. We previously reported the successful optimization of ADA treatment in 23 patients with refractory uveitis secondary to BD who had achieved clinical remission, reducing both costs and adverse events30.
In our present study, both optimized and nonoptimized patients presented a maintained improvement in the analyzed ocular variables. Moreover, a lower frequency of severe side effects without an increase in the number of relapses was observed in optimized group. In Spain, IFX cost (100 mg/20 mL vial) for a standard weight of 70 kg is around €1408. Therefore, optimization after remission yielded a significant reduction in the mean cost of IFX per patient per year.
Up to 50% of patients with uveitis due to BD may have relapses when abruptly discontinuing biologic treatment once remission is achieved27. Therefore, IFX optimization has been performed slowly by progressive prolongation of dosing interval and decreasing the dose sequentially.
Based on our experience, we propose a protocol for IFX optimization in patients with refractory uveitis secondary to BD who achieve remission. After 12 months of treatment with IFX and once remission has been reached and sustained for at least 3–6 months, we recommend either of the following 2 alternatives: extending very slowly, but progressively, the dosing intervals with regular monitoring of ocular inflammation variables, or reducing the dosage to 3 mg/kg every 8 weeks, and then progressively increasing the dosing interval with tight ocular control. Once the dosing interval has been increased to up to every 12 weeks, and there is no ocular inflammation data, we recommend discontinuing treatment but keeping close monitoring. If relapse occurs, the patient should be restarted with the standard dose of 5 mg/kg every 8 weeks (Figure 4).
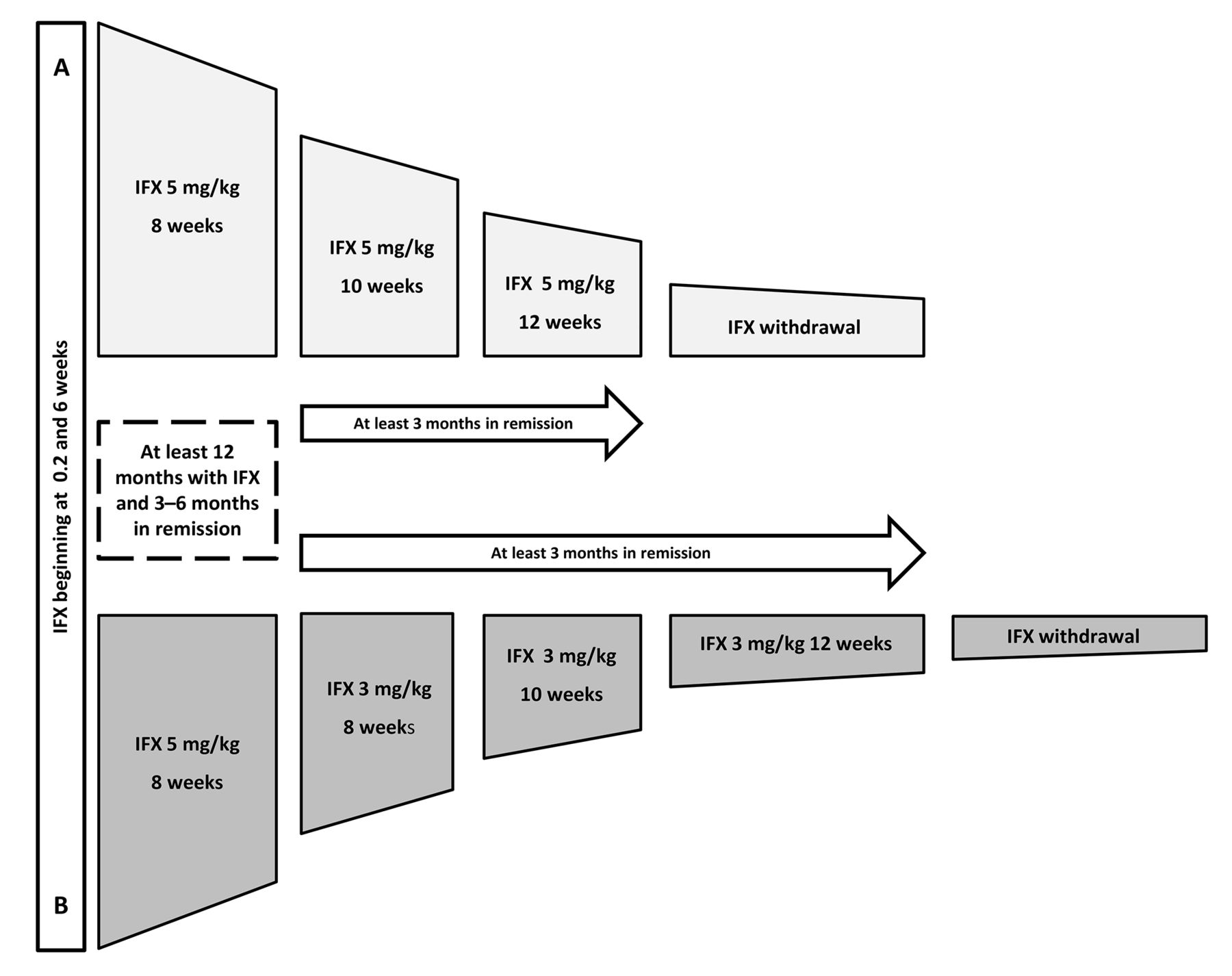
A proposed protocol for optimization of IFX dose up to withdrawal by (A) extending the dosing interval progressively (upper), or (B) reducing the dose and prolonging the dosing interval (lower). IFX: infliximab.
Our study has several limitations due to its observational nature and the relatively low number of optimized patients. Because of this, further randomized controlled trials comparing conventional immunosuppressive drugs and other anti-TNF agents are required. However, it is difficult to carry out such a clinical trial with these specific diseases, and even more so since the entry of biosimilars into the market. Therefore, future information will likely be obtained from observational multicenter studies such as ours.
In conclusion, our results suggest that IFX seems to be effective and relatively safe, both short- and long-term, in White patients with refractory BD uveitis. IFX optimization could be a feasible, safer, and more cost-effective option than conventional IFX therapy.
APPENDIX
Biological Therapy in Refractory Uveitis Due to Behçet’s Disease Collaborative Group. Marina Mesquida, MD, PhD, María V. Hernández, MD, Francisco J. López-Longo, MD, PhD, Lucía Martínez Costa, MD, PhD, José L. García-Serrano, MD, PhD, José L. Callejas-Rubio, MD, PhD, José M. Herreras, MD, PhD, Alejandro Fonollosa, MD, PhD, Ana Blanco, MD, Esperanza Pato, MD, Susana Romero Yuste, MD, PhD, José C. Fernández Cid, MD, Miriam García-Arias, MD, Antonio Atanes, MD, PhD, Félix Francisco, MD, Santos Insúa, MD, Senén González-Suárez, MD, Amalia Sánchez-Andrade, MD, PhD, Luis Linares, MD, PhD, Fredeswinda Romero Bueno, MD, PhD, Raquel Almodóvar, MD, Enrique Mínguez, MD, PhD, Carmen Carrasco Cubero, MD, María Alcalde Villar, MD, Cristina Fernández-Carballido, MD, PhD, and Fred A. Pagés, MD.
Footnotes
J.L. Martín-Varillas, B. Atienza-Mateo, and V. Calvo-Río shared first authorship. J.L. Hernández, M.A. González-Gay, and R. Blanco shared senior authorship.
This study was presented in part at the 2017 American College of Rheumatology Congress held in San Diego, California, and at the 2018 American College of Rheumatology Congress held in Chicago, Illinois, USA. This work was also partially supported by RETICS Programs, RD08/0075 (RIER) and RD12/0009/0013 from Instituto de Salud Carlos III (ISCIII; Spain).
JMV received grants/research supports from AbbVie, Pfizer and Celgene. BAM received grants/research supports from Roche, Celgene, and GSK. VCR received grants/research supports from MSD and Roche and had consultation fees/participation in the company-sponsored speaker’s bureaus from AbbVie, Lilly, Celgene, Grünenthal, and UCB Pharma. JSB received grants from Lilly and Janssen and had fees/participation in company-sponsored speaker’s bureaus from Pfizer. AA received grants/research supports from AbbVie and had consultation fees/participation in company-sponsored speaker’s bureaus from AbbVie. EVP received grants/research supports from Roche, Novartis, and AbbVie, and had consultation fees/participation in company-sponsored speaker’s bureaus from AbbVie, Lilly, Pfizer, MSD, Novartis, Janssen, Bristol Myers Squibb, UCB Pharma. ASF received consultation fees/participation in company-sponsored speaker’s bureaus from Abbott, Lilly, Celgene, Pfizer, Schering-Plough, Janssen, Novartis, and Nordic Pharma. VJ received grants/research supports from AbbVie, MSD, Novartis, and Pfizer and had consultation fees/participation in company-sponsored speaker’s bureaus from AbbVie. DP received grants/research supports from AbbVie, Lilly, MSD, and Roche, and had participated in a company-sponsored speaker’s bureaus from AbbVie, Roche, and MSD. DDV received lecture fees from MSD and AbbVie. MAC received grants fees/participation in company-sponsored speaker’s bureaus from Lilly, Sanofi-Genzyme, and Amgen. ERÁ received grants/research supports from MSD and had consultation fees/participation in company speaker’s bureaus from Lilly. NVR received grants/research support from AbbVie, Roche, Pfizer, Lilly, Gebro Pharma, MSD, Novartis, Bristol Myers Squibb, Janssen, and Celgene. MAGG received grants/research supports from AbbVie, MSD, and Roche, and had consultation fees/participation in company-sponsored speaker’s bureaus from AbbVie, Pfizer, Roche, Sanofi, and MSD. RB received grants/research supports from AbbVie, MSD, and Roche, and had consultation fees/participation in company-sponsored speaker’s bureaus from AbbVie, Pfizer, Roche, Bristol Myers Squibb, Janssen, and MSD. The following authors did not declare financial disclosure: EB, MHG, NO, OM, IT, CFE, EA, RDP, SC, and JLH.
- Accepted for publication August 18, 2020.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}
{kind=link}
{kind=link}
{kind=link}