

To the Editor:
Psoriatic arthritis (PsA) is a chronic inflammatory arthritis that affects almost one-third of patients with psoriasis. PsA is a relatively common inflammatory condition in rheumatology clinics. In fact, a recent epidemiological study raised the prevalence of PsA to almost 0.6% in the general population in Spain.1
PsA presents multiple musculoskeletal and cutaneous manifestations that should be adequately represented in disease activity assessment tools. Also, it is important that these tools address how PsA affects patients’ lives, as seen in such tools as the PsA Impact of Disease (PsAID) questionnaire, an instrument promoted by the European Alliance of Associations for Rheumatology and recently endorsed by the Group for Research and Assessment of Psoriasis and PsA to assess the quality of life (QOL) in PsA.2,3 On the other hand, the Assessment of SpondyloArthritis international Society Health Index (ASAS HI) is a more generic disease impact instrument, initially designed for axial spondyloarthritis (axSpA), and very recently also applied in PsA.4,5 Both impact instruments capture similar but also different aspects in PsA, so it would be of interest to compare their clinimetric properties in this population.
In the present work, we have determined which items of the ASAS HI may explain a higher value of the PsAID-12, and therefore a greater impact on the QOL of these patients.
We carried out a posthoc analysis of a previous study in which we tested the construct validity of the ASAS HI in patients with PsA.5 The methodological details, results, and ethical considerations of that study have been published elsewhere.5 The study included 90 consecutive patients with PsA (median age 53 [IQR 45–65], 52 males:38 females, and median disease duration of 16 [IQR 10–29] yrs for psoriasis and 7 [IQR 3–14] yrs for arthritis). We previously found a high correlation between PsAID and ASAS HI (r = 0.75, 95% CI 0.64–0.83).5 Therefore, we carried out an analysis on the ASAS HI items that could explain higher PsAID values as well as a state of high-disease impact (PsAID > 4).
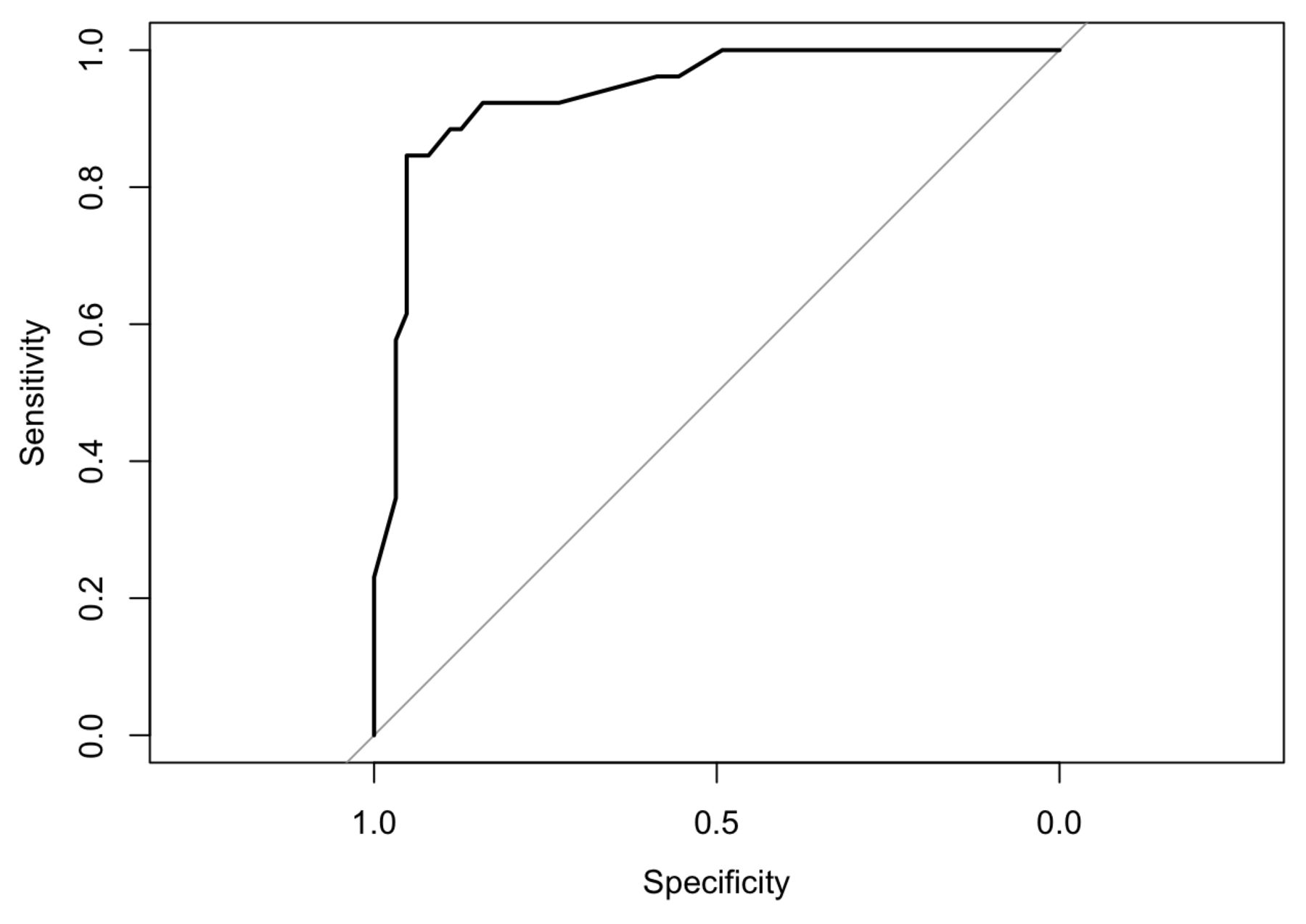
The ASAS HI items significantly associated with higher PsAID scores are presented in Table 1. The ASAS HI items associated with PsAID > 4 (high impact) according to Firth logistic regression were as follows: #2, “I find it hard to stand for long” (OR 4.9, P < 0.05); #5, “I am often exhausted” (OR 6.5, P < 0.05), #13, “I often get frustrated” (OR 5.02, P < 0.05); #16, “I sleep badly at night” (OR 7.1, P < 0.05); and #17, “I cannot overcome my difficulties” (OR 6.9, P < 0.05). To define the best predictive model of a high-impact PsAID based on the ASAS HI components, a backward elimination based on penalized likelihood ratio test was used. An ASAS HI > 5 identified patients in the high-impact PsAID category with an area under the receiver-operating characteristic curve (AUC) of 0.94 (95% CI 0.88–0.99, P = 0.007; Figure 1).
Spearman estimate coefficients between the different components of the ASAS HI and PsAID.
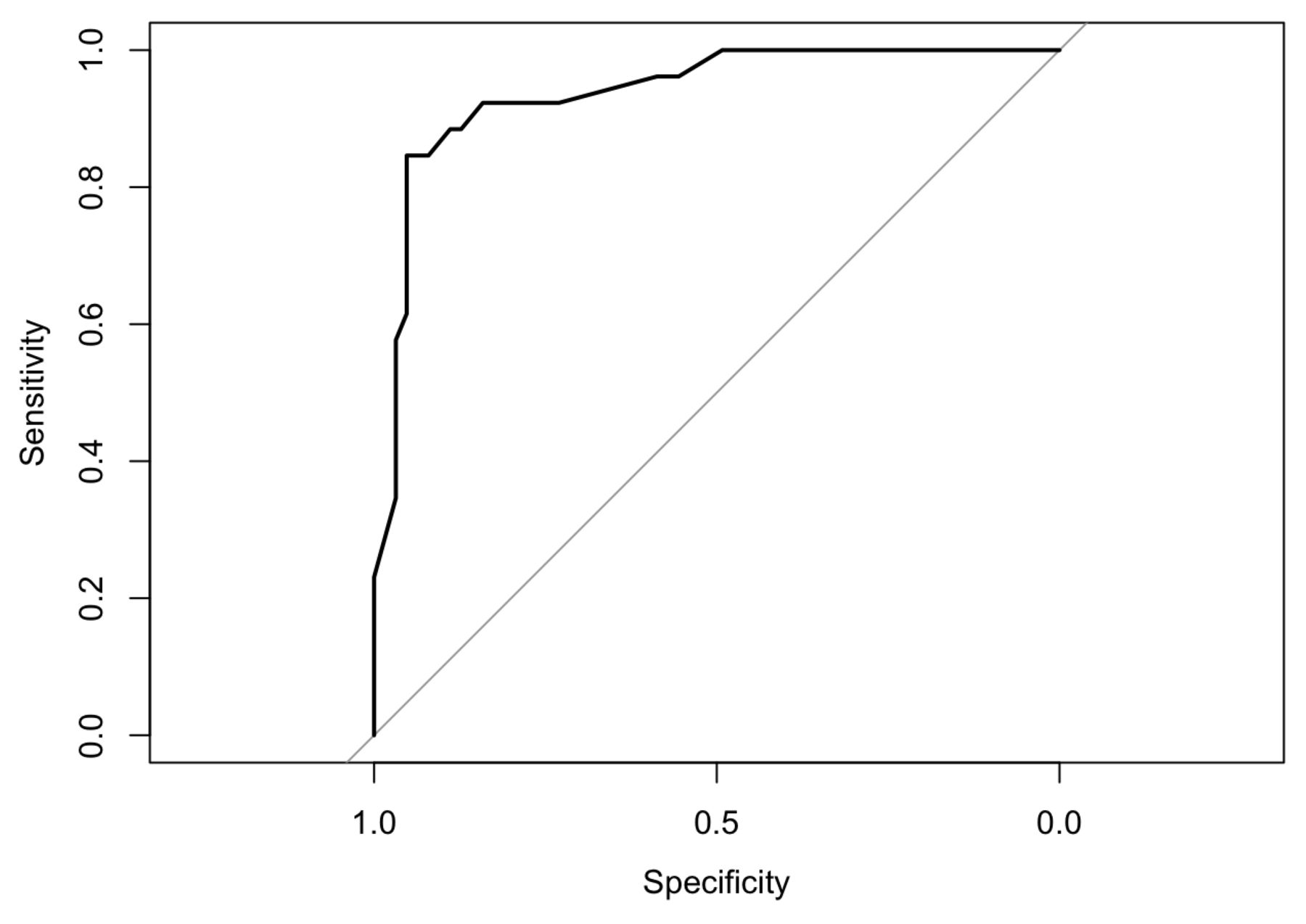
The optimal cut-off for the ASAS HI to identify a high-impact PsAID (> 4) turned out to be a value of 5.3 according to the maximum efficiency criterion (AUC 0.94, 95% CI 0.88–0.99, P = 0.007). ASAS HI: Assessment of SpondyloArthritis international Society Health Index; AUC: area under the receiver-operating characteristic curve; PsAID: Psoriatic Arthritis Impact of Disease.
In this study, the ASAS HI components that significantly contributed to a higher mean PsAID score were #2, #4 (“I have problems using toilet facilities”), #5, #8 (“I have difficulty operating the pedals in my car”), #13, #16, and #17, whereas only one of them (#10, “I am not able to walk outdoors on flat ground”) was associated with lower mean scores with this instrument. The predictive model with the best sensitivity and specificity associated an ASAS HI > 5 with a high-impact PsAID.
It is not uncommon for estimates of activity informed by physicians and patient-reported outcome measures to be inconsistent.6,7 Therefore, it is beneficial to know which disease factors determine the impact of the disease. Thus, it has been seen that both joint and skin activity, together with fibromyalgia, influence PsAID values in patients with PsA.8 However, in our study, item #1 of the ASAS HI, referring to pain (“pain sometimes disrupts my normal activities”), had a lesser impact on PsAID values compared to other items related to sleep, fatigue, and physical and psychological aspects.
Both ASAS HI and PsAID could be used as disease impact estimators, although they are instruments with differential aspects.2,4 Thus, the cutaneous domain is not represented in the ASAS HI, whereas the patient’s sexuality is not represented in the PsAID.2,4 This last domain, for example, is usually more affected in patients with PsA than with axSpA.9 Moreover, the ASAS HI cut-off value of 5 found in our study shows some parallelism with cut-off values linked to the activity of axSpA in other studies.10 All of this indicates that both the ASAS HI and the PsAID could be used for a more accurate estimate of the true effect of PsA on patients’ lives.
Our study is limited by the relatively small number of patients, because it is a point estimate of a disease that tends to exhibit phenotypic changes over time, and because it does not include the entire spectrum that psoriatic disease can display. Therefore, it is necessary to expand the number of studies evaluating ASAS HI in PsA.
Together with the PsAID, the ASAS HI could be used to evaluate disease impact in PsA. An ASAS HI < 5 could constitute a good treatment objective, although more information is required on the sensitivity to change of this questionnaire in PsA.
Footnotes
The authors declare no conflicts of interest relevant to this article.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}