

Abstract
Objective. To characterize skin severity and joint activity outcomes and associated treatment changes in patients with psoriatic arthritis (PsA) through 12 months of follow-up after enrollment in the Corrona Psoriatic Arthritis/Spondyloarthritis (PsA/SpA) Registry.
Methods. Patients ≥ 18 years of age with a diagnosis of PsA and a history of psoriasis between March 21, 2013, and September 30, 2016, were enrolled (n = 647). Demographics, clinical features, and treatment characteristics were collected and stratified by skin severity and joint activity. Change in joint and skin from enrollment to the 12-month visit was classified by change in category of Clinical Disease Activity Index (CDAI) or body surface area (BSA). Tests of association evaluated the relationship between changes in therapy and changes in skin severity and joint activity.
Results. Patients with improvement in both joint activity and skin severity saw the largest median reduction in both CDAI and BSA, while those who worsened in both had the greatest median increase in both CDAI and BSA. The majority of PsA patients (> 50%) had no change in skin severity regardless if they had reduced therapy (50%), no therapy changes (54%), or increased therapy (56%; P = 0.5875). However, there was a significant association between changes in therapy and changes in joint activity (P < 0.001). Patients who increased therapy were more likely to have improvement in joint activity (32%) compared to patients who reduced therapy (22%) or had no therapy changes (11%).
Conclusion. The clinical implication for our findings suggests the assessment and incorporation of both skin and joint components may be advisable.
Psoriatic arthritis (PsA) is a chronic inflammatory disease, with manifestations that include inflammation of the joints, periarticular structures, and skin1. Psoriasis affects up to 3.2% of the population in the United States2, and up to 30% of patients with moderate to severe psoriasis also have PsA3. Previous studies of patients with PsA have shown a higher impairment of quality of life measures and an increase in overall comorbidities compared to psoriasis4,5. The assessment of patients with PsA requires the consideration of major disease domains, including peripheral arthritis, axial disease, enthesitis, dactylitis, nail disease, and skin disease. Patient treatment decisions should be tailored to the individual and may be based on disease activity, prognostic factors, access to therapy, and comorbidities6.
Many biologic treatments used in psoriasis are also effective in PsA. New and emerging biologics, such as interleukin (IL)-17A inhibitors (ixekizumab and secukinumab) and IL-23 inhibitors (guselkumab and risankizumab), have shown encouraging clinical results in treating PsA and psoriasis, with ixekizumab and secukinumab currently being used in the treatment of both diseases. Collaborative efforts between dermatologists and rheumatologists, along with further research into patient stratification, are needed to enable clinicians to make the best use of the myriad biologic treatment options available7,8. Given the relationship between PsA and psoriasis, treatment of both joint and skin symptoms is important for overall disease management for patients with PsA7,9. Managing patients with PsA requires a greater understanding of how joints and skin may respond differently to available therapies.
To our knowledge, no studies have investigated the relationship between changes in drug therapy and changes in skin and joint outcomes in patients with PsA. Understanding the outcomes seen in skin disease severity and joint disease activity may identify existing treatment gaps. Therefore, the objective of our study was to characterize skin and joint outcomes and associated treatment changes in patients with PsA through 12 months of follow-up after enrollment in the Corrona Psoriatic Arthritis/Spondyloarthritis (PsA/SpA) Registry.
MATERIALS AND METHODS
Study setting. The Corrona Psoriatic Arthritis/Spondyloarthritis (PsA/SpA) Registry is an independent, prospective, observational cohort of patients with PsA recruited by rheumatologists at 40 private and academic practice sites across 25 states in the US. As of March 31, 2018, the Corrona PsA/SpA registry database included information on 2827 patients and 11,525 patient visits, and approximately 6278 patient-years of follow-up observation time had been collected. The mean time of patient follow-up was 3.1 years (median 3.5 yrs). Information on disease duration; prognosis; disease severity and activity; medical comorbidities; use of medications including biologics; conventional synthetic disease-modifying antirheumatic drugs (csDMARD) and prednisone; and adverse events were collected from both patients and their treating rheumatologists.
Institutional review board approval. The Corrona PsA/SpA Registry was established according to the Declaration of Helsinki. All participating investigators were required to obtain full board approval for conducting noninterventional research involving human subjects. A central institutional review board (IRB) granted sponsor approval and continuing review (New England Independent Review Board, NEIRB No. 120160610). Respective IRB supplied full board approval for those academic investigative sites that did not receive a waiver to use the central IRB. Documentation of approval was submitted to Corrona before initiating any study procedures. All registry patients provided written informed consent and authorization before participating.
Study population. Our study population included 647 patients from the Corrona PsA/SpA Registry. These patients were continuously enrolled following an index date defined as enrollment into the Corrona PsA/SpA Registry between March 21, 2013, and September 30, 2016. Enrolled patients included those ≥ 18 years of age with a diagnosis of PsA (with or without SpA) and with a history of psoriasis before or at the time of enrollment into the registry. Patients must have had 12 months of follow-up with body surface area (BSA) and Clinical Disease Activity Index (CDAI) assessments, available at enrollment and at their 12-month visit.
Data analyses. Demographic characteristics, duration of PsA and psoriasis, clinical characteristics, patient-reported outcome measures (PROM), history of PsA drug therapy, and information on current drug therapy at enrollment were collected. Patients were entered into 1 of 12 cohorts based on joint disease activity and skin disease severity. Skin disease severity and joint disease activity were categorized as follows: low skin (BSA 0–1%), mild skin (BSA > 1 to 3%), moderate skin (BSA > 3 to 10%), and high skin (BSA > 10%); and low joint (CDAI ≤ 10), moderate joint (10 < CDAI ≤ 22), and high joint (CDAI > 22). We compared baseline patient characteristics, clinical and disease characteristics, and PROM among the 12 stratified skin disease severity–joint disease activity groups using appropriate methods: ANOVA for continuous variables and chi-square test of association (for categorical variables; Fisher test was used if cell count was < 5).
Improvement in skin disease severity and joint disease activity. Patients were considered to have improved in skin disease severity if they were in a lower skin disease severity category at the 12-month follow-up visit compared to status at enrollment. Likewise, patients were considered to have worsened in skin disease severity if they were in a higher skin disease severity category at the 12-month follow-up visit compared to status at enrollment. Patients who remained in the same skin disease severity category were defined as “no change.” Similar definitions were used to define improvement/worsening/no change in joint disease activity. Patients were then categorized into 1 of 9 combined skin/joint improvement groups: improve in both skin and joint; worsen in both skin and joint; no change in either skin or joint; improve in skin/no change in joint; improve in joint/no change in skin; worsen in skin/improve in joint; worsen in joint/improve in skin; worsen in skin/no change in joint; and worsen in joint/no change in skin. Improvement in skin disease severity and joint disease activity was evaluated in all patients and stratified subgroups by minimal disease activity (MDA) status at baseline.
Changes in drug therapy. Patients were categorized into the following drug status groups: change in therapy or no change in therapy. Changes in therapy that occurred between enrollment and the 12-month visit were captured. “Change in therapy” included a reduction (patient reducing number of DMARD) or an increase (patient adding to number of DMARD or switching from 1 DMARD to another). Reasons for discontinuation were categorized as “efficacy,” “safety,” “tolerability,” “other,” or “unreported.” Change in joint disease activity and skin disease severity from enrollment to the 12-month visit was classified by change in category of CDAI or BSA. P values from chi-square tests of association or Fisher exact test (if cell counts were ≤ 5) were calculated to evaluate the association between changes in therapy and changes in skin disease severity and/or joint disease activity. The association between changes in drug therapy and change in joint disease activity and/or skin disease activity was evaluated in all patients and within stratified subgroups by MDA status at baseline.
RESULTS
Patient baseline demographics and clinical characteristics are presented in Table 1. In our study, 647 patients were included, mean (SD) age for all patients was 55.1 (12.6) years, 95% of patients were White, and 52% were females. Of the 647 patients, 47% were categorized as low skin (BSA 0–1%); 19% mild skin (BSA > 1 to 3%); 21% moderate skin (BSA > 3 to ≤ 10%), 13% high skin (BSA > 10%); 66% low joint (CDAI ≤ 10); 26% moderate joint (10 < CDAI ≤ 22), and 8% high joint (CDAI > 22). For PsA, the mean (SD) disease duration was 11.8 (9.7) years for all patients, with the longest duration of 15.0 (10.4) years in the high skin/low joint subgroup. Those with the highest skin severity had the longest duration of PsA. The mean duration of psoriasis was 21.2 (14.7) years for all patients, with the longest duration of 28.0 (17.4) years in the high skin/moderate joint subgroup. As with PsA, those in the highest skin subgroup (> 10%), had the longest duration of psoriasis, compared to other skin subgroups. Further, there were significant differences between subgroups for duration of PsA (P = 0.030). Only 17.0% of patients were normal weight (BMI < 25), 32.5% were overweight (25 ≤ BMI < 30), and 50.6% were obese (BMI ≥ 30). The mean BMI for all patients was 31.2 (obese), 40% of all patients had hypertension, nearly 13.9% of all patients had diabetes, and a similar percentage (13.8%) suffered from depression. However, except for depression (P = 0.04), there were no significant differences among the subgroups for these characteristics. Overall, about 1/4 of all patients had enthesitis. There was a significant difference in proportion of patients with enthesitis across BSA/CDAI categories. Within BSA categories, patients in the low joint disease activity category had a lower proportion of patients with enthesitis compared to patients in moderate or high joint disease activity categories. Although the data in Table 1 do suggest there may be proportionally higher enthesitis in patients with low skin disease activity in this registry, we compared patients with low BSA (n = 306) to those with high BSA (n = 81) and found the proportions of enthesitis to be 27.1% and 16.0%, respectively. However, the mean (SD) Spondyloarthritis Research Consortium of Canada (SPARCC) scores among those with enthesitis were 4.3 (2.7) and 6.4 (4.5) for low and high BSA, respectively. We also found similar proportions of patients with dactylitis (5.9% for low BSA, 8.6% for high BSA). Therefore, given these data and the small sample sizes (306 for low BSA, 81 for high BSA), we are reluctant to overemphasize this finding until multiple and larger sample sizes are evaluated. We believe this would be an interesting question to answer in a larger dataset (data not shown).
Patient baseline demographic and clinical characteristics of all PsA patients at time of enrollment; stratified by levels of BSA and CDAI.
The mean SPARCC scores for those with enthesitis were significantly different across all subgroups (P = 0.048). Patients in the high skin/high joint subgroup had the highest nail psoriasis visual analog scale (VAS), with a mean (SD) score of 38.1 (23.4). Overall, 8% of patients had dactylitis. There was a significant difference in the proportion of patients with dactylitis across BSA/CDAI categories. Within BSA categories, the low joint disease activity group had a lower proportion of patients with dactylitis compared to patients in moderate or high joint disease activity. Among patients with nail involvement, the mean (SD) nail VAS score was 15.0 (18.2). There was a significant difference in mean Nail VAS score among the BSA/CDAI categories. Within BSA categories, patients in high joint disease activity had the highest mean Nail VAS scores. Over 47% of all patients were in MDA at baseline, with the number of patients in MDA decreasing with increasing BSA and CDAI. Within subgroups, 73% of patients in the low skin/low joint category, 65% in mild skin/low joint, 51% in moderate skin/low joint, and 37% in high skin/low joint had achieved MDA (P < 0.001).
When pooling the means of the summarized results of the patient global skin assessment in Table 1, we found that patient global skin VAS increases with BSA. The high BSA group had a smaller number of patients, but in general, the patient global skin assessment was lower in the low BSA group and higher in the moderate and high groups. For low BSA, mild BSA, moderate BSA, and high BSA, the pooled patient global VAS score means were 37.9, 41.4, 43.8, and 45.9, respectively (data not shown).
Table 1 also presents PROM at the time of enrollment. The mean (SD) Health Assessment Questionnaire (HAQ) was 0.6 (0.7) for all patients with the highest mean (SD) HAQ of 1.9 (0.5) among patients in the high skin/high joint subgroup. Patient-reported EuroQuol Group 5 Dimensional (EQ-5D) VAS was 72.4 (20.9) for all patients and lowest (worst health state) among patients in the high skin/high joint subgroup [mean (SD) of 34.8 (25.8)]. There were statistically significant differences between all subgroups for HAQ and EQ-5D VAS scores (both P < 0.001). Patient-reported pain was 36.3 (29.4) for all patients, with the worst pain rating (mean 83.5, SD 12.0) in the high skin/high joint subgroup.
Overall, 55% of patients had no change in skin disease severity (remained in same severity group at 12-month follow-up visit compared to enrollment visit), while 30% saw improvement in skin disease severity (median decrease in BSA ranging between 2–5%) and 16% had worsening skin disease severity (median increase in BSA ranging from 2 to 3%). Likewise, 69% of patients had no change in joint disease activity, whereas 19% saw improvement (median decrease in CDAI ≥ 5.5) and 12% had worsening joint disease activity (median increase in CDAI ≥ 6.5; data not shown). Table 2 presents the change in CDAI and BSA by skin disease severity and joint disease activity status. When examining the entire population of 647 patients, we found that 8% of patients had improvement over 12 months in both domains and 41% had no improvement in either domain, with the remainder of patients showing improvement in 1 domain with no change or worsening of the other domain. Patients with improvement in both joint disease activity and skin disease severity saw the largest median reduction in both CDAI and BSA, while those who worsened in both had the greatest median increase in both CDAI and BSA.
Median change in CDAI and BSA by skin disease severity and joint disease activity status in all patients.
Table 3 presents the relationship between improvement in skin disease severity and/or joint disease activity and changes in drug therapy from baseline to 12-month follow-up visit among all patients. The majority (57%) had no change in therapy within the first 12 months after enrollment while 35% had an increase in therapy and 8% had a reduction in therapy. Among the 21 patients that had worsened in both joint disease activity and skin disease severity, 38% had no change in therapy, 14% had reduced therapy, and 48% had at least 1 change in therapy. Of the 54 patients who had improvement in both domains, 37% had no change in therapy, 11% reduced therapy, and 52% had at least 1 change in therapy. A larger percentage of patients who saw joint improvement alone (58%) had at least 1 change in therapy versus those with skin improvement (41%). Of the 194 patients who improved in skin disease severity alone (not taking into account changes in joints), 60% had no change in therapy, 9% had reduced therapy, and 41% had at least 1 change in therapy. Among the 120 patients who improved in joint disease activity alone (not taking into account changes in skin), 33% had no change in therapy, 10% reduced therapy, and 58% had at least 1 change in therapy. Of the 100 patients that worsened in skin severity alone, the majority (52%) had no change in therapy, while 43% of the 79 patients who worsened in joint activity alone had no change in therapy. Among patients with a reason for changing therapy, “lack of efficacy” was the most frequently identified reason for therapy change (Table 3).
Treatment changes among the 647 patients by improvement group for skin disease severity and joint disease activity.
As noted, the majority (57%) of patients did not have a change in therapy within the first year after enrollment; however, 284 (47%) patients were in MDA at time of enrollment. When evaluating changes in therapy stratified by MDA status at enrollment, we observed that 71% of patients who were in MDA at enrollment had no therapy changes, versus only 45% of patients who were not in MDA at enrollment (Table 4). Only 19% of patients in MDA at enrollment had an increase in therapy versus 48% of patients not in MDA at enrollment.
Changes in therapy and improvement in skin disease severity and joint disease activity stratified by baseline minimal disease activity (MDA) status.
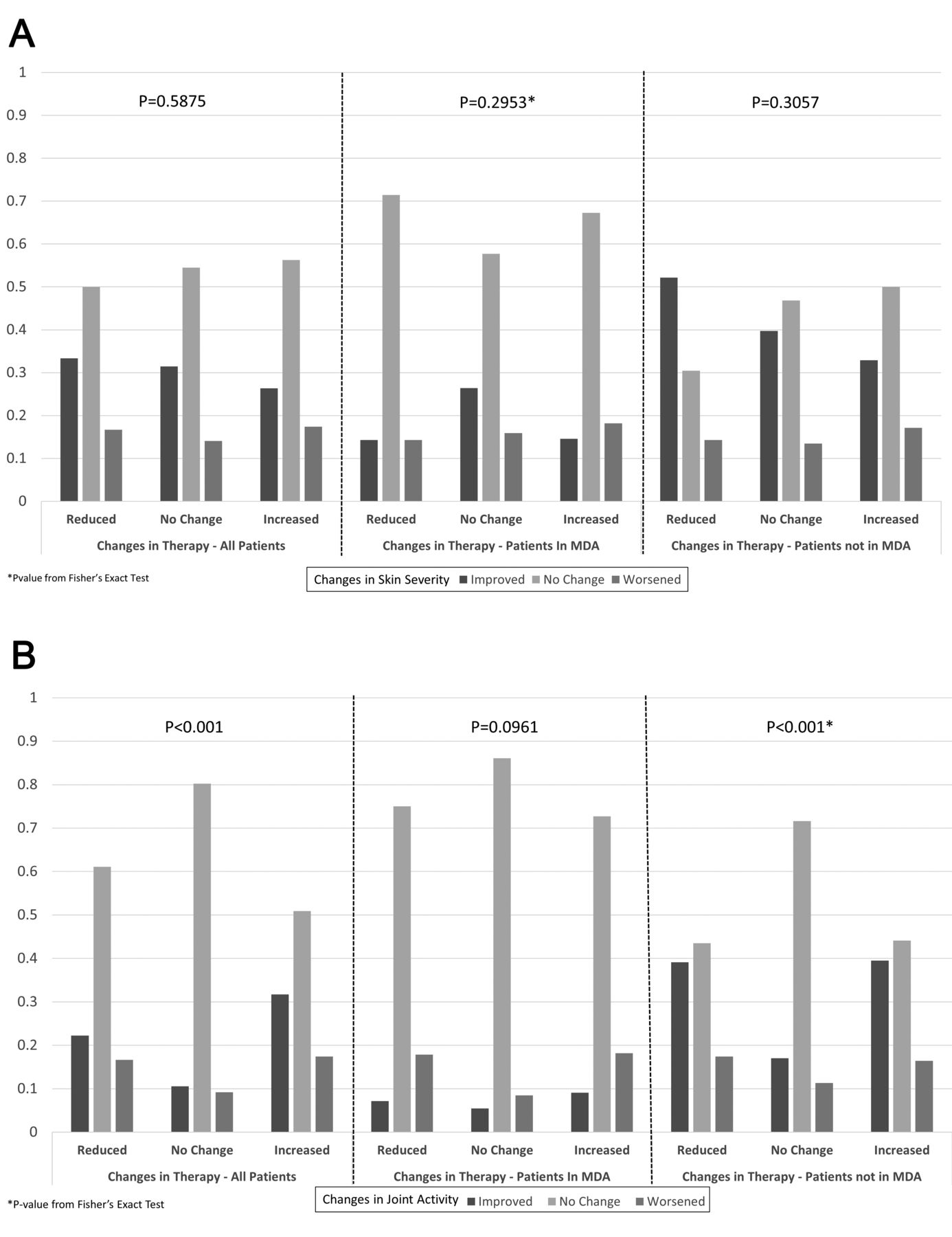
We observed that the patients who had an increase in therapy were more likely to show improvement in joint disease activity but not in skin disease severity. Figure 1A summarizes changes in skin disease severity and Figure 1B summarizes changes in joint disease activity, with therapy decisions for all patients stratified by MDA status at baseline. The majority of PsA patients (> 50%) had no change in skin disease severity (remained in same severity category), regardless of whether they had reduced therapy (50%), no therapy changes (54%), or increased therapy (56%; P = 0.5875, Figure 1A). However, there was a significant association between changes in therapy and changes in joint disease activity (P < 0.001; Figure 1B). Patients who increased therapy were more likely to have improvement in joint disease activity (32% of these patients) compared to patients who reduced therapy (22%) or had no therapy changes (11%). For patients in MDA at baseline, the vast majority (> 50%) of patients had no change in skin disease severity or joint disease activity (even if therapy changes had occurred) and there was no association between changes in therapy and changes in skin disease severity (P = 0.2953; Figure 1A) or changes in joint disease activity (P = 0.0961; Figure 1B). Among patients not in MDA at baseline, patients who experienced some type of therapy changes (increased therapy or reduction of therapy) had similar improvement in joint disease activity (39%), which was higher compared to those with no change in therapy (only 17% improved; P < 0.001; Figure 1B). On the other hand, there was no association of the change in therapy with change in skin disease severity for the patients not in MDA (P = 0.3057; Figure 1A).

(A) Changes in therapy and skin disease severity among all patients, stratified by MDA status at baseline. (B) Changes in therapy and joint disease activity among all patients, stratified by MDA status at baseline. MDA: minimal disease activity.
DISCUSSION
To our knowledge, many of these analyses involving patients with PsA have not been performed in a real-world setting. In addition, comparisons between 12 cohorts based on skin severity and joint disease activity have not been previously shown. We believe our study is the first to simultaneously investigate skin and joint outcomes in association with treatment changes in patients with PsA. A large number of patients in our study were in the low skin activity group at the beginning of the study and subsequently had no change in therapy at the 12-month follow-up. However, when patients did have an increase in therapy, they were more likely to show improvement in joint disease activity over skin disease severity. These findings may be due, in part, to an increased emphasis on joint, rather than skin, assessment and improvement. Our study cohort was derived from patients seen by rheumatologists; therefore, their care might have been focused on arthritic symptoms rather than skin manifestations. It is conceivable that therapies chosen for treatment were selected based on their effectiveness for arthritis rather than skin.
Patients with improvement in both joint disease activity and skin disease severity saw the largest median reduction in both CDAI and BSA, while those who worsened in both categories had the greatest median increase in CDAI and BSA. We believe our results underscore the need for a treat-to-target (T2T) strategy in PsA addressing both joint disease activity and skin disease severity10. The Tight Control of Psoriatic Arthritis (TICOPA) study was the first to test the T2T concept in PsA. Results from the TICOPA study showed patients in the tight control group were nearly 2-times more likely to achieve the American College of Rheumatology 20% response (OR 1.91, 95% CI 1.03–3.55; P = 0.04) and nearly 3-times more likely to achieve a Psoriasis Area and Severity Index 75% response (OR 2.92, 95% CI 1.51–5.65, P = 0.02) at 48 weeks than the standard care group, thus suggesting that a T2T strategy is appropriate for PsA11.
To achieve better results in both skin disease severity and joint disease activity, the importance of collaborative care among rheumatologists and dermatologists is increasingly being recognized. International organizations, such as the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) and the members of the Psoriasis and Psoriatic Arthritis Clinics Multicenter Advancement Network (PPACMAN) in North America, are working towards simultaneously improving care for patients with psoriasis and PsA and recognizing arthritis at an early stage12. Our findings that some patients with severe skin and/or joint involvement did not see improvement highlights the need for rheumatologists and dermatologists to work collaboratively in the long-term management of both domains of PsA13,14,15,16,17,18. Psoriasis typically presents years before symptoms of PsA, with a lag time of 7–12 years from the onset of psoriasis to the diagnosis of PsA. Since most patients with PsA present to a dermatologist before the onset of joint symptoms, routinely screening psoriasis patients for PsA gives the dermatologist the opportunity to refer the patients to a rheumatologist earlier in the disease, leading to improved outcomes7. Early diagnosis of PsA will limit its progression, leading to less joint damage and improvement in the patient’s quality of life.
Our study is not without limitations. The findings are descriptive, and some characteristics may be highly correlated since no statistical adjustments were made. Rheumatology practices collect data for this registry and information on topical therapy for psoriasis or light therapy is not collected. In addition, this is a cross-section of an observational study in which we evaluated the association between change in therapy and change in skin severity and/or joint activity, but it does not evaluate causation. The data source is a North American registry and the results may not be generalizable to others outside the US. Our study population offered little ethnic diversity since most of our patients were White. Moreover, only a small number of patients had reasons for change in therapies, and the follow-up period was only one year. Future studies with a more ethnically diverse population and longer follow-up periods are needed to address these shortcomings.
The clinical implication of our findings suggests a T2T approach, requiring the assessment and incorporation of both skin and joint components, may be advisable. Similar studies can help bolster efforts to educate both patients and providers on the need for serial evaluation of disease activity and changes in therapy until the target disease activity is achieved.
ACKNOWLEDGMENT
Michelle D. Karpman, PhD, (Corrona, LLC) provided scientific writing support.
Footnotes
This study was sponsored by Corrona, LLC. Corrona, LLC has been supported through contracted subscriptions in the last 2 years by AbbVie, Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Crescendo, Eli Lilly and Company, Genentech, Gilead, GSK, Janssen, Momenta Pharmaceuticals, Novartis, Pfizer Inc., Regeneron, Roche, Merck, UCB, and Valeant.
PJM has received research grants from Novartis, AbbVie, Amgen, BMS, Janssen, Eli Lilly, Novartis, Pfizer, SUN, and UCB; consultant fees from Abbvie, Amgen, BMS, Celgene, Corrona, Galapagos, Gilead, Janssen, Leo, Eli Lilly, Merck, Novartis, Pfizer, SUN, and UCB; and speakers bureau fees for AbbVie, Amgen, BMS, Genentech, Janssen, Eli Lilly, Novartis, Pfizer, and UCB. AWA has acted as an investigator, advisor and/or consultant to AbbVie, Janssen, Novartis, Eli Lilly, Regeneron, Sanofi, Leo, Science 37, Modernizing Medicine, and Ortho Dermatologics. TMM, JL, WNM, MJM, and WJH are employees of and hold stock in Eli Lilly. RD and SR are employees of Corrona, LLC. CJE is an employee and holds stock in Corrona, LLC, and is on the advisory board to Merck. JDG is an employee and holds stock in Corrona, LLC, and is a consultant for Genentech, Janssen, Novartis, Pfizer, and Eli Lilly.
- Accepted for publication March 20, 2020.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}