

Abstract
Objective Our study aimed to evaluate the cost effectiveness of initiating tocilizumab (TCZ) ± methotrexate (MTX) versus initiating MTX as treat-to-target treatment strategies over 5 years in early disease-modifying antirheumatic drug (DMARD)-naïve rheumatoid arthritis (RA).
Methods Data on resource use were collected with questionnaires at baseline, 3, 6, 12, and 24 months, and yearly thereafter, and were converted to costs using Dutch reference prices. Quality-adjusted life-years (QALY) were calculated using the EQ5D5L, with utility based on Dutch tariff or estimated by the Health Assessment Questionnaire. To account for missing cost data and QALY data and for sample uncertainty, first bootstraps (10,000 samples) were obtained. Second, single imputation using chained equations nested within these bootstrap samples was performed. An economic evaluation was performed for TCZ + MTX and TCZ, compared to MTX, as initial treatment in a treat-to-target strategy from a healthcare and societal perspective over 5 years. Several sensitivity analyses were performed.
Results Mean differences in QALY were small and not significant (TCZ + MTX vs MTX: 0.06, 95% CI –0.02 to 0.13; TCZ vs. MTX: –0.03, 95% CI –0.05 to 0.11). Limited savings in indirect nonhealthcare costs and productivity loss costs (for TCZ only) were observed, but these did not compensate for the higher medication costs. Sensitivity analyses did not materially change these findings, although lower-priced TCZ, or reserving TCZ as initial therapy for prognostically unfavorable RA patients, improved cost effectiveness considerably but did not individually lead to a strategy being cost effective.
Conclusion Based on our analyses, early initiation of TCZ + MTX is not cost effective compared to MTX initiation in a step-up treat-to-target treatment strategy over 5 years in early RA patients.
- biological therapies
- disease-modifying antirheumatic drugs
- epidemiology
- health economics
- rheumatoid arthritis
- quality of life
Rheumatoid arthritis (RA) is a chronic inflammatory disease affecting mainly the joints, in which lifelong treatment is required to reduce symptoms, improve physical function, and avoid structural joint damage. Over the past decades, early treatment with disease-modifying antirheumatic drugs (DMARD) according to the treat-to-target principle, together with the use of newer, more effective, biologic DMARD (bDMARD), improved these outcomes1.
Due to their high costs compared to conventional synthetic DMARD (csDMARD), bDMARD are reserved as second-line treatment after a first DMARD, mostly methotrexate (MTX), which has not shown to be sufficiently effective. Typically, bDMARD are added to the existing csDMARD therapy. Some studies have evaluated tumor necrosis factor inhibitors (TNFi) as initial bDMARD therapy in RA, and have shown that initial treatment with this bDMARD, though effective, is currently not cost effective over 1–2 years2,3,4. Simulation model–based analyses over a longer term (i.e., 5 yrs to lifetime horizon) also conclude that this is not a cost-effective strategy5,6,7.
Tocilizumab (TCZ) is a non-TNFi bDMARD, targeting the interleukin 6 receptor. A recent trial8 and its posttrial follow-up (PTFU)9 investigated the effect of TCZ as first-line treatment in early RA patients. U-Act-Early was a 2-year multicenter, double-blind, randomized, placebo-controlled trial in early (DMARD-naïve) RA patients treated to the target of remission [i.e., Disease Activity Score in 28 joints (DAS28) < 2.6 with ≤ 4 swollen joints]. Patients were assigned to step-up treatment strategies starting with TCZ, MTX, or a combination of these (TCZ + MTX)8. If the treatment target was not achieved, MTX (in the TCZ-monotherapy group) or TCZ (in the MTX group) was added. When patients achieved and remained in remission for ≥ 24 weeks, medication was tapered and finally stopped8. Patients were followed for 3 years after the trial (i.e., PTFU), during which treatment was at the discretion of the treating rheumatologist9.
Results of U-Act-Early and its PTFU showed a high effectiveness of all treatment strategies. Almost all patients achieved sustained remission over follow-up that was achieved earlier in the TCZ strategy groups. Due to active tapering during the trial, we observed that bDMARD use decreased in TCZ-based strategies and increased in the MTX-based strategy, and TCZ use was almost similar in both arms after 2 years. High effectiveness and higher sustained (drug-free) remission rates compared to previous cost-effectiveness bDMARD studies were achieved in U-Act-Early, as well as in its PTFU, possibly due to the patient population with very early RA being treated within the “window of opportunity.” Further, TCZ monotherapy was equally effective as TCZ + MTX as the initial strategy9, in contrast to most TNFi. Since some patients do not tolerate MTX, TCZ monotherapy may have a positive influence on quality of life (QOL) and productivity. Therefore, the our objective was to investigate whether using TCZ (± MTX) as initial therapy in a strict treat-to-target strategy with active tapering in case of sustained remission might be cost effective in very early RA patients compared to MTX as initial strategy, while taking into account costs related to medical consumption, other direct healthcare costs, indirect nonhealthcare costs, as well as costs related to productivity loss. The current study aimed to compare these costs and quality-adjusted life-years (QALY), as a generic measure of effectiveness, of initial treatment with TCZ + MTX, TCZ, and MTX in a treat-to-target treatment strategy over the 5-year observation period.
MATERIALS AND METHODS
Detailed methods of U-Act-Early and PTFU are reported elsewhere8,9. In the current study, we evaluated the cost effectiveness of TCZ (+ MTX) compared to MTX. For this purpose, we used individual patient data of U-Act-Early and its PTFU, hence we performed a trial-based cost-utility analysis (i.e., using empirical study data). Patients visited the outpatient clinic every month during the 2-year trial period, every 3 months during the first year of the PTFU, and every 6 months thereafter. The medical ethics research committee of the University Medical Center Utrecht approved the trial (ID number: ML28388). For the PTFU, the institutional review boards of the participating centers confirmed that the Medical Research Involving Human Subjects Act (WMO) was not applicable. In both studies, all patients gave written informed consent.
QALY. Effectiveness was expressed as QALY, measured at baseline and at 3, 6, 12, and 24 months using the 5-Level EuroQol 5-Dimensions (EQ5D5L), with results expressed as a utility score. Utility is a score ranging from 0 (death) to 1 (full health), and was based on the Dutch tariff10. For the posttrial period, during which EQ5D5L was not measured, and in case of missing EQ5D5L data, utility was estimated from the Health Assessment Questionnaire and age11 (see Supplementary Data 1 for details, available with the online version of this article).
Medication costs. Medication use was based on recorded dose and duration of (nonplacebo) MTX and TCZ, and recorded use (yes/no) for nonsteroidal antiinflammatory drugs (NSAID). If patients dropped out during U-Act-Early (about 25%, n = 80), we assumed that TCZ was discontinued, treatment with MTX (15 mg per week) was continued, and a TNFi (i.e., adalimumab 40 mg subcutaneously biweekly) was added until the end of the trial, as advised by the U-Act-Early study protocol. If the reason for dropout was infection or malignancy (about 34% of dropouts, n = 27), we assumed that treatment was continued with MTX (15 mg per week), and that, for safety reasons, another csDMARD (e.g., sulfasalazine 1000 mg twice a day) was added, instead of a TNFi, in line with the U-Act-Early protocol and clinical guidelines during the inclusion period (i.e., 2010–2012). For patients completing U-Act-Early, but not included in PTFU, medication use (per category) during the first 3 months after U-Act-Early (first 3 months of PTFU) were assumed equal to the use in the last 3 months of U-Act-Early and further set as “missing” and imputed for the analysis.
To calculate medication costs, medication use was multiplied by national prices, separately for bDMARD, csDMARD, and NSAID (Supplementary Table 1, available with the online version of this article)12. If the administration route of the medication was intravenous, we calculated additional costs for day care or hospital care. For NSAID, we assumed the most frequently used NSAID in the trial (naproxen) in a dose of 0.75 g per day.
Other direct healthcare costs and indirect nonhealthcare costs. Other direct healthcare-related resource use (e.g., physician visits, hospital admissions, non-RA medication) and indirect nonhealthcare-related resource use (e.g., travel cost, purchase of a stair lift) typically over the last 3 months were obtained through healthcare resource use questionnaires, as used in previous studies3,4,10,13.
Productivity loss costs. Data about productivity loss was obtained with the work participation questionnaire as filled out at baseline and at 3, 6, 12, and 24 months during the trial, and yearly during PTFU. Costs related to productivity loss were calculated as incidental work loss hours caused by sickness as well as structural reduction in working hours, including discontinuation of paid work. The productivity loss costs related to structural reduction in work were calculated compared to the productivity hours per week at baseline. Working hours lost were valued by the average wage of Dutch citizens by sex to calculate the total productivity loss costs, following the human capital approach10. Productivity loss costs were also calculated, applying the friction cost approach using only structural productivity loss hours during the first 15 weeks (i.e., friction period 2017)10. If the patient reached the retirement age of 65 years, we assumed that they had retired and productivity loss costs no longer occurred.
Costs were calculated using 2017 reference prices in euros (€) and in line with the Dutch costing manual (Supplementary Table 1, available with the online version of this article)10.
Discounting. Costs were discounted using a discount rate of 4% per year, and QALY using a discount rate of 1.5% per year, according to Dutch guidelines for economic evaluations in healthcare10.
Missing data and data imputation. To obtain yearly costs and QALY, linear interpolation was used over scheduled visits within a year. To account for remaining missing cost (12% and 22% during the trial and PTFU, respectively) and QALY (13% and 20%, respectively) values in a year, as well as (population) uncertainty in outcomes, we used the following approach, which has been suggested to be optimal in this situation14. As a first step, 10,000 bootstrap samples (with replacement) were taken per treatment strategy arm. In the second step, single imputation of the missing yearly QALY and cost estimates was performed per bootstrap sample (see Supplementary Data 2 for details, available with the online version of this article).
Analysis. Baseline (inclusion in U-Act-Early) characteristics of the strategy groups were described for the intention-to-treat (ITT) population and the population as included in the PTFU. Mean values (2.5 and 97.5 percentiles, respectively) of costs per category and QALY were calculated for the treatment strategy groups as well as for the differences of TCZ + MTX and TCZ, both compared to MTX over a 2-year (trial period) and 5-year (trial + PTFU) time horizon.
Incremental cost effectiveness ratios (ICER; calculated as difference in costs between 2 strategies divided by difference in effectiveness, expressed as € per QALY gained) were estimated. A healthcare perspective (including only healthcare cost) as well as societal perspectives (including nonhealthcare cost like costs related to productivity) were used for this estimation. The primary analysis uses the ITT population of U-Act-Early (n = 317) and the follow-up period of 5 years. Results were illustrated in cost-effectiveness planes. The distribution of simulations over the quadrants in these planes was also calculated and illustrates if TCZ (+ MTX) is cost effective compared to MTX [e.g., southeast quadrant indicates that lower costs with higher effectiveness: TCZ (+ MTX) is dominant compared to MTX]. Cost effectiveness acceptability curves (CEAC) were constructed to illustrate the probability of TCZ (+ MTX) being cost effective compared to MTX at different willingness to pay (WTP; the price society is willing to pay for a gain of 1 QALY) thresholds.
Sensitivity and scenario analyses. To evaluate the effect of missing data, a complete case analysis was performed (i.e., using data from PTFU population) as sensitivity analyses. To investigate the sensitivity of the results to treatment effect, we assumed QALY were 0.05 higher and lower, respectively, in the TCZ strategies. We also performed a sensitivity analysis using discount rates of 4% per year for both costs and QALY, as is generally in line with international guidelines.
Moreover, the following scenario analyses were performed. As TCZ has recently become available as a subcutaneous injection, making an admission day no longer necessary, we performed a scenario analysis assuming that TCZ is given subcutaneously instead of intravenously, resulting in a reduction of 23% of the total price (Supplementary Table 1, available with the online version of this article). Further, a scenario analysis was performed in which, in addition to subcutaneous administration, reductions in drug price of 10% and 30% were assumed. Finally, we performed an analysis in which only patients with a baseline DAS28 > 5.1 (i.e., more severe disease; a stratification factor for randomization in U-Act-Early) were included8. All sensitivity/scenario analyses are based on discounted costs and QALY (unless otherwise specified, with 4% for costs and 1.5% for QALY, respectively) and over the 5-year time horizon.
RESULTS
Overall, no relevant differences between the treatment groups (as initially randomized) were found at baseline (Table 1). Ninety-one (29%) patients did not participate in the PTFU. Differences were found only for mean baseline working hours per week between patients included in the PTFU and patients not included in the PTFU (22.3 vs 26.7; P = 0.03; Supplementary Table 2, available with the online version of this article). Approximately 80% of all patients were employed at baseline and worked on average 24 h weekly.
Baseline characteristics of patients included in the U-Act-Early trial.
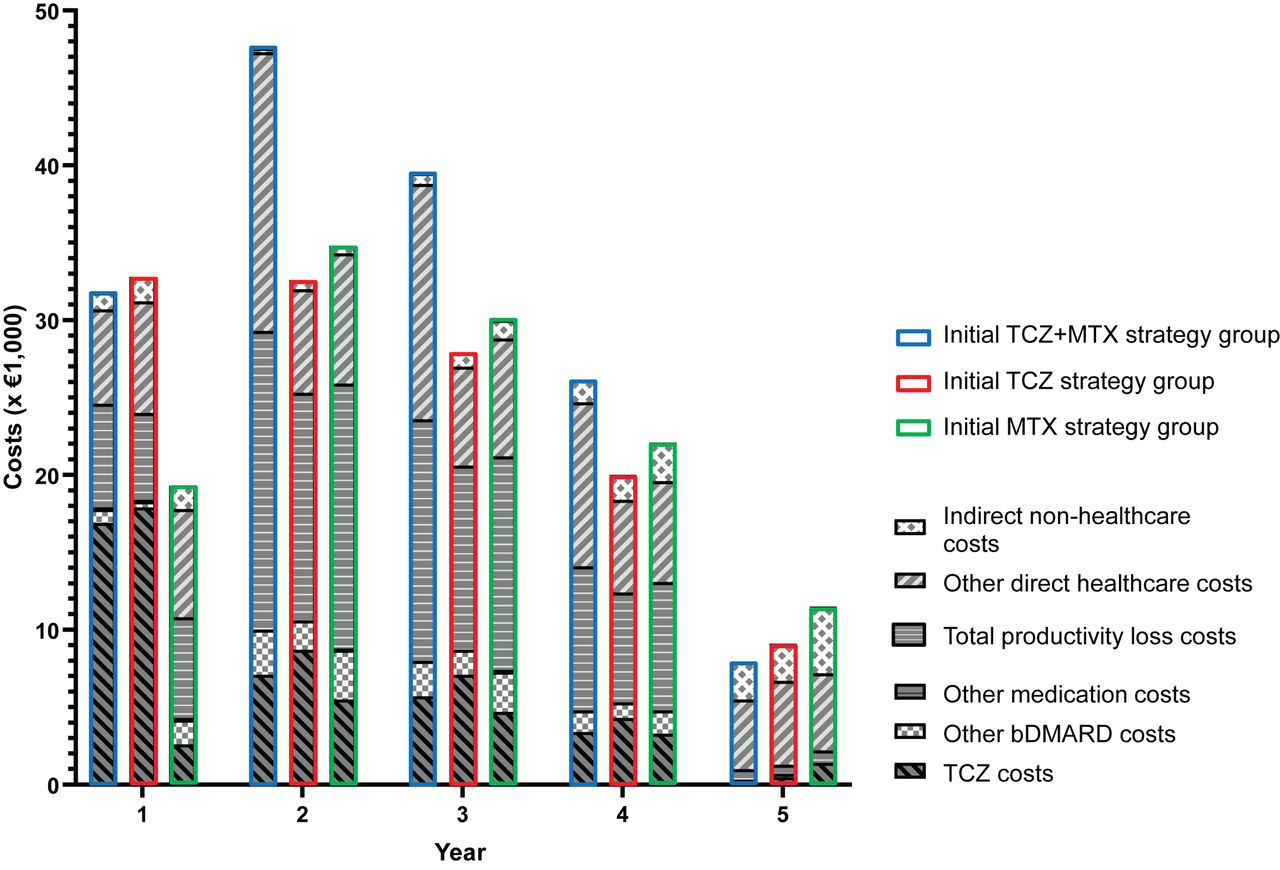
Figure 1 and Supplementary Table 3 (available with the online version of this article) show the cost per category in each year, and over 2 and 5 years. Total medication costs were, as expected, higher in the TCZ strategy groups compared to the MTX strategy group over 2 and 5 years (TCZ + MTX and TCZ at €27,900 and €29,100, respectively, over 2 yrs vs MTX €13,200; and €41,200 and €43,700, respectively, vs €26,600 MTX over 5 yrs). After 2 years, medication costs decreased in all groups, and it was only in the last year (Year 5) that mean medication costs (i.e., total and TCZ costs) were lower for the TCZ strategy groups. Regarding productivity loss costs using the human capital approach, the highest costs over 5 years were observed in the TCZ + MTX strategy group (€51,700) versus TCZ and MTX (€39,900 and €46,500, respectively). Using the friction cost approach for productivity loss costs, differences between TCZ- and MTX-based strategy groups were small. Direct healthcare costs were highest in the TCZ + MTX group, and indirect nonhealthcare costs were lowest in this group over 5 years. A similar number of QALY was attained in all treatment groups over 5 years. Supplementary Table 4 (available with the online version of this article) gives an overview of undiscounted cost and QALY.

Cost (€ × 1000) over time per initial treatment strategy in means. Outcomes based on single imputation nested in 10,000 bootstraps; costs expressed in euros. TCZ + MTX: initiation of TCZ + MTX; TCZ: initiation of TCZ + placebo-MTX; MTX: initiation of MTX + placebo-TCZ. Indirect nonhealthcare costs: costs related to patient and family (e.g., travel costs, buying stair lift); direct healthcare costs: all costs related to healthcare, also for other diseases (RA medication costs excluded); productivity loss costs: costs related to work loss or being less productive; other medication costs: all RA medication costs, including NSAID and csDMARD (excluding bDMARD). bDMARD: biologic disease-modifying antirheumatic drug; csDMARD: conventional synthetic disease-modifying antirheumatic drug; MTX: methotrexate; NSAID: nonsteroidal antiinflammatory drug; RA: rheumatoid arthritis; TCZ: tocilizumab.
Mean differences between the treatment strategies with 95th percentile ranges per cost category and QALY are shown in Table 2.
Mean (2.5–97.5 percentile) difference in costs (€, rounded to the nearest hundreds) and QALY, and ICER with distribution in cost-effectiveness plane (%).
For TCZ + MTX over 5 years, direct healthcare costs and medication costs as well as total cost are significantly (i.e., the 95th percentile range of the difference does not include 0) higher compared to those of MTX, and indirect nonhealthcare costs significantly lower. Productivity loss costs and QALY are numerically higher without being significant. Regarding the 2- to 5-year evaluation period, the difference in total cost increases and the QALY difference remains the same, decreasing the cost effectiveness of TCZ + MTX compared to MTX.
For TCZ, direct healthcare costs (RA medication costs excluded) and productivity loss costs are lower compared to MTX (not significant), but total costs are significantly higher. Over a 5-year evaluation period, the difference in total cost remains constant and significantly higher, except if productivity loss costs are calculated using the human capital approach, which results in a smaller, nonsignificant increase in costs compared to those of MTX. Differences in QALY are not significant, but the small numerical advantage over the 2-year period is lost over the 5-year period, leading to a small disadvantage in QALY for TCZ versus MTX.
TCZ + MTX has an ICER between 526,674 and 594,021 per QALY gained, compared to MTX (depending on perspective taken and method of calculating productivity loss costs), and is inferior in 23% of all bootstrap samples over 5 years. TCZ has a negative ICER (between –426,967 and –149,241, depending on the perspective taken and method of calculating productivity loss costs) as, on average, QALY were lost over 5 years, and TCZ is inferior in between 47% and 65% of all bootstrap samples over 5 years. Taking the societal perspective, using the human capital approach, TCZ dominated (i.e., more QALY and lower costs) in 8% of all bootstrap samples, and in 18% TCZ was found less expensive, but also less effective (Figure 2). Outcomes based on undiscounted values are shown in Supplementary Table 5 (available with the online version of this article).

Cost-effectiveness planes for the TCZ-based initiation treatment strategy groups versus the MTX initiation strategy group over 5 years, using the societal perspective (human capital approach). TCZ + MTX: initiation of TCZ + MTX strategy group; TCZ: initiation of TCZ + placebo-MTX strategy group; MTX: initiation of MTX + placebo-TCZ strategy group. TCZ dominated (i.e., more QALY and lower costs) in 8% of all bootstrap samples (8% chance that the intervention is cost effective) compared to MTX. MTX: methotrexate; QALY: quality-adjusted life-years; TCZ: tocilizumab.
The probability of TCZ (+ MTX) being a cost-effective intervention over 5 years, using different WTP thresholds for a QALY, was low in general, but somewhat higher for TCZ compared to TCZ + MTX (Figure 3, and Supplementary Figures 1 and 2, available with the online version of this article).

Cost-effectiveness acceptability curve for the TCZ-based initiation treatment strategy groups versus the MTX initiation strategy group over 5 years, using the societal perspective (human capital approach). TCZ + MTX: initiation of TCZ + MTX strategy group; TCZ: initiation of TCZ + placebo-MTX strategy group; MTX: initiation of MTX + placebo-TCZ strategy group. Using a willingness to pay of €50,000, the probability that TCZ + MTX or TCZ is more cost effective compared to MTX is 0% or 20%, respectively. MTX: methotrexate; TCZ: tocilizumab.
Sensitivity and scenario analyses. Results of the sensitivity/scenario analyses are shown in Table 3. Overall results confirmed that the probability that TCZ strategies are cost effective is low. The exception may be if a cost reduction of 30% for subcutaneously administrated TCZ is assumed. In this case, the cost savings are considerable and may compensate for the limited QALY loss for TCZ compared to those of MTX (taking a societal perspective and using a human capital approach). TCZ is found to be dominant in 25% of the bootstrap samples, and in 49%, less expensive but also less effective. Assuming a QALY gain of 0.05, the average QALY difference between TCZ and MTX becomes positive, and TCZ is dominated in 15% of all bootstrap samples; in 11%, TCZ was found less expensive but also less effective. In the subgroup of patients with a DAS28 > 5.1 at start of treatment, TCZ is found to be dominant in 21% of the bootstrap samples, and in 24% less expensive but still somewhat less effective (mean difference in QALY –0.01).
Mean (2.5–97.5 percentile) difference in costs (€, rounded to the nearest hundred) and QALY, and ICER with distribution in cost-effectiveness plane (%)
Outcomes based on undiscounted values are shown in Supplementary Table 6 (available with the online version of this article). Supplementary Figures 3 and 4 illustrate the CEAC at different WTP, for our base case and all sensitivity analyses.
DISCUSSION
We hypothesized that initiating a TCZ-based strategy using a strict treat-to-target approach and including a clear tapering strategy when in sustained remission might become cost effective. Our results do not confirm this hypothesis: We found that treat-to-target treatment strategies initiating TCZ as first treatment after diagnosis of RA are not cost effective compared to a treatment strategy initiating MTX. Our results are in line with those of previous research, in which the cost effectiveness of early initiation of bDMARD compared to MTX was analyzed in early (DMARD-naïve) RA patients7.
The observed decrease in medication use during U-Act-Early, however, did not decrease further in the PTFU9. When a tapering protocol had been included in the PTFU, this might have led to a further decrease in TCZ use and might have increased cost effectiveness of TCZ strategies compared to MTX. Interestingly, our study showed that medication costs did decrease over time but remained higher for TCZ strategies; the only exception was the final (Year 5) observation, where medication cost became lower in both TCZ strategy groups compared to MTX. Because total medication costs, productivity loss costs, and direct healthcare costs are lower in TCZ-based treatment strategies specifically in Year 5, we hypothesize that this may be due to patients needing less intensive treatment owing to their initial intensive treatment strategy during the window of opportunity. However, an evaluation over a longer time horizon would be needed to definitively establish this. Further, the differences between TCZ (+ MTX) and MTX regarding productivity loss costs were lower than expected. Interestingly, productivity loss costs were saved only in the TCZ group, not in the TCZ + MTX group, compared to MTX. This indicates that omitting MTX may be an advantage in terms of productivity effects of the treatment, as MTX is associated with (mild) adverse events15. In line with this, limited savings in overall healthcare costs and indirect nonhealthcare costs were made in the TCZ group. We did not include presenteeism in these costs (i.e., costs of being less productive during working hours), and this omission may have led to a higher effect of productivity on cost savings.
However, the sensitivity/scenario analyses show that the effect would need to be substantial to materially influence the results. Specifically, sensitivity analyses showed that it is only with a combination of a substantial TCZ price reduction and treatment of only the subgroup of early RA patients with a DAS28 > 5.1 at the start of treatment that TCZ-based strategies may become cost effective. The results were based on the human capital approach, as it is internationally the most widely used method and accounts most extensively for productivity effects in our sensitivity/scenario analyses, where the aim was to investigate if TCZ-based strategies could be cost effective in some of the analyses. No sensitivity/scenario analyses were performed for the type or costs of follow-up treatment in patients who dropped out because the number of those patients as well as the duration of this follow-up treatment were similar between treatment strategy arms, indicating that these analyses would not have resulted in differences in costs when comparing the treatment strategies. Overall, no differences in QALY were shown in our study; this is in line with the majority of earlier performed studies as shown in a systematic review7. The unexpected numerically lower number of QALY obtained with TCZ versus MTX over 5 years may be due to the fact that TCZ was not self-administered. The additional hospital visits for TCZ infusions may have been a burden for patients, resulting in QALY losses. We would expect a gain in QALY for early RA patients if treated with TCZ subcutaneously, compared to intravenously16.
The current study has several limitations. First, there were considerable missing data, which we handled by resampling using a large number of bootstraps (10,000) and imputation. This 2-step method was previously described as an optimal way to handle uncertainty due to both sampling and missing data14. Second, our study had a reasonably short 5-year time horizon, whereas a lifelong time horizon would be ideal to establish the final effect of short-term intervention in early RA, given that it is a chronic disease. Although extension of the time horizon to lifetime would have been possible with a health economic modeling approach (e.g., discrete-event simulation, Markov modeling) using our patient data as part of the input, this was beyond the main aim of this study; however, it would be interesting for future research. Third, it was not possible to calculate the exact NSAID costs. We assume that our choice for naproxen, as one of the 3 most used NSAID in the Netherlands with minimal price differences, results in a plausible estimate of NSAID costs for this population. Further, the combination of NSAID and other csDMARD costs (i.e., other medication costs) are only maximally 1% of total medication costs. Therefore, it is unlikely that a more precise estimate of NSAID costs would influence our results.
The strengths of the current study are the availability of real-world data on QOL and resource use, preventing the need for models to estimate outcomes. Also, the 317 patients included in the current analysis were treated according to the treat-to-target approach, which enhances the generalizability for patients with RA in the Netherlands and other European countries.
Based on our analyses, early initiation of TCZ, with or without MTX, is not cost effective compared to MTX initiation in step-up treat-to-target treatment strategies over 2 or 5 years in early RA patients. Based on sensitivity analyses, subcutaneous administration of lower-priced TCZ may be cost effective compared to MTX in the subgroup of patients with high disease activity at the start of treatment.
ACKNOWLEDGMENT
We thank all patients for their participation, as well as anyone who was involved in conducting these trials and other personnel for their contribution, especially the rheumatologists and study nurses of the participating institutions.
Footnotes
The U-Act-Early trial and the U-Act-After study were funded by Roche Nederland B.V.
J.L. reports personal fees from Arxx Tx, personal fees from Gesyntha, personal fees from Eli Lilly, personal fees from Boehringer, personal fees from Sanofi-Genzyme, personal fees from Leadiant, personal fees from Roche, grants from Astra Zeneca, grants from MSD, and grants from Roche, outside the submitted work. A.P-S. reports personal fees from F. Hoffmann-La Roche, outside the submitted work; M.B. is an employee of Roche Nederland B.V. J.B. reports grants from Roche during the conduct of the study.
- Accepted for publication July 15, 2020.
- Copyright © 2021 by the Journal of Rheumatology
REFERENCES
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.








{kind=link}
{kind=link}
{kind=link}