

Abstract
Objective While opioids are known to cause unintended adverse effects, they are being utilized by a number of patients with osteoarthritis (OA). The aim of this study was to evaluate the association of patient familiarity and perceptions regarding efficacy and risks with opioid medication use for OA.
Methods A total of 362 adults with knee and/or hip OA were surveyed in this cross-sectional study. Patients’ familiarity with and perceptions of benefits/risks of opioid medications were measured to evaluate potential associations with the utilization of opioid medications for OA within the last 6 months. Logistic regression models were adjusted for sociodemographic and clinical variables.
Results In this sample, 28.7% (100/349) reported use of an opioid medication for OA-related symptoms in the last 6 months. Those who were on an opioid medication, compared to those who were not, were younger (mean age 62.5 vs 64.8 yrs), were more likely to have a high school education or lower (48.0% vs 35.3%), and had higher mean depression (Patient Health Questionnaire [PHQ]-8 7.2 vs 4.9) and OA-related pain (Western Ontario and McMaster Universities Arthritis Index [WOMAC] 54.8 vs 46.8) scores. After adjustment for sociodemographic and clinical variables, the following were associated with opioid medication use: higher perception of medication benefit (OR 1.68, 95% CI 1.18–2.41), lower perception of medication risk (OR 0.67, 95% CI 0.51–0.88), and having family or friends who received the medication for OA (OR 3.88, 95% CI 1.88–8.02).
Conclusion Among adults with knee/hip OA, opioid use was associated with being familiar with the treatment, as well as believing that the medication was beneficial and low-risk.
Osteoarthritis (OA) is the most common form of arthritis, and disease management includes pain control and functional improvement.1,2 Exercise, physical therapy, acetaminophen, and nonsteroidal antiinflammatory drugs (NSAIDs) are considered first-line treatments.1,2 Initial nonpharmacologic and pharmacologic OA therapies may be insufficient to control the symptoms, however. Pain-relieving effects of NSAIDs and acetaminophen (paracetamol) can be small and short-lasting.2,3 Prescription of NSAIDs may not be appropriate due to drug intolerance and/or the presence of particular comorbidities (e.g., gastrointestinal bleeding history). Joint replacement surgery may be an option among those with severe disease.1,2 However, those with multiple comorbidities may be poor surgical candidates, and some patients have a preference against surgery.4 The 2019 American College of Rheumatology/Arthritis Foundation guidelines conditionally recommend against the use of nontramadol opioid agents in patients with knee and/or hip OA.1 However, the guidelines acknowledge that opioids may be used under certain instances, particularly when alternative therapies have failed or are contraindicated.
Indeed, opioids have been increasingly used to treat chronic pain conditions, including those caused by musculoskeletal (MSK) disorders, in the United States and worldwide.5,6 From 2001 to 2010, opioid prescribing in the US for acute and chronic MSK pain visits increased by 50% and 79%, respectively.5 In a recent study, there was an observed decrease in the use of opioids between 2013 and 2016 among men and those who were less educated; however, there was a significant overall increase in opioid use from 1999 to 2016.7 In Sweden from 2013 to 2015, the 1-year prevalence of opioid use among patients with OA was 24%, 2-fold higher compared to those without OA.8 Yet, opioid medications can cause nausea, constipation, drowsiness, and vomiting.9 The chronic use of opioids has been associated with increased risk for fractures, cardiovascular events, and greater mortality.10 There is also concern regarding the dangers of opioid dependence and overdose.11 In response to the opioid epidemic crisis, rheumatologists have advocated for the use of alternate methods of pain control and the focus on the treatment of concomitant psychiatric diseases.12
With recognition of the necessity to minimize potential risks while maintaining adequate pain management among OA patients with chronic pain, there is a need to understand factors that are associated with the use of opioids for OA-related symptoms.13,14,15,16,17 Younger age, female sex, white race, depression, and greater OA disease severity have all been associated with opioid use.13,14,15,18,19 In addition, patient-level factors such as attitudes and beliefs about treatment options may influence treatment choices. Patient familiarity and perceptions about nonpharmacologic treatments have been associated with utilization of exercise and joint replacement surgery for OA.20,21,22 Yet, the potential association of these patient-level factors with utilization of opioids for OA is poorly understood. While many of the known determinants of opioid use are relatively immutable, patient familiarity and perceptions about medications are also modifiable at the point of care.23
The primary objective of this study was to investigate the association of familiarity, perceived benefits, and perceived risks with opioid medication use for OA treatment, controlling for patient demographics and clinical characteristics. The secondary objective was to examine the association of demographic factors with familiarity, perceived benefits, and perceived risks of opioid use for OA.
METHODS
Setting and participants. Participants for this cross-sectional study were recruited from the University of Arizona Arthritis Center research registry and Banner University Medical Center (BUMC) Rheumatology, Orthopedic Surgery/Sports Medicine, and Internal Medicine Clinics located in Tucson, Arizona, from July 2015 through April 2018. The target sample included patients with knee or hip OA. A diagnosis of knee OA was confirmed by radiographic evidence of OA, presence of chronic frequent knee pain, and age ≥ 50 years.24 A confirmed diagnosis of hip OA depended on the presence of hip pain and femoral and/or acetabular osteophytes on radiograph.25 The presence of chronic frequent pain due to knee or hip OA was evaluated according to questions from the arthritis supplement of the National Health and Nutrition Exam Survey.26,27 Patients with any of the following diagnoses were excluded: disease associated with inflammatory arthritis (e.g., rheumatoid arthritis), total hip and knee arthroplasty history, or moderate to severe cognitive dysfunction.
Screening and recruitment. Medical records and the University of Arizona Arthritis Center research registry were reviewed to identify patients with knee and/or hip OA. Patients were then screened by telephone to evaluate eligibility. Those who were eligible and willing to participate in the study subsequently consented and were given a questionnaire to complete on-site. They were given a private room where they individually filled out the paper survey by themselves, without assistance. They were also offered the option to complete the survey at home and return it by mail. English and Spanish language versions of surveys were offered.
Primary study outcome. The primary study outcome was opioid medication use for treatment of pain from OA within the last 6 months. Participants were asked if they “used or participated” in various different “treatments for joint pain of arthritis in the last 6 months.” Treatment options included “strong pain medications you get with a prescription, including opioids such as morphine (MS Contin, Astramorph, Duramorph), acetaminophen with codeine (Tylenol with codeine #3), or hydrocodone with acetaminophen (Vicodin, Lorcet, Lortab).”
Familiarity with opioid medications for OA treatment. Participants’ familiarity with opioid medications as treatment for OA was determined by asking if they (1) have heard of it as OA treatment, (2) have family or friends who received it for treatment, and (3) have a good understanding of what happens after treatment. Response options for all questions were yes or no. There were items used in previous studies20,28 but modified to measure familiarity with opioid medications for OA.
Perceptions of benefit and risk of opioid medications. Perceived benefit and risk of opioid medications were assessed using previously used measures of perceived benefit (4-item) and risk (3-item) of joint replacement surgery,21 but adapted for opioids. The perception of benefit was measured by determining the extent to which participants believed that an opioid medication treatment (1) was beneficial for people with arthritis, (2) was beneficial for them, (3) could lead to pain relief, and (4) could cause functional improvement. The perception of risk was measured by determining the extent to which participants (1) believe in the risk/danger with (very harmless to very harmful); (2) believe in serious complications with (not at all to very serious); and (3) showed concern for potential complications from opioid medication treatment use (not at all to very concerned). Possible ordinal responses ranged from 1 to 5 for each question. Responses to each set of questions were averaged to obtain a scale of 1 to 5, with higher values indicating greater perception of benefit/risk. Both perceived benefit and perceived risk of opioid medication measures had good internal reliability scores (Cronbach α = 0.8250 and 0.8517, respectively).
Sociodemographic covariates. The following were included as covariates: age, sex, race, ethnicity, educational attainment, employment, marital status, household income, and medical insurance.
Clinical covariates. Quality of life was assessed using the following question: “How would you rate your overall quality of life?”, which was scored on a 5-point ordinal scale ranging from poor to excellent.29 Depression was assessed using the Patient Health Questionnaire-8 (PHQ-8, range 0–24).30 Medical comorbidity was assessed using a modified self-reported Charlson Comorbidity Index.31 Health literacy was determined by asking, “How confident are you filling out medical forms by yourself ?”32 Study participants were dichotomized between those with adequate (extremely, quite a bit) vs inadequate (somewhat, a little bit, or not at all) health literacy. OA-related disease severity was measured using the 24-item Western Ontario and McMaster Universities Arthritis Index (WOMAC).33 The WOMAC has 3 subscales: pain, stiffness, and disability. Each subscale score was normalized to a range from 0 to 100.
The full study protocol was approved by the University of Arizona Institutional Review Board (#1502663769) and was previously described.20,34
Statistical methods. Demographic information, clinical characteristics, and psychosocial variables were compared by opioid treatment group using a 2-sided Fisher exact test or chi-square test for categorical variables, and 2-sided t test for continuous variables.
Familiarity with opioid medication statements were compared by opioid treatment group and by various sociodemographic characteristics using a 2-sided Fisher exact test or chi-square test. Perceived benefit and risk of opioid medications were also compared by the same variables using a 2-sided t test.
A logistic regression model was used to estimate the adjusted OR of using an opioid medication, comparing participants by levels of perceived benefit and perceived risk of opioid medicines and by familiarity with opioids. The model was adjusted for age, sex, race (White vs not), education, PHQ-8 (depression) score, and WOMAC total score. All demographic (age, sex, race, education, income) and clinical variables (quality of life, OA disease severity, number of comorbidities, depression) that were previously associated with opioid medication use in other OA studies were considered as covariates.13,14,15,16,17 Income was considered but dropped from the model due to significant overlap with education. To account for missing data, multiple imputation using chained equation was used to build the multivariable model.35
Analyses were performed using STATA IC 16.0 (StataCorp).
RESULTS
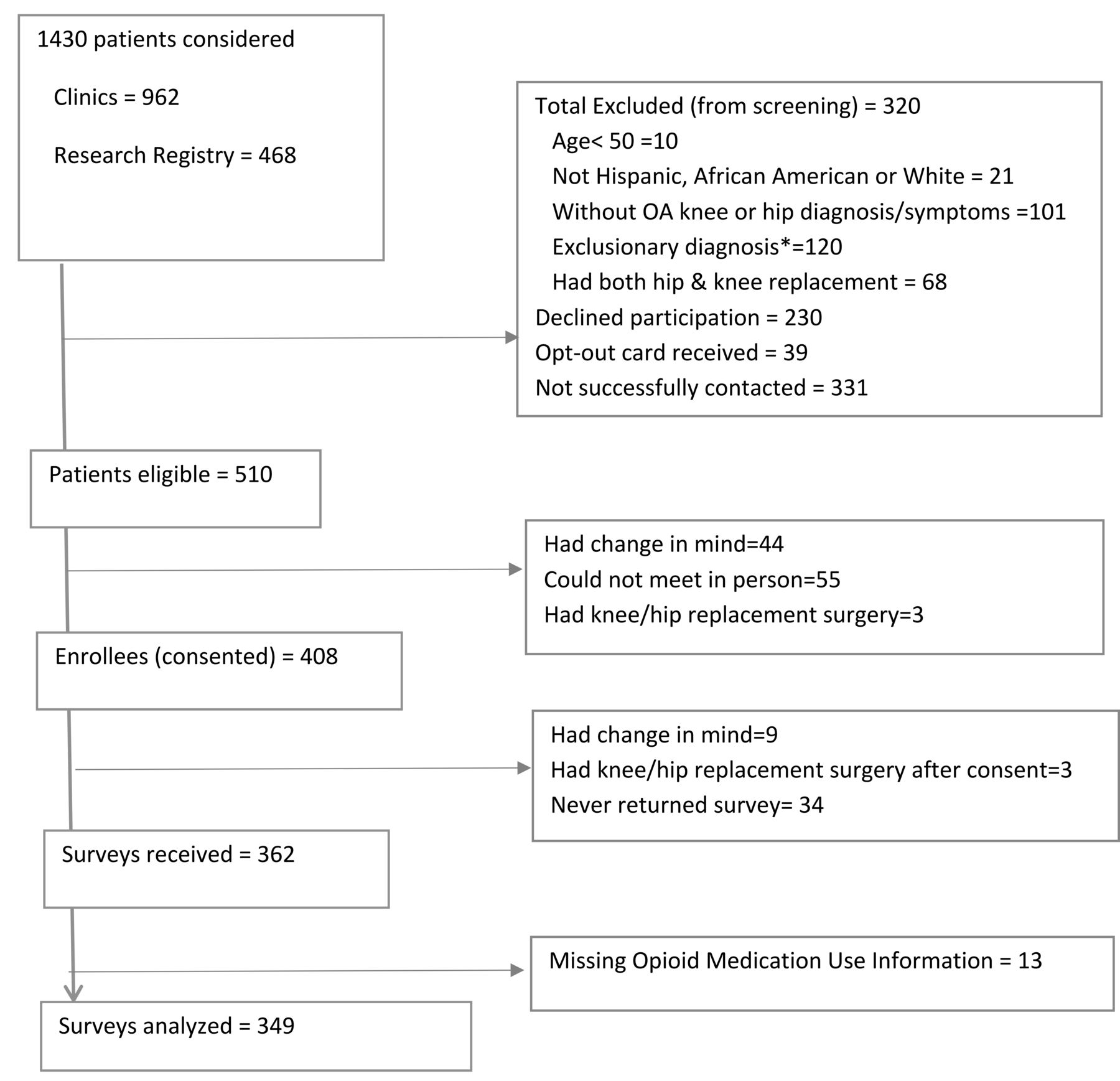
Among the 1430 considered for study eligibility, 320 were excluded during screening, 269 declined study participation (prior to screening), and 331 could not be contacted. A total of 510 were deemed eligible for the study, and 408 consented to participate (Figure 1). Among those who consented, 34 never returned a survey, and 12 changed their mind about participating or had subsequent joint replacement surgery. Overall, 362 surveys were received, but 13 had missing opioid medication use information and were therefore excluded.

Study flowchart. * Exclusionary diagnoses: rheumatoid arthritis, systemic lupus erythematosus, seronegative spondyloarthropathy, gout, pseudogout, senile dementia, vascular dementia, alcohol-induced dementia, drug-induced dementia. OA: osteoarthritis.
Sociodemographic and clinical characteristics by treatment use. A total of 100 study participants out of 349 were on an opioid medication for OA in the last 6 months. Those who had used an opioid medication, compared to those who had not, were younger (mean age 62.5 vs 64.8, P = 0.02), but the 2 medication treatment groups did not significantly differ by sex, race, or ethnicity (Table 1).
Patient sociodemographic and clinical characteristics by opioid medication use in the last 6 months.
Having a high school education or lower (48.0% vs 35.3%, P = 0.01), not having full-time employment, and a household income of < $20,000 per year (52.0% vs 28.5%, P = 0.001) were more common among those who were on an opioid medication compared to those who were not (Table 1). Having Medicaid insurance was also more common among those who had used an opioid medication compared to those who had not (33.0% vs 14.9%, P = 0.003). Neither marital status nor having other types of medical insurance differed by opioid medication treatment group (Table 1).
Those who had used an opioid medication for OA, compared to those who had not, were more likely to report having only fair or poor health (31.0% vs 13.7%, 7.0% vs 6.0%, respectively, P < 0.001), had a higher number of comorbidities (mean 4.1 vs 3.2, P < 0.001), and had higher PHQ-8 scores (mean 7.2 vs 4.9, P = 0.002). Mean WOMAC pain and disability scores were also higher among them compared to those who were not on an opioid medication for OA (54.8 vs 46.8, P = 0.002; 56.6 vs 44.9, respectively, P < 0.001).
Knowledge and attitudes about opioid medications. Study participants who were on an opioid medication for OA had greater familiarity with opioid medications than those who were not on the medication in the last 6 months (Table 2). They were more likely to have heard of its use for OA (95.9% vs 71.4%, P < 0.001), to have family or friends who received it for OA (77.4% vs 40.4%, P < 0.001), and to have a good understanding of the consequences of its use (92.2% vs 64.7%, P < 0.001). They also had higher perceived benefit (mean 3.9 vs 3.3, P < 0.001) and lower perceived risk (mean 3.2 vs 3.8, P < 0.001) of taking opioid medications for OA. After adjustment for age, sex, race, education, PHQ-8 score, and WOMAC total score, odds of opioid medication treatment use remained significantly higher among those with higher perceived medication benefit (OR 1.68, 95% CI 1.18–2.41) or had family or friends who received the medication for OA (OR 3.88, 95% CI 1.88–8.02). Odds of opioid medication treatment use were lower among those who perceived greater medication risk (OR 0.67, 95% CI 0.51–0.88; Table 3).
Patient knowledge and attitudes about opioid medications.
Patient knowledge and attitudes towards opioid medications associated with use (vs lack of use) in the last 6 months adjusted for sociodemographic and clinical variables (n = 271).
Those with a high school education or lower, compared to those with more than a high school education, were less likely to have heard of the use of opioid medications for OA (71.9% vs 82.5%, P = 0.03) and perceived opioid medications as less risky (mean 2.1 vs 3.0, P < 0.001). Other familiarity with opioid medication statements and perception of medication benefit, however, did not differ by educational level (Table 2).
Compared to those with an annual household income of at least $40,000, those with an income < $40,000 per year perceived opioid medications as less risky (mean 2.3 vs 3.0, P < 0.001). However, perceived medication benefit and familiarity with opioid medications did not differ by annual household income level (Table 2).
DISCUSSION
In this sample of patients with OA, patient knowledge and attitudes regarding opioid medications were significantly associated with use of opioids in the management of pain. We specifically found that having family or friends who have used opioid medications, and having higher perceived benefit and lower perceived risk of opioid medications were independently associated with their use. Perceived risk of the use of opioid medications was lower, whereas opioid medication use for OA was higher, among those with lower educational attainment and less income. Use of the treatment was also more common among those with fair or poor health, higher levels of depression, and higher OA disease severity.
Knowledge, attitudes, and beliefs about treatments may influence perceptions of need and use of health treatments, including treatments for OA.36,37 In a recent study, patients’ familiarity with exercise and higher perceived benefits of exercise were associated with exercise use for OA treatment.20 Patients’ familiarity, along with lower perceived risk and higher perceived benefits, of joint replacement surgery were also strongly linked to their willingness to undergo joint replacement surgery.21. In turn, willingness to have the surgical procedure had been tightly linked to actual joint replacement.22 The current study, albeit cross-sectional and therefore unable to establish direction of causality, found positive associations between patient knowledge and attitudes about opioid medications and utilization of an opioid medication for knee/hip OA.
Patients’ perceptions about the effects of opioid medications may or may not reflect the treatment’s actual effects, however. While higher perceived benefit may be linked to more use of an opioid medication, pain and disability may only be minimally relieved with an opioid drug. In a metaanalysis, treatment of OA patients with opioids compared to placebo was associated with a mere 12% improvement in pain and 11% improvement in function.38 A systematic review found that nonsteroidal antiinflammatory drugs and opioids offer comparable levels of pain relief in OA.39 In a randomized trial, treatment with opioids was not superior to treatment with nonopioid medications for improving pain-related function due to chronic back or joint pain, and adverse medication-related symptoms were more common among opioid users.40 Perceived risk about opioid medicines may also be underestimated or overestimated. Up to 22% of people with OA who use opioids experience a side effect, and 1.3% have adverse events that result in hospitalization, permanent disability, or death.38 Use of opioids compared to placebo was also previously associated with higher risk of having an adverse event affecting the upper and lower gastrointestinal, dermatologic, and central nervous systems.41
Similarly, familiarity with a medication may not be helpful when the information about it is incomplete or imprecise. It was not surprising to find that having family or friends who used an opioid medication was associated with self-reported use of the drug. An individual’s social network often influences utilization of various treatments.20,42 When the treatment is high risk, however, the effect may be detrimental to the individual’s health and can lead to drug misuse or overuse. In a qualitative study of 30 nonmedical opioid users, most admitted that they initiated recreational use when they were able to access the medication through a family member or friend.43 Regardless, patient knowledge and beliefs about opioid medications may be changed through patient education.44,45
Lower educational attainment and income were both associated with greater use of an opioid medication for OA treatment in our study. Education level was not significantly associated with opioid use in other studies of patients with arthritis.15,16,46 However, lower income was consistently associated with current use of an opioid medication in several OA studies.14,46 It is possible that those with lower income have less access to other OA treatments that require financial resources and/or time commitment (e.g., exercise, complementary/alternative therapies). Our study additionally found that those with a lower level of education and income were less likely to perceive an opioid medication as risky compared to those with higher levels of education and income. Less educated study participants were also found to have lower awareness of its use as a treatment in OA.
Our cross-sectional study found an association between greater OA disease severity (which was based on patient-reported measures) and opioid use. This association was also found in other studies.14,15,18 The finding also suggests that patient perspectives are likely taken into account when providers consider prescribing these types of medications and that some patients with OA may truly benefit from opioid use. However, while disease severity may lead to increased use of an opioid therapy, it is also possible that opioid use may worsen OA symptoms. Prospective studies may be useful in clarifying these relationships. The association between OA disease severity and opioid use may also be an example of confounding by indication; those with more severe joint pain might have been more likely to be offered opioids by providers. Nevertheless, OA-related pain severity was controlled for in our multivariable analysis (Table 3).
More than 25% of the study participants reported opioid use for OA in the last 6 months. In contrast, in a study of veterans with OA from 1998 to 1999, 41% of subjects had at least 1 opioid prescription.13 In a study of community-dwelling elders with OA from 2002 to 2003, prescription opioids were taken by < 10% of participants.15 In a national study of patients with knee OA, opioid prescription was received by 31% in 2003, 39% in 2006, and 40% in 2009.47 An administrative claims database study from 2007 to 2014 found that 13% of hip OA and 16% of knee OA patients were prescribed an opioid.48 Differences in the reported rates of opioid use are likely from various reasons: varying times of study administration, different data sources, different study designs, and sample differences (e.g., radiographic vs nonradiographic OA).
There are several limitations to consider in interpreting our results. First, this is a cross-sectional study; only associations, and not causal relationships, between patient knowledge/beliefs about opioids and opioid medication use could be made. Second, all measures used for this study were based on self-report, including opioid medication use. Although self-reported measures are vulnerable to memory and social desirability biases,49 self-reported medication use tends to correlate well with pharmacy data confirming high validity and utility for analysis.50 Third, our sample is composed of a population primarily residing in Tucson, Arizona. The generalizability of our findings to other patients with OA who reside in other geographic regions is unknown. Future studies should consider replicating our study in other geographic areas. Fourth, we do not have details on patients’ more specific and explicit reasons for opioid use or nonuse. Future research should examine the role of other patient-related variables that may affect opioid medication use for OA, such as previous experiences with opioids, perceived financial burden associated with medical care, and perceived benefits/risks of other therapies for OA. Fifth, provider-related characteristics (e.g., recognition of appropriateness of opioid use, bias for/against opioid use) could also affect the associations observed in our main analyses; these should be studied as well. Finally, our sample was limited to people who were successfully contacted and could fill out a questionnaire. Treatment use patterns and beliefs about opioid medications may differ among those who could not or chose not to participate in the research study. The Health Insurance Portability and Accountability Act prevents us from gathering data from nonstudy participants, so we cannot compare our study sample from screened but nonconsented OA patients.
In this cross-sectional study, we found that patient knowledge and beliefs about opioids were associated with use of opioid medications in the management of OA-related pain symptoms. Among patients with knee or hip OA, those who were on an opioid medication, compared to those who were not, were more familiar with opioids, were more likely to believe in their efficacy, and perceived them as less risky. Perceived medication efficacy and risk, as well as having family or friends who use the medication, were associated with opioid medication use even after controlling for patient sociodemographic and clinical characteristics. Use of an opioid medication for OA was also more common among those with lower education, lower income, poorer physical and mental health, and more OA-related symptoms. Patients’ perceptions and beliefs about opioids should be evaluated and discussed when considering these medications for OA treatment.
ACKNOWLEDGMENT
We would like to thank Andrea Arellano and Jazmin Dagnino for assistance with patient recruitment. We would also like to thank all BUMC patients and University of Arizona Arthritis Center research registry members who participated in the study.
Footnotes
The current study and ERV were funded in part by the National Institutes of Health (NIH)/National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS) (K23AR067226). CKK’s work was supported by the NIH/NIAMS (R01AR066601). SAI was supported in part by a K24 Mid-Career Development Award from NIAMS (K24AR055259).
The authors declare no conflicts of interest.
- Accepted for publication January 8, 2021.
- Copyright © 2021 by the Journal of Rheumatology








{kind=link}