

Abstract
Objective. Enthesitis-related arthritis (ERA) represents a subgroup of juvenile idiopathic arthritis (JIA) that is regularly accompanied by anterior uveitis. This study describes the prevalence and characteristics of ERA-related uveitis.
Methods. Cross-sectional data from the National Pediatric Rheumatological Database (NPRD) were used to characterize ERA-related uveitis (ERA-U). In addition to sociodemographic variables, we documented the occurrence of uveitis and course of disease, including symptoms, visual acuity, and complications, as well as JIA characteristics such as disease activity (Juvenile Arthritis Disease Activity Score 10), functional ability (Childhood Health Assessment Questionnaire score), laboratory variables, and treatment.
Results. In the years from 2002 to 2014, there were 3778 (15.2%) of a total of 24,841 JIA patients recorded in the NPRD who had ERA, and 280 (7.4%) of them had developed uveitis. Detailed ophthalmological documentation by a uveitis add-on module was available for 22.9% of these patients. Uveitis onset was acutely symptomatic in 63% of patients. Patients with uveitis were more frequently male, HLA-B27–positive, younger at ERA onset, and they had higher erythrocyte sedimentation rate values at first uveitis documentation than those without uveitis. Uveitis was diagnosed at a mean age of 11.5 (± 3.9) years (50% within 2 years after ERA onset). Systemic treatment with corticosteroids and synthetic and biologic disease-modifying antirheumatic drugs was associated with a (not significantly) lower risk of developing uveitis.
Conclusion. The course of disease in ERA-U patients is frequently similar to HLA-B27–associated uveitis in adults; however, a subgroup of patients presents with asymptomatic uveitis.
Juvenile idiopathic arthritis (JIA) comprises a heterogeneous group of diseases with chronic arthritis of at least 6 weeks’ duration and onset before the age of 16 years. According to the clinical features at onset, 7 categories of JIA can be distinguished in correspondence with the International League of Associations for Rheumatology (ILAR) classification1. Enthesitis-related arthritis (ERA) is a defined JIA category, which presents with arthritis and/or enthesitis and may also involve the axial skeleton2.
ERA shares many features of spondyloarthritis (SpA), which typically occurs in adults, but may also begin in childhood or adolescence3. However, the initial manifestation of juvenile and adult SpA is often different, with less axial involvement but more frequent inflammation of peripheral joints and entheses in children4. When applying the ILAR criteria for JIA to patients with symptoms of juvenile SpA, the majority is classified as ERA or undifferentiated arthritis4. A common extraarticular manifestation of both SpA and ERA is anterior uveitis (SpA-U, ERA-U). As the literature on pediatric ERA-U is scarce and the disease often resembles SpA-U in the adult population, recommendations for management of ERA-U are frequently derived from what is known from SpA patients.
While disease characteristics and treatment approaches are provided for ERA5, no comprehensive data regarding onset and long-term course of the associated uveitis in childhood and adolescence are available. Previous studies on SpA in adults point to male sex and HLA-B27 as risk factors for uveitis occurrence, which has also been found in children6,7,8.
For adults, the long-term prognosis of HLA-B27-associated uveitis has been found to be relatively good9, while such data are not provided for children. We therefore employed the National Pediatric Rheumatological Database (NPRD) in Germany to describe the clinical course and outcome of uveitis in the ERA patients documented therein.
MATERIALS AND METHODS
Patient data. All patients with ERA recorded in the NPRD between 2002 and 2014 were considered in this analysis. In the NPRD, physician- and patient-reported data are recorded annually by standardized questionnaires. For more details regarding this database, see Supplementary Material (available from the authors upon request) and previously published data7.
The study was approved by the Ethics Committee of the Charité – Universitaetsmedizin Berlin (approval number EA1/044/07). Patients’ and/or parents’ informed consent to participate in the study was obtained according to the Declaration of Helsinki, and the design of the work conforms with the standards currently applied in Germany.
Statistical analysis. Data were analyzed by using the statistics program R (Version 3.2.5). Data were tested for normal distribution by Shapiro-Wilk test. For further analysis, t test, Mann-Whitney U test, chi-square test, Wald test, or ANOVA were applied as appropriate. Logistic regression analyses were applied to identify correlates of uveitis occurrence and correlation between uveitis symptoms and age at onset, as well as arthritis disease duration. Results were expressed as mean and SD, OR, and 95% CI. A significance level of 5% was used for all analyses. Kaplan-Meier analysis was applied to analyze the onset of uveitis as a function of ERA disease duration.
Due to the varying degree of available documentation, different patient groups were used for statistical analysis of different questions as described below. All ERA patients with at least 1 rheumatological documentation were referred to group “ERA”. It was noted whether uveitis had been diagnosed (n = 280 patients with uveitis; group “ERA-U”). Those for whom detailed ophthalmological documentation on uveitis (uveitis module) was available were referred to as the ERA-UM group.
For analysis of the association between treatment and the likelihood of uveitis occurring, 2 groups were selected: systemic treatment in all ERA-U patients (n = 280) was compared to systemic treatment in a selected group of prospectively documented ERA patients (n = 273; “ERA_prosp”) fulfilling the following criteria: no uveitis at baseline documentation and no uveitis development throughout NPRD documentation, duration between ERA onset and baseline of ≤ 1 year, and minimum follow-up documentation of 3 years.
RESULTS
Patient characteristics. Of a total of 24,841 JIA patients enrolled in the NPRD from 2002 to 2014, there were 3778 who had ERA (group “ERA”) and were included in the analysis. Uveitis was diagnosed in 2693 (10.8%) of all JIA patients and in 280 (7.4%; group “ERA-U”) of the 3778 ERA cases. The baseline characteristics of ERA and ERA-U patients are compared in Table 1. ERA-U patients were more frequently male, HLA-B27–positive, and younger at ERA onset, and they had a significantly higher erythrocyte sedimentation rate (ESR) value at initial documentation than ERA patients without uveitis. The mean follow-up documentation period in the NPRD was longer for ERA-U than ERA patients (2.8 ± 2.7 vs 1.4 ± 2.0 yrs, P < 0.001).
Characteristics of ERA patients at first documentation in the National Pediatric Rheumatological Database.
In 64 (22.9%) of the ERA-U patients (group “ERA-UM”), detailed information for uveitis at first and current visit to the attending ophthalmologist was available through the add-on uveitis module. Patients from the ERA-UM group were slightly younger at baseline documentation and the follow-up period documented in the NPRD was longer than for those from the ERA-U group (3.8 ± 3.0 “ERA-UM” vs 2.4 ± 2.6 yrs “ERA-U” without uveitis module, P < 0.0001). As these groups did not differ significantly with respect to sex, age at onset of arthritis, laboratory variables (except for a slightly higher percentage of patients being antinuclear antibody (ANA)–positive in the ERA-UM group), and Childhood Health Assessment Questionnaire and Juvenile Arthritis Disease Activity Score 10 values at baseline, data from those with ophthalmological documentation were considered representative for the uveitis patient group and were utilized for further statistical analysis of the ophthalmological characteristics.
Uveitis onset. Uveitis initially occurred between the ages of 2 and 19 years (mean 11.5 ± 3.9 yrs; Figure 1B). Between 2 and 10 years, uveitis manifestation increased steeply. In 25% of all ERA-U patients, disease onset occurred between 10 and 12 years of age.

Age at uveitis onset. (A) Arthritis onset in patients with or without uveitis. (B) Age at uveitis onset. (C) Duration between arthritis and uveitis onset. ERA: enthesitis-related arthritis.
In more than 20% of ERA-UM patients, uveitis was the initial disease manifestation: In 17.2% and 5.2% of patients, uveitis onset preceded arthritis by 0 to 2 years and by 2 to 4 years, respectively. In the majority of ERA-UM patients, uveitis developed within the first 2 years after arthritis diagnosis; only approximately 10% of patients were diagnosed with uveitis after 4 years of arthritis (Figure 1C). In contrast, Kaplan-Meier analysis of all ERA patients demonstrated a relatively homogeneous risk distribution for developing uveitis during the first 10 years after arthritis onset (Figure 2A). This apparent contrast is due to the analysis of different patient collectives: Using a right-censored model for Kaplan-Meier analysis, the number of patients available for analysis drops markedly due to the relatively large percentage of short-term documentation (Figure 2B), whereas the relative portion of those developing uveitis is rather stable. In contrast, the ERA-UM subgroup consists of selected uveitis patients with a detailed, but also mostly short-term, ophthalmological documentation and disease characteristics differing slightly from those of the ERA group.
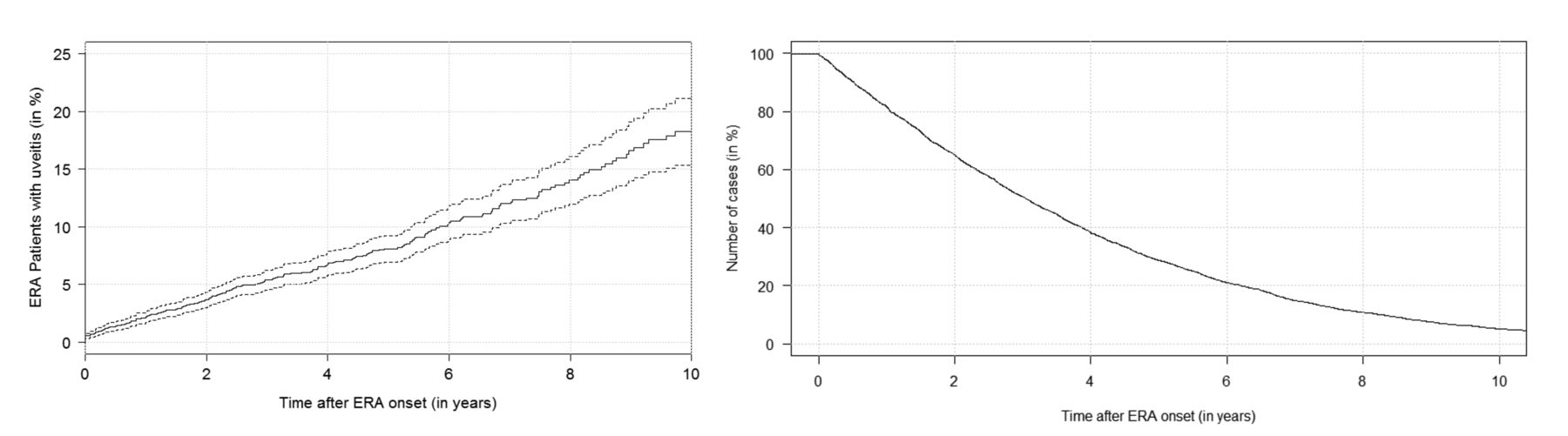
Risk of uveitis development in patients with ERA. Continuous line: risk for uveitis development (mean); dashed lines: 95% CI. ERA: enthesitis-related arthritis.
The likelihood of developing uveitis was associated with a young age at ERA onset: In children aged ≤ 10 years at arthritis onset, the risk of developing uveitis was 9.2%, whereas the likelihood was 6.9% in those with ERA onset after 10 years of age (P = 0.014). ANA status was similar between those patients aged younger or older than 10 years at ERA onset (ANA+ 75.4%, ANA– 76.1%). Patients with ERA onset before 10 years of age were more frequently HLA-B27–positive (40.5% vs 34.6%, P = 0.0007).
Uveitis characteristics. Clinical characteristics of uveitis were analyzed in the ERA-UM group (n = 64). In 63%, symptomatic onset of uveitis flares was documented. A correlation between symptomatic uveitis and higher age at arthritis onset was observed (OR 1.23, 95% CI 1.03–1.48, P = 0.025), whereas no statistically significant correlation was found between ERA disease duration and uveitis symptoms (OR 0.9, 95% CI 0.71–1.15, P = 0.41). Clinical data of patients with symptomatic and asymptomatic uveitis are displayed in Table 2. In the majority of cases (83%), uveitis was unilateral during the course of disease. Uveitis was classified most frequently as anterior uveitis (88%) and less frequently involved primarily the posterior eye segments (12%). The course of uveitis episodes after initial manifestation was acute in the majority of patients (46%, with sudden onset and limited duration), recurrent (28%, repeated episodes separated by periods of inactivity without systemic and topical treatment ≥ 3 months in duration), or chronic (25%, persistent uveitis with relapse in < 3 months after discontinuing systemic and topical treatment).
Characteristics of uveitis patients with symptomatic and asymptomatic onset of flare.
Ocular complications had already developed in 44% at the initial visit (Table 3), and the mean visual acuity was 0.19 logMAR (± 0.33 SD) at baseline and 0.17 logMAR (± 0.32 SD) at last documentation. In 1 patient, best corrected visual acuity (BCVA) was hand movements and counting fingers in 1 eye on all visits documented, which would mean legal blindness in this eye.
Visual acuity and uveitis complications.
Course of disease in relation to HLA-B27–negative and ANA status. As a relatively high number of patients reported asymptomatic uveitis onset, and the clinical entity of acute anterior uveitis has been previously linked to the presence of HLA-B2710, we analyzed disease characteristics in relation to HLA-B27 status in the ERA-UM group. Of those patients, 2 were both ANA- and HLA-B27–negative, 6 were ANA-positive and HLA-B27–negative, 23 were HLA-B27–positive and ANA-negative, and 9 were both ANA- and HLA-B27–positive. The frequency of symptomatic uveitis onset was somewhat, but not significantly, higher in HLA-B27–positive patients [symptomatic onset in 74% (32 out of 43)] than in those who were HLA-B27–negative [44.4% (4 out of 9); P = 0.17]. ANA-positive patients more frequently had asymptomatic uveitis [43% (6 out of 14 ANA-positive patients)] than ANA-negative patients [9% (2 out of 22 ANA-negative patients); P = 0.05). The frequency of complications at disease onset did not differ significantly depending on HLA-B27 or ANA status (e.g., positive or negative; however, mean BCVA at onset differed depending on the presence of HLA-B27 [0.3 logMAR (± 0.44 SD) in HLA-B27–positive vs 0.14 (± 0.4 SD) in HLA-B27–negative patients, P = 0.05], but not with ANA status.
To identify the influence of HLA-B27- and ANA-positivity on the occurrence of uveitis, we performed a multivariate survival analysis of all ERA patients. We applied the Cox proportional hazard model [variables: sex, HLA-B27 positivity, ANA positivity, age at ERA onset (metric scale; HR as a function of risk per yr)] with right-censored event times. Here, we could identify the presence of HLA-B27 (HR 1.77, 95% CI 1.27–2.45, P < 0.001) and age at ERA onset (HR 1.11, 95% CI 1.06–1.16, P < 0.0001) as independent risk factors, whereas the risk for development of uveitis was not influenced by ANA status (HR 1.27, 95% CI 0.92–1.75, P = 0.149) or sex (HR 1.25; 95% CI 0.92–1.69, P = 0.156).
Initial treatment of the ERA-U group. Data from 280 ERA-U patients documenting medical treatment during the 12 months prior to and at NPRD baseline documentation were available for analysis. Indication for treatment (medication given for uveitis or arthritis) was not reported and could not be considered for analysis. At baseline documentation and during the previous 12 months, 76% (n = 213) of ERA-U patients had been treated with nonsteroidal antiinflammatory drugs (NSAID), 33% with oral low-dose corticosteroids (< 0.2 mg/kg body weight, n = 91), 15% with oral high-dose corticosteroids (≥ 0.2 mg/kg body weight, n = 42), and 9% with corticosteroid pulse therapy (10–30 mg/kg body weight methylprednisolone IV for 3 days, n = 24). Methotrexate (MTX) was used in 51% (n = 142), followed by sulfasalazine (SSZ; 27%, n = 76) and cyclosporine A (8%, n = 23). Within the group of biological disease-modifying antirheumatic drug (DMARD), etanercept (ETN; 21%, n = 58) and adalimumab (ADA; 13%, n = 36) had been given already before and/or at baseline documentation.
Therapy prior to and after uveitis manifestation. We then analyzed therapeutic strategies at initial study documentation and at the first documentation after uveitis manifestation in the ERA-UM group (Table 4). With uveitis manifestation, the use of NSAID decreased, whereas corticosteroids and biologics were given more frequently.
Systemic medication at initial documentation and after uveitis manifestation.
Local medical treatment. Local treatment was analyzed in the ERA-UM group. At initial documentation with the uveitis module (mean time between initial manifestation of uveitis and documentation 2.31 ± 2.41 yrs), topical therapy consisted of corticosteroids (47%), cycloplegics (24%), NSAID (11%), or antiglaucomatous agents (7%). Another 33% of the patients did not receive any local therapy at initial documentation, while local treatment was not documented in 20%. At any time during the entire follow-up documentation, 93% of patients were treated with topical corticosteroids, NSAID (26%), cycloplegics (72%), or antiglaucomatous agents (14%). In all, 14% received subconjunctival or parabulbar corticosteroid injections.
Surgery. At first uveitis documentation, 6 surgical interventions had already been performed for uveitis complications (cataract surgery, n = 3; glaucoma surgery, n = 2; and vitrectomy, n = 1). The number of surgical interventions that had been performed by the time of the last available ophthalmological follow-up documentation increased to n = 13 [cataract, n = 7 (n = 6 with intraocular lens implantation); vitrectomy, n = 1; glaucoma surgery, n = 3; and other procedures n = 2].
Effect of systemic therapy on uveitis occurrence. To determine the association of systemic therapy with the likelihood of uveitis, therapeutic strategies in the ERA-U group (n = 280) and an incident and prospectively observed ERA group (ERA_prosp) without ocular involvement (n = 268) were analyzed.
DMARD treatment was associated with a reduced risk for developing uveitis; however, only trends, none of them significant, were observed: Corticosteroid intake decreased the OR for developing uveitis (< 0.2 mg/kg: OR 0.78, 95% CI 0.41–1.49; ≥ 0.2 mg/kg: OR 0.41, 95% CI 0.14–1.21; steroid pulse therapy: OR 0.33, 95% CI 0.09–1.26). Among the cDMARD, MTX (OR 0.75, 95% CI 0.46–1.22) and SSZ (OR 0.89, 95% CI 0.53–1.51) decreased the risk for uveitis onset. Regarding biological DMARD therapy, ETN, given as monotherapy (n = 5 ERA-U patients and n = 6, ERA_prosp) or combined with MTX (n = 3 ERA-U patients and n = 5 ERA_prosp) decreased the risk for uveitis manifestation (OR 0.53, 95% CI 0.21–1.37); however, this finding was not significant and the patient groups receiving this medication were very small. NSAID treatment did not decrease but rather increased the risk for developing uveitis (OR 1.76, 95% CI 1.04–2.99); this was the only significant effect observed.
The numbers of patients receiving other medications (azathioprine, leflunomide, cyclosporine, and ADA) were too low to obtain meaningful results and were therefore not analyzed.
DISCUSSION
About 10–20% of JIA patients are diagnosed with ERA5,11, and disease characteristics of uveitis associated with ERA are assumed to be different from those of oligoarthritis-associated uveitis; however, little is known about the clinical course of ERA-associated uveitis in children and adolescents. Recommendations for management of this uveitis entity are derived either from uveitis associated with other JIA subtypes or from (mostly HLA-B27–related) acute anterior uveitis of patients with SpA in adulthood. We therefore analyzed disease characteristics of juvenile patients with ERA-U, which were followed in the context of a large JIA cohort: the German NPDR.
Frequency of uveitis in this cohort was in line with previously published data on children with ERA, as were the numbers of ERA patients in whom HLA-B27 or ANA were detected5,12,13. Younger age at ERA onset was associated with uveitis development, as it is well established for the JIA population in general11,14,15, and has also been demonstrated especially for the subgroup of ERA patients previously13. In their inception cohort, Saurenmann, et al found a significant increase in risk for development of uveitis in those ERA patients who were ANA-positive and female13, an association which was not found in our patients, although demographic data regarding frequency of uveitis in ERA patients, age at ERA and uveitis onset, and numbers of patients being ANA-positive were similar. In our cohort, children with ERA-U were more frequently male and HLA-B27–positive than those without uveitis manifestation, and they presented with more pronounced systemic inflammatory activity at baseline documentation, as indicated by a higher ESR. Previously, HLA-B27–positive ERA patients were found to have acute anterior uveitis more frequently than those who were HLA-B27–negative16. The predominance of the male sex and HLA-B27 positivity among patients with uveitis has also been described in SpA-associated disease17 and are distinguishing features of ERA, in contrast to oligo- or rheumatoid factor–negative, polyarthritis-related uveitis that is seen more frequently and where the female sex and ANA positivity predominate and HLA-B27 is not an independent risk factor8,18. Further, our finding regarding ESR elevation is similar to what Haasnoot, et al18 demonstrated for a subset of children with JIA oligo- and polyarthritis and was also found in a German inception cohort of JIA children, where both ESR and S100A12, another marker of systemic inflammation, were shown to be associated with an increased risk for developing uveitis11. The mean ESR levels measured here were lower than those documented in the other 2 studies11,18, which is probably due to the fact that the ESR levels were determined at or at least close to JIA diagnosis and ours were measured at study inclusion with the majority of patients already being treated with systemic antiinflammatory medication. Previously, ESR has also been identified as a risk factor for relapses of HLA-B27–associated anterior uveitis19.
Previous studies have disclosed a reduced risk for developing uveitis and for a more favorable disease course in JIA patients treated with DMARD, namely with MTX, and a combination therapy with ETN or ADA11,20. We were not able to demonstrate a statistically significant effect in our cohort, but can only report a trend toward risk reduction in our patients. Treatment with NSAID was (significantly) associated with an increased risk for developing uveitis. Given the fact that the majority of ERA patients are initially treated with NSAID therapy only12, this might require some reconsideration if future studies confirm our findings. As we were not able to conduct a multivariate analysis investigating the potential effect of other risk factors for uveitis development, we cannot say whether NSAID treatment is an independent risk factor or is correlated with other clinical characteristics accounting for the effect observed. It might as well be that those patients treated with NSAID monotherapy were influenced by other factors including disease activity, age group, HLA-B27 or ANA status, etc. However, given what is already published on the protective effect of early DMARD treatment11,20, it is tempting to speculate that the same is true for ERA-related uveitis. Prospective studies will be needed to clarify this situation.
Given the frequently cited assumption that ERA-associated uveitis “typically” presents with acute symptoms21,22,23, resembling the course observed in SpA, we were somewhat surprised to find that this was not the case in almost 40% of ERA patients documented here. The occurrence of both SpA and ERA is typically associated with the HLA-B27 allele, which therefore constitutes one of the diagnostic criteria. Uveitis in HLA-B27–positive patients (regardless of presence or absence of a systemic disease) is a well-characterized clinical entity, which is typically acutely symptomatic in onset, manifesting with redness, pain, and photophobia24. As the vast majority (> 90% of white and 60% of African Americans) with SpA are HLA-B27–positive24, this represents the most predominant uveitis type and was documented in almost 90% of all SpA patients with uveitis in a metaanalysis of 29,877 SpA cases within 126 publications25. However, the percentage of ERA patients in whom HLA-B27 can be detected varied immensely (45–88%)5 and only amounted to about 60% in our cohort, which is in line with previous findings5. Taking into account that the risk for a symptomatic, acute onset of uveitis flares seems to be related to the HLA-B27 allele according to both the data presented here and previous literature17, and the fact that almost 40% of patients in this study reported insidious uveitis onset, suggests that the management of these patients might require some reconsideration. Indeed, the ophthalmological screening schedule for JIA patients currently employed in Germany recommends yearly examinations in ERA7, assuming that these patients characteristically experience acute symptoms of flare onset, prompting immediate ophthalmological consultation. Meanwhile, the British guidelines suggested a 3- to 4-monthly screening of children diagnosed with ERA26, similar to what is recommended for patients with other JIA subtypes, for which onset of the vast majority of uveitis cases is insidious7,26. Regarding the results from the large cohort in the present study, this approach is probably more appropriate, especially in children younger than 10 years at ERA onset, as those children had a particularly high risk for developing uveitis in our cohort.
According to the data presented here, ERA-associated uveitis does indeed share some clinical features of the disease course considered to be characteristic for HLA-B27–positive SpA patients, as one might assume due to the many overlapping rheumatologic characteristics of (juvenile) SpA and ERA. However, certain findings resemble those observed in uveitis associated with other JIA subtypes, so that ERA patients may benefit from similar screening schedules. Prospective studies employing both detailed ophthalmological documentation and biomarker monitoring with a focus on ERA patients are required to outline the similarities and differences of the diverse uveitis forms in JIA in order to improve our understanding of pathophysiological concepts and optimize patient management.
ACKNOWLEDGMENT
The authors thank Britta Stratmann and Beatrix Zurek-Imhoff for support with data acquisition.
Footnotes
↵Dr. K. Walscheid and Dr. K. Glandorf contributed equally to this study.
KW has received a DFG grant (WA 4449/2-1) and honoraria from Novartis.
KM is funded by the Rheumastiftung and has received research grants from BMBF (FKZ, 01ER1504A), Pfizer, AbbVie, and Roche, and honoraria from AbbVie, Biermann, GSK, Medac, Sanofi. AH has received research grants from BMBF (FKZ, 01ER1504C), DFG (He 1877/19-1), Pfizer, and Novartis, and honoraria from AbbVie, Biermann, Alimera Sciences, Allergan, MSD Sharp and Dohme, Pfizer, Santen, and Xoma.
- Accepted for publication March 6, 2020.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}
{kind=link}