

Abstract
Objective This study evaluated associations between fibroblast growth factor (FGF)-21, an adipokine associated with metabolic stress, and adverse longitudinal changes in body composition and physical functioning in patients with rheumatoid arthritis (RA).
Methods At baseline and follow-up, patients with RA aged 18–70 years completed whole-body dual-energy X-ray absorptiometry and peripheral quantitative computed tomography to quantify lean mass, fat mass, and muscle density. Dynamometry assessed muscle strength at the hand and knee, and physical functioning was measured with the Health Assessment Questionnaire (HAQ) and the Short Physical Performance Battery (SPPB). FGF-21 and inflammatory cytokines were measured at baseline. Linear and logistic regression analyses assessed associations between FGF-21 levels and both body composition and physical functioning over time.
Results There were 113 patients with RA enrolled, and 84 (74%) returned for follow-up at a median of 2.68 years. At baseline, FGF-21 was associated with age, smoking, methotrexate use, adiposity, and inflammatory cytokines: tumor necrosis factor receptor type I, YKL-40, vascular endothelial growth factor (VEGF), and resistin. The highest FGF-21 quartile was associated with worse SPPB and HAQ. Higher baseline FGF-21 levels (per 1 SD) were associated with worsening in muscle density and area Z-scores (β –0.06, 95% CI –0.12 to 0.008, P = 0.08; and β –0.05, 95% CI –0.10 to 0.006, P = 0.08, respectively) and a greater probability of a clinically meaningful worsening of HAQ (OR 2.37, 95% CI 1.21–4.64, P = 0.01). The fourth FGF-21 quartile was associated with worsening of SPPB (β –0.57, 95% CI –1.04 to –0.09, P = 0.02).
Conclusion FGF-21 levels are associated with obesity and inflammatory cytokines, and with worsening in physical functioning in RA. These data support the hypothesis that FGF-21 can identify patients at risk of functional decline.
- biomarkers
- body composition
- disease activity
- fibroblast growth factor 21
- physical functioning
- rheumatoid arthritis
Rheumatoid arthritis (RA) can lead to changes in body composition, including muscle loss and excess adiposity1,2, which are in turn associated with physical disability3,4,5. Given this link between body composition and long-term outcomes in RA, it is of interest to identify biomarkers that could help identify patients most at risk for developing progressive deficits in the skeletal muscle and the ensuing loss of physical functioning.
Fibroblast growth factor-21 (FGF-21) is an adipokine in the FGF family that acts as an endocrine hormone and metabolic regulator. Although the exact targets of FGF-21 are still not well understood, there is evidence that FGF-21 plays an important role in the body’s metabolic stress response. This role encompasses an array of physiologic responses to a diverse number of conditions that change the body’s metabolic demands, including fasting, malnutrition, obesity, amino acid deprivation, mitochondrial diseases, and exercise, among many others6,7. Indeed, FGF-21 levels are elevated in many of these physiologic states, including starvation, obesity, metabolic syndrome, insulin resistance, and exercise8–15; they are also associated with age and are elevated in patients with endstage renal disease, heart disease, fatty liver disease, and cachexia16,17,18. Further, FGF-21 is constitutively produced by the skeletal muscles in times of stress, and high circulating FGF-21 levels have been associated with muscle stress conditions and mitochondrial disease19. Given this link between FGF-21 and metabolic changes as well as muscle stress, FGF-21 could be a potential marker of inflammatory processes that leads to functional deficits in patients with RA.
However, few studies have evaluated FGF-21 levels in patients with RA. One study found elevated FGF-21 levels in seropositive RA patients, but no correlations with measures of disease severity20. Other studies have demonstrated that in mouse models of RA, exogenous FGF-21 may have a therapeutic effect21,22. However, evidence is limited, and the role of FGF-21 in RA is not clear. In order to address this knowledge gap, we conducted an analysis of a cohort of RA patients with comprehensive clinical data collected at 2 timepoints over 2–3 years of follow-up. We hypothesized that levels of FGF-21 at baseline would be associated with worsening muscle deficits (as measured through muscle density/area and muscle strength) and physical functioning outcomes over time.
MATERIALS AND METHODS
Study setting. The data collection methods for this study have been previously described23. Briefly, RA subjects aged 18–70 years, with established disease and meeting 2010 American College of Rheumatology classification criteria, were recruited from the University of Pennsylvania and Philadelphia Veterans Affairs Medical Center (VAMC) rheumatology practices24. Subjects with juvenile idiopathic arthritis (or another inflammatory arthritis), active cancer, a history of chronic diseases known to affect bone health, pregnancy, or who were unable to perform the muscle density or body composition assessments were excluded. The original pilot study was expanded to include a follow-up visit occurring 2–3 years later for most participants; 84 patients completed the study. The data collection procedures described below were conducted at both the initial visit and follow-up. The protocols were approved by the institutional review board (IRB) at University of Pennsylvania and the Philadelphia VAMC (approval number 01427 from the Corporal Michael J. Crescenz VAMC IRB), and informed consent was obtained from all participants.
Assessment of anthropometrics, race, and medical history. Weight and height were measured in light clothing and with shoes removed using a digital scale (Scaltronix) and stadiometer (Holtain Ltd.), respectively. BMI was calculated (kg/m2). Participants self-reported race (according to National Institute of Health categories), smoking status, and comorbidities (cardiac disease and diabetes). Comorbidities were confirmed in the medical record.
Whole-body dual-energy X-ray absorptiometry. Subjects underwent whole-body dual-energy X-ray absorptiometry (DXA) assessment using a Hologic densitometer (Delphi/Discovery Systems, Hologic, Inc.) to measure appendicular lean mass, total fat mass, and visceral adipose tissue area (VAT). Similar to the adjustment of weight for height to estimate BMI, body composition estimates were adjusted for height2 to generate appendicular lean mass index (ALMI; kg/m2) and fat mass index (FMI; kg/m2). Measurement of VAT by DXA has been previously validated25.
Peripheral quantitative computed tomography. Muscle density and muscle area measurements in the left lower leg were obtained by peripheral quantitative computed tomography (pQCT; Stratec XCT2000 12-detector unit, Orthometrix, Inc.) with a voxel size of 0.4 mm, slice thickness of 2.3 mm, and scan speed of 25 mm/s. All scans were analyzed with Stratec software version 6.00. Calf muscle and subcutaneous fat cross-sectional area (mm2) were assessed 66% proximal to the distal physis using threshold 40 mg/cm3 for fat/lean separation and 711 mg/cm3 for lean/bone separation. The pQCT measure of muscle density (mg/cm3) was used as a composite index of intra- and extramyocellular fat content, as previously described26,27. Edge-detection and threshold techniques were used to separate tissues (fat, muscle, and bone) based on attenuation characteristics that are directly related to tissue composition and density28,29. Images were filtered prior to being analyzed, using contour mode 3 (−101 mg/cm3) to find skin, and peel mode 2 (40 mg/cm3) to separate adipose and muscle/bone. Images were filtered subsequently with a combination 3 × 3, and double 5 × 5 kernel image filter that clearly defined the edge of the muscle using contour mode 31 (40 mg/cm3). All bone was identified using a threshold of 150 mg/cm3 and mathematically removed to generate results for muscle density. In our laboratory, the coefficient of variation (CV) for short-term precision has ranged from 0.5% to 1.6% for pQCT outcomes.
Dynamometric measurement of muscle strength. Muscle strength was assessed in several ways using the Biodex Multi-Joint System 3 Pro Dynamometer (Biodex Medical Systems Inc.). Peak isokinetic torque (ft-lbs) was measured in triplicate at the knee and lower leg (ankle). For lower leg (ankle) Biodex, we reported strength as peak isometric torque (ft-lbs) in dorsiflexion (with the foot placed in 20º plantarflexion) as previously described30. Peak isometric torque in flexion and extension at the knee was also reported (ft-lbs). Hand-grip strength (kg) was measured using a hand-grip dynamometer (Takei Scientific Instruments Co., Ltd.). A clinically important decrease in hand grip strength has been previously defined as 6.5 kg, and a clinically meaningful change in leg extensor power in older adults has been defined as 9–10%31,32.
Assessments of physical function and disability. Disability was assessed using the Health Assessment Questionnaire (HAQ), a widely used tool in RA. Briefly, 8 categories are assessed, including dressing and grooming, arising, eating, walking, hygiene, reach, and grip33. The survey also includes questions about work status, symptoms, and overall health status. Physical function was assessed using the Short Physical Performance Battery (SPPB), a simple test to measure lower extremity function using tasks that mimic daily activities. It examines static balance, gait speed, and timed chair rises34. SPPB testing was initiated later and was therefore measured in a smaller sample of participants (n = 69). Clinically important changes in HAQ and SPPB have been previously defined35,36. Based on these prior data, this study defined an important worsening of HAQ as an increase of 0.2 and an important worsening of SPPB as a decrease of 1.
Disease measures, inflammatory markers, and medical history. Medication use was determined by self-report and confirmed in the medical record. Erythrocyte sedimentation rate (ESR) was performed using the Westergren method. C-reactive protein (CRP) levels were measured using a Fixed Point Immuno Rate Assay. Creatinine was measured in the clinical laboratory, and estimated glomerular filtration rate (eGFR) was determined using the Modification of Diet in Renal Disease Study equation. Disease activity was quantified using the Disease Activity Score in 28 joints based on CRP (DAS28-CRP) and the modified DAS28 (M-DAS28)37. The M-DAS28 is a composite measure that includes the CRP, swollen joint count, and evaluator global score, and has been validated to correlate strongly with synovitis on magnetic resonance imaging (MRI) and radiographic damage progression. It was included to avoid bias related to incorporation of the patient global score in the DAS28-CRP, which is closely correlated with physical functioning scores (HAQ). Commercially available ELISAs (R&D Systems) were used to measure FGF-21 (CV = 2.4–3.4%) and adiponectin (CV = 3–5%). A V-Plex Plus Proinflammatory Panel 1 kit (Meso Scale Discovery) was used to measure tumor necrosis factor (TNF), interleukin 1 (IL-1), IL-6, and interferon-γ (IFN-γ). A multibiomarker disease activity (MBDA) test (Vectra DA; Crescendo Bioscience) was used to measure levels of 12 serum markers: vascular cell adhesion molecule I (VCAM-I), epidermal growth factor (EGF), vascular endothelial growth factor (VEGF), IL-6, TNF receptor type I (TNF-RI), matrix metalloproteinase 1 (MMP-1), MMP-3, bone glycoprotein 39 (YKL-40), leptin, resistin, serum amyloid A (SAA), and CRP. The MBDA score, a validated test of RA activity, was also analyzed38,39. IL-6 was measured in both the Meso Scale Discovery kit and the MBDA test. The primary analysis used the value from the MBDA test (results were similar for both). Cytokine assays were run on serum samples stored at –80ºC that had never been previously thawed. Radiographs of the hands and feet were performed, and Sharp/van der Heijde (SvdH) scores were determined by a trained radiologist (EGT).
Statistical analysis. Measures of muscle density and muscle area were converted to age-, sex-, and race-specific Z-scores based on distributions among a reference population, as has been previously described2,5,40,41. Z-scores represent the number of SD above or below the predicted value for a healthy control of the same age, sex, and race. Body composition (ALMI and FMI) measures were converted to Z-scores relative to a national reference population (National Health and Nutrition Examination Survey).
FGF-21 levels at baseline were first log-adjusted to normalize the distribution, and then a standardized FGF-21 value was constructed from the log-adjusted values, with mean and SD set to 0 and 1, respectively. The minimum measurable FGF-21 value was 31.3 pg/mL, so all measurements at this level and below were converted to 15.65 pg/mL for analysis (n = 10). A similar procedure for standardization was used for other cytokines, adipokines, and inflammatory markers with a skewed distribution (specifically IL-1, IL-6, IFN, TNF, ESR, CRP, leptin, EGF, VEGF, SAA, MMP-1, MMP-3, TNF-RI, and YKL-40).
Associations between FGF-21 levels and demographics, disease characteristics, and other serum markers were first assessed using individual linear regression analyses at baseline. All variables found to be moderately associated with FGF-21 levels (P < 0.20) were tested together in a multivariable model. A stepwise deletion process was then used to eliminate covariates with P > 0.10. The final model included standard demographics (age, sex) and all variables with P < 0.10 in the multivariable model after stepwise deletion.
Associations between selected outcome measures at baseline (muscle density and area Z-scores, strength outcomes, and physical functioning assessments) and FGF-21 levels at baseline were assessed using 2 linear regression models: 1 only adjusting for age and sex, and 1 also incorporating adjustments for important identified covariates. In each of these models, FGF-21 was tested as both a continuous and categorial variable (quartiles), comparing the highest quartile to all other quartiles. Models using muscle strength measures as outcomes included an adjustment for height.
To assess associations between FGF-21 and other known cytokines, adipokines, and inflammatory markers, linear regression analyses were performed at baseline between FGF-21 and each individual marker. These models were then tested including an adjustment for the previously identified covariates.
Linear regression analyses were conducted evaluating associations between baseline FGF-21 and per-year rates of change of each outcome measure over follow-up. The regression coefficients represent the difference in the rate of change in outcome per year associated with an FGF-21 level of 1 SD higher at baseline. To assess the clinical importance of these relationships, logistic regression models estimating the risk of clinically meaningful worsening in function, strength, and imaging outcomes were also performed. In the primary analysis, we considered death as a worsening in these outcomes; however, we also performed sensitivity analyses wherein participants who died were excluded from the analysis.
Analyses were performed with STATA 15.1 (StataCorp). Since a Bonferroni correction for multiple comparisons was considered overly conservative in the context of related outcomes, we evaluated instead for consistency across analyses.
RESULTS
Basic characteristics and description of cohort. A total of 113 patients with RA were enrolled in the study and 84 patients (74%) returned for follow-up assessment, at a median time of 2.68 years (IQR 2.30–3.56 yrs). The baseline characteristics of the study cohort are shown in Table 1. Supplementary Table 1 (available with the online version of this article) compares characteristics of patients who completed the study to those who were lost to follow-up or died; patients who completed the study were on average younger and had higher FMI Z-scores and lower FGF-21 values than those who did not complete the study.
Basic characteristics of study participants by FGF-21 quartile at baseline.
Factors associated with FGF-21 levels at baseline. Table 2 and Supplementary Table 2 (available with the online version of this article) display associations between FGF-21 levels and participant characteristics at baseline. In univariate models, older age, active smoking, cardiac disease, longer RA duration, greater BMI, and multiple measures of body fat (including FMI-Z, waist circumference, and visceral fat area) were all associated with greater FGF-21 levels. Higher eGFR and current methotrexate (MTX) use were associated with lower FGF-21 levels. In multivariate models, only age, visceral fat area, MTX use, and current smoking remained moderately associated (P < 0.1). None of the measures of RA disease activity or severity (specifically, M-DAS, DAS28-CRP, and SvdH score) were significantly associated with FGF-21 levels.
Associations between FGF-21 levels and participant demographics and disease characteristics at baseline.
Associations between FGF-21 and several cytokines, adipokines, and inflammatory measures were also assessed at baseline. Figure 1 shows results of linear regression analyses; each coefficient on the graph shows the effect of a 1-SD increase of each measure on standardized FGF-21 levels. Several markers, including TNF-RI, YKL-40, VEGF, and resistin, were significantly and positively associated with FGF-21, both before and after adjusting for age, sex, visceral fat area, smoking status, and MTX use. Supplementary Table 3 (available with the online version of this article) contains numerical results for these analyses.

Association between cytokines and inflammatory markers and FGF-21 levels. Graph shows regression coefficients from models regressing FGF-21 levels on each factor. Bars show 95% CI. FGF-21 and all factor levels were converted to standardized scores to allow for direct comparisons. Right-hand coefficients (triangle) for each marker are adjusted for age, sex, visceral fat area, current smoking, and methotrexate use (all at baseline). N = 106 (unadjusted model) and 104 (adjusted) for TNF-RI, YKL-40, VEGF, resistin, CRP, leptin, VCAM-1, IL-6, SAA, EGF, MMP1, and MMP3. N = 111 (unadjusted model) and 109 (adjusted) for ESR. N = 113 (unadjusted model) and 111 (adjusted) for TNF, IFN, IL-1, and adiponectin. CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; EGF: epidermal growth factor; FGF: fibroblast growth factor; IFN-γ: interferon-γ; IL: interleukin; MMP: matrix metalloproteinase; SAA: serum amyloid A; TNF-RI: tumor necrosis factor receptor type I; VCAM: vascular cell adhesion molecule; VEGF: vascular endothelial growth factor; YKL-40: bone glycoprotein 39.
Associations between baseline FGF-21 levels and muscle and functional outcomes. At baseline, after adjusting for age, sex, visceral fat area, current smoking, and MTX use, FGF-21 levels were not associated with skeletal muscle outcomes (specifically muscle density Z-score, muscle area Z-score, peak isometric torque in flexion and extension at the knee, and hand grip strength). Over time, while there were modest associations noted between FGF-21 and the rates of decline of muscle density Z-score (β –0.06, 95% CI –0.12 to 0.008, P = 0.08) and muscle area Z-score (β –0.05, 95% CI –0.10 to 0.006, P = 0.08), baseline FGF-21 levels were also largely not associated with changes in skeletal muscle outcomes (Table 3).
Associations between FGF-21 values and muscle and strength variables.
Adjusting for age, sex, visceral fat area, current smoking, and MTX use, a top-quartile FGF-21 value at baseline was associated with both HAQ score (β 0.34, 95% CI 0.04–0.6, P = 0.03) and SPPB (β –1.68, 95% CI –2.94 to –0.41, P = 0.01). The highest quartile of FGF-21 was also associated with a significantly faster rate of decline in SPPB over time (β –0.57, 95% CI –1.04 to –0.09, P = 0.02; Table 4).
Associations between FGF-21 values and functional outcomes.
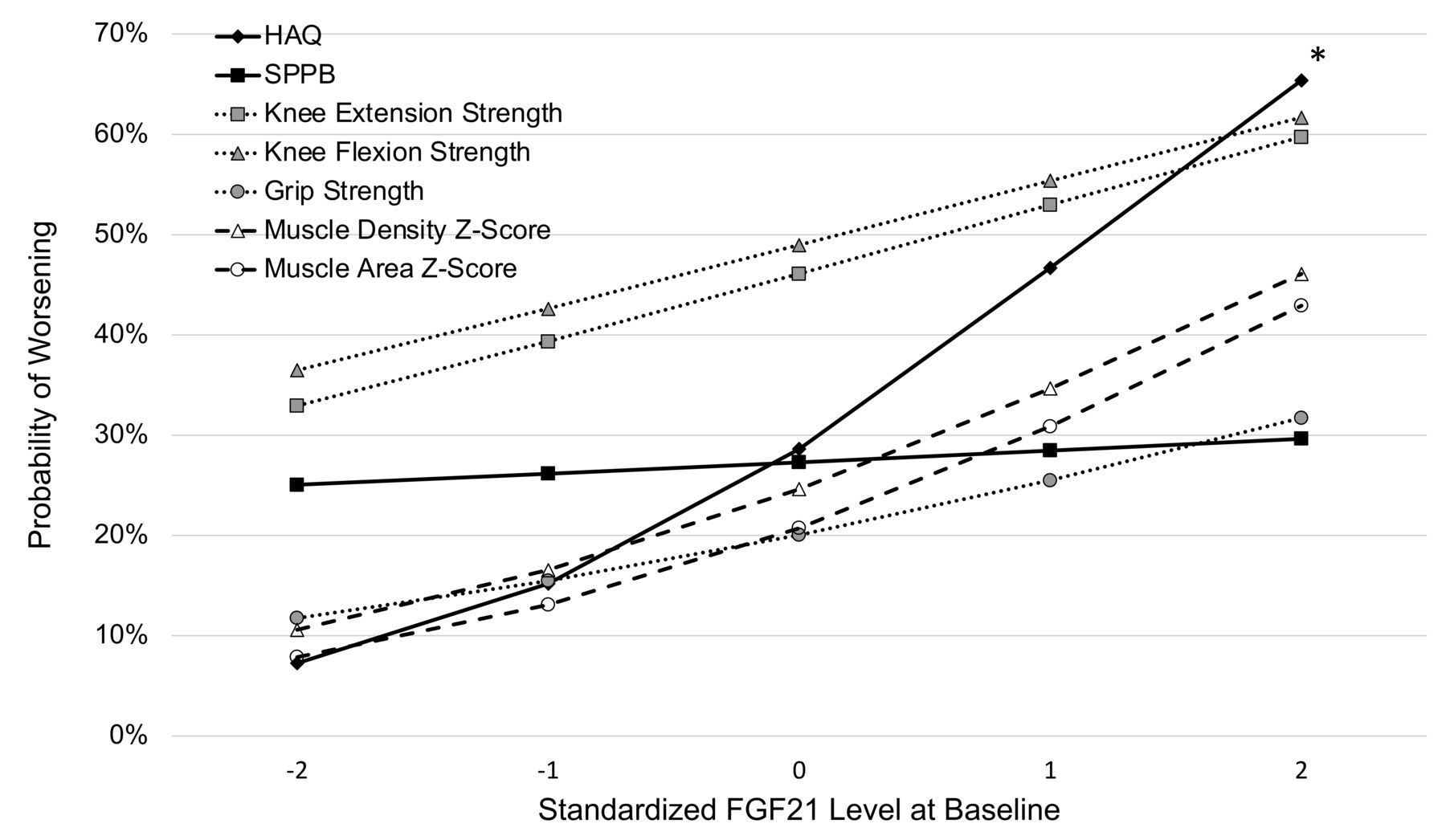
A higher FGF-21 level at baseline (per 1 SD) was associated with greater odds of a clinically meaningful worsening of HAQ score (OR 2.37, 95% CI 1.21–4.64, P = 0.01), and tended toward an association with a greater risk of significant worsening of muscle density Z-score (OR 1.76, 95% CI 0.89–3.47, P = 0.10) and muscle area Z-score (OR 1.85, 95% CI 0.88–3.89, P = 0.11). No association was seen with extension strength (OR 1.35, 95% CI 0.77–2.38, P = 0.30), flexion strength (OR 1.37, 95% CI 0.76–2.49, P = 0.30), grip strength (OR 1.42, 95% CI 0.71–2.85, P = 0.32), and SPPB (OR 1.09, 95% CI 0.42–2.79, P = 0.86; data not shown). All of these models included adjustments for age, sex, visceral fat area, smoking status, and MTX use. Figure 2 displays predicted probabilities of worsening in these outcomes by SD of FGF-21 level based on these models. Supplementary Table 4 (available with the online version of this article) displays results for the sensitivity analysis excluding patients who died; the results are similar. Greater FGF-21 levels (per 1 SD) were also associated with a greater risk of death before follow-up (OR 3.14, 95% CI 1.22–8.07, P = 0.02; unadjusted to avoid overfitting).

Probability of a clinically meaningful negative change in selected measures at second visit, by baseline FGF-21 Z-score. * P < 0.05. Models include adjustments for age, sex, visceral fat area, current smoking, and methotrexate use (all at baseline). Clinically meaningful worsening was defined as follows, or as patient death before visit (N for each regression is listed as well): HAQ: increased by 0.2 (n = 89); SPPB: decreased by 1 (n= 51); extension and flexion strength: decreased by 10% (N = 78, 78); grip strength: decreased by 6.5 kg (n = 86); Muscle density and muscle area Z-score: decreased by 0.5 (n = 82, 76). FGF: fibroblast growth factor; HAQ: Health Assessment Questionnaire; SPPB: Short Physical Performance Battery.
DISCUSSION
To our knowledge, this is the first study evaluating longitudinal associations between FGF-21 and RA disease characteristics, obesity, skeletal muscle deficits, and physical functioning. We observed associations between FGF-21 and greater age, smoking, visceral adiposity, and elevations in inflammatory mediators including TNF-RI, YKL-40, VEGF, and resistin. This study also demonstrated associations between FGF-21 and poor physical functioning, as well as deteriorations in functioning over several years. Overall, these observations support the hypothesis that FGF-21 is a potential marker of adverse inflammatory processes that could predict future functional declines in this population.
The baseline patient characteristics associated with FGF-21 levels are consistent with prior results derived from the general population. We observed that FGF-21 levels were highly associated with all measures of body fat in this study. In other populations, FGF-21 has been observed to be elevated in the contexts of obesity, metabolic syndrome, type 2 diabetes, hypertension, and atherosclerosis10,11,12,13,14,15,42. FGF-21’s associations with smoking, increased age, cardiac disease, and kidney disease have also been reported previously42,43,44,45. Previous studies have reported associations with sex, but this was not observed in our study43.
The observation that MTX use is associated with lower FGF-21 levels is novel. This could indicate that MTX works to ameliorate the inflammatory processes that lead to increases in serum FGF-21. Alternatively, metabolic obesity is a risk factor for elevations in liver enzymes among patients taking MTX46, possibly resulting in drug discontinuation in patients with high FGF-21 levels related to the obesity. Further study will be needed to determine if MTX might have direct beneficial metabolic effects in RA.
At baseline, FGF-21 was not found to be associated with muscle density, muscle area, or muscle strength. However, significant associations were found with measures of physical functioning, and elevated FGF-21 levels were associated with faster rates of decline in functioning. Additionally, while not all the longitudinal comparisons between FGF-21 and changes in muscle variables were statistically significant in this small study, there was remarkable consistency nevertheless in the direction of the effects. These longitudinal models support the hypothesis that FGF-21 levels in patients with RA are reflective of a metabolically adverse profile that is associated with deteriorations in strength and physical functioning47,48,49,50. Notably, FGF-21 at baseline was not found to be associated with any standard composite measures of RA disease activity or severity (including M-DAS, DAS28, SvdH score, and the MBDA score). This result indicates that the processes leading to elevated FGF-21, and therefore the associations identified in this study, are not necessarily related to RA activity, at least as has been historically measured in clinic. However, FGF-21 was associated with several individual serum proteins (TNF-RI, YKL-40, VEGF, and resistin) included in the MBDA assay, even after adjusting for age, sex, visceral fat area, MTX use, and smoking status38,39. The associations with these markers could suggest links between FGF-21 and various components of the RA disease process, and may provide further evidence of an association with inflammatory stress not accounted for in many clinical measures of RA disease activity (including the MBDA composite score itself).
Although we believe this is the largest longitudinal study to date evaluating the role of FGF-21 in RA, the small sample size limited the power to detect modest associations. While the results suggest that FGF-21 levels are associated with deteriorating physical function, larger studies will be needed to more accurately assess its prognostic value and identify levels at which FGF-21 represents a clinically significant risk of decline. Additionally, many patients died or were lost to follow-up, and patients who did complete the study were more likely to be younger, have a more normal FMI Z-score, and have a lower M-DAS. Therefore, given that the sickest patients may be more likely to be lost to follow-up, some of the patients with the highest FGF-21 and the biggest declines in functioning might have been lost, thereby underestimating the associations with FGF-21. Indeed, patients who either died or were lost to follow-up had significantly higher baseline FGF-21 than those who completed the study; this was driven by a very high FGF-21 average among patients who died. While this is an interesting result, the small sample size (only 7 patients died) limited statistical power to evaluate for associations with cause-specific mortality. Finally, while this study adjusted for a wide variety of potential confounders, unobserved confounders may still be present.
Strengths of this study include the comprehensive array of disease measures and muscle quality, strength, and physical functioning assessments collected for each patient. These measurements allowed us to assess the effects of FGF-21 beyond its effect on typical measures of RA disease activity. Additionally, the longitudinal nature of the study allowed us to assess temporal relationships important for understanding the potential prognostic value of FGF-21.
In conclusion, factors associated with higher FGF-21 levels in RA include increased age, smoking, obesity, and MTX use, and associations with deteriorating physical functioning support the hypothesis that serum FGF-21 serves as a biomarker of adverse metabolic processes that can predict greater functional decline. This study builds upon existing research by demonstrating temporal relationships between FGF-21 and long-term functional changes in patients with RA.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
JFB was supported by a Veterans Affairs Clinical Science Research and Development Career Development Award and VA Merit Award (IK2 CX000955, I01 CX001703), and by the University of Pennsylvania Clinical and Translational Research Center (UL1 RR024134). Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under award number UL1TR001878. The contents of this work do not represent the views of the Department of Veterans Affairs or the US Government.
The authors declare no conflicts of interest.
- Accepted for publication October 21, 2020.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}
{kind=link}