

Abstract
Objective. To investigate whether tumor necrosis factor inhibitor (TNFi) combination therapy with conventional synthetic disease-modifying antirheumatic drugs (csDMARD) is more effective for psoriatic arthritis (PsA) and/or improves TNFi drug survival compared to TNFi monotherapy.
Methods. Five PsA biologics cohorts were investigated between 2000 and 2015: the ATTRA registry (Czech Republic); the Swiss Clinical Quality Management PsA registry; the Hellenic Registry of Biologics Therapies (Greece); the University of Bari PsA biologics database (Italy); and the Bath PsA cohort (UK). Drug persistence was analyzed using Kaplan-Meier and equality of survival using log-rank tests. Comparative effectiveness was investigated using logistic regression with propensity scores. Separate analyses were performed on (1) the combined Italian/Swiss cohorts for change in rate of Disease Activity Score in 28 joints (DAS28); and (2) the combined Italian, Swiss, and Bath cohorts for change in rate of Health Assessment Questionnaire (HAQ).
Results. In total, 2294 patients were eligible for the drug survival analysis. In the Swiss (P = 0.002), Greek (P = 0.021), and Bath (P = 0.014) databases, patients starting TNFi in combination with methotrexate had longer drug survival compared to monotherapy, while in Italy the monotherapy group persisted longer (P = 0.030). In eligible patients from the combined Italian/Swiss dataset (n = 1056), there was no significant difference between treatment arms in rate of change of DAS28. Similarly, when also including the Bath cohort (n = 1205), there was no significant difference in rate of change of HAQ.
Conclusion. Combination therapy of a TNFi with a csDMARD does not appear to affect improvement of disease activity or HAQ versus TNFi monotherapy, but it may improve TNFi drug survival.
Tumor necrosis factor inhibitors (TNFi) are an effective treatment for psoriatic arthritis (PsA)1 and are generally prescribed following the failure of initial treatment with conventional synthetic disease-modifying antirheumatic drugs (csDMARD), of which methotrexate (MTX) is the most widely used. TNFi may be prescribed as monotherapy or in combination with csDMARD with 51% to 79% of patients using TNFi in combination with MTX2. A systematic review of randomized controlled trials (RCT) and observational studies of TNFi monotherapy versus TNFi combination therapy with MTX did not find any difference in efficacy for peripheral disease, but there was some evidence of benefit of combination therapy on TNFi drug survival2. While there is clear evidence for the benefit of combination TNFi plus csDMARD in rheumatoid arthritis (RA)3, the value of combination therapy in PsA remains unresolved4, and this may explain the variability observed in clinical practice and the lack of clarity in current treatment guidelines5,6.
Biologics registries have been set up globally to investigate the long-term efficacy and safety of TNFi. The aim of this study was to combine data from multiple European TNFi databases to describe the utilization patterns of TNFi monotherapy and combination therapy in PsA and to investigate the comparative effectiveness of TNFi monotherapy versus combination therapy in terms of drug survival and patient outcomes.
MATERIALS AND METHODS
Participating databases. An invitation to participate in the study was sent to all European biologics registries known to collect data on patients with PsA. Three biologics registries and 2 hospital-based PsA biologics cohorts agreed to participate and were included in the study: the ATTRA registry, Czech Republic (the “Czech database”); the Swiss Clinical Quality Management (SCQM) in Rheumatic Diseases PsA registry, Switzerland (the “Swiss Database”); the Hellenic Registry of Biologic Therapies (HeRBT), Greece (the “Greek Database”); the University of Bari School of Medicine PsA biologics database, Italy (the “Italian Database”); and the Royal National Hospital for Rheumatic Diseases, Bath, UK PsA cohort (the “Bath Database”). The hospital-based Italian and Bath databases are both prospective cohort studies that have submitted data to the biologics registry that was established by the Italian Group for the Study of Early Arthritis (GISEA) and the British Society for Rheumatology Rheumatoid Arthritis Biologics Registry (BSRBR-RA), respectively, and were therefore deemed of sufficiently high quality in terms of data collection to be included in the study. Ethics approval was granted for each of the 5 cohorts (for the lead center, this was by the South West-Central Bristol National Research Ethics Service Committee, approval number BA74/00-01; all other approvals can be found in Supplementary Table 1 (available with the online version of this article). A summary of data collection for each database is shown in Supplementary Table 2.
Study population. The study period ran from January 1, 2000 to December 31, 2015. We included all adults (3 18 yrs) with a clinical diagnosis of PsA who were new (first-line) users of TNFi during the study period and who were registered in their respective biologics database from the time of first TNFi prescription. Patients who had been prescribed any other type of biologic DMARD before their first TNFi prescription were excluded. Patient and disease characteristics at baseline were extracted from the databases.
Drug exposure and patient follow-up. Recorded prescription data was used to determine exposure status during the follow-up period. Exposure to treatment groups was classified at baseline into: (1) TNFi monotherapy; and (2) TNFi combination therapy with MTX (this group was also included in a category of TNFi combination therapy with any csDMARD, including MTX).
Patient follow-up and outcome measures. Patients were followed until their censoring date, which was the earliest of (1) the time of discontinuation of their first TNFi agent, defined as discontinuation of therapy for at least 3 months; or (2) the date that they were lost to follow-up; or (3) the date of their last follow-up on the biologics database, whichever was the earliest. Drug persistence was defined as the time from TNFi to censoring date.
The primary outcome measure for the comparative effectiveness analyses was rate of change of disease activity, measured using the Disease Activity Score in 28 joints (DAS28)7, during the follow-up period. The secondary outcome measure was rate of change in physical function, measured using the Health Assessment Questionnaire (HAQ)8, during the follow-up period.
Statistical analyses. Statistical analyses were undertaken using R statistical software9. Individual patient data from the Bath, Italian, and Swiss databases were analyzed at the University of Bath; the Czech and Greek data were analyzed locally. A full description of the statistical methods can be found in the Supplementary Data 1 (available with the online version of this article).
Drug survival. Drug survival was analyzed using Kaplan-Meier survival estimates and defined as time from TNFi initiation to censoring date, stratified by treatment group, age at TNFi initiation, and sex. The median time from baseline to discontinuation of first TNFi, with 95% CI, was calculated from the survival function. The equality of the survival functions was compared using log-rank tests.
Comparative effectiveness. Due to the complexity of the comparative effectiveness analyses modeling, we only included data for which we had individual patient data at the University of Bath (Bath, Italian, and Swiss databases). Initial data analysis included examining changes in DAS28 and HAQ over time, without adjustment for covariates. Comparative effectiveness analyses were based on an intention-to-treat analysis approach using negative binomial regression. Comparisons were made between TNFi monotherapy and (1) any TNFi + csDMARD and, as a subgroup analysis, we also compared to (2) TNFi + MTX. For HAQ, in order to allow for the observed excess of zeros, a zero-inflated negative binomial model was used, with a consistent set of covariates used for both components of the model. Statistical comparisons were based on the relative difference in rates of change in disease score between treatments.
While each registry had planned follow-up periods (for example 3, 6, 12 months), the actual dates of follow-up varied substantially around these, with additional follow-up appointments also being recorded. Attempting to classify these variable follow-up appointments into specific follow-up periods (e.g., change at 3 months and 6 months) resulted in significant loss of data. Therefore, we included all follow-up data in the analysis rather than planned timepoints.
The regression models were adjusted for age at TNFi initiation and sex. Differences between rates of improvement in the 2 treatment groups were obtained by including an interaction term between time and treatment group in the regression models. To account for any confounding by indication, we developed database-specific propensity score (PS) models, using all available baseline data, to calculate the individual PS for treatment to monotherapy or combination therapy. All covariates that were not explicitly included in the model were included in the PS models, including clinical characteristics such as disease duration.
Missing values in any explanatory variable (where < 70% were missing) were estimated using multiple imputation using the Amelia II package in R10. In order to test for a significant difference in the rate of change for each treatment group, estimates of the log relative risk (RR) with standard error associated with the interaction between treatment group and time were extracted and then combined to give an overall estimate of RR, together with a combined standard error using Rubin’s rule.
RESULTS
There were 2294 eligible patients identified from the contributing databases, of which 34% started treatment as monotherapy and 66% as combination therapy. Table 1 summarizes requirements for access to TNFi and baseline patient characteristics. Clinical guidelines for access to TNFi differed across countries. The effect of the guidelines on measures of disease severity and activity at TNFi initiation was reflected in the relatively lower HAQ and DAS28 scores in the Swiss database and higher baseline scores in the Bath database. Comorbidity data were not consistently recorded across all of the databases; however, in general, the proportion of patients with significant comorbidities was < 5% of each study population, with the exception of a prevalence of latent tuberculosis (TB) of 13% in the Italian database due to screening for latent TB.
Patient characteristics stratified by biologics database and baseline treatment regimen.
Drug utilization. In all centers, TNFi were more commonly prescribed in combination with a csDMARD than as monotherapy and MTX was the csDMARD most frequently prescribed (Table 1). Changes in baseline prescribing during the study period are shown in Supplementary Figure 1 (available with the online version of this article). Patient characteristics and baseline disease activity and severity were generally similar across treatment groups within the databases (Table 1). Adalimumab (ADA) and etanercept (ETN) were the most frequently prescribed TNFi in all databases other than the Greek database, where 47.7% of patients were treated with infliximab (IFX). Supplementary Table 3 shows the TNFi products prescribed at baseline. The majority of patients (81.7% monotherapy and 66.0% combination therapy) did not have changes to their baseline treatment regimen before discontinuing their first TNFi, and > 85% of these changes were made > 12 months after TNFi initiation.
Drug survival. The Kaplan-Meier survival curves for drug survival on first TNFi, stratified by database and baseline treatment regimen, are shown for monotherapy versus any csDMARD combination therapy in Figure 1 and monotherapy versus combination therapy with MTX in Supplementary Figure 2 (available with the online version of this article). Figure 2 shows the Kaplan-Meier survival curves for drug survival stratified by sex and Supplementary Figure 3 shows them stratified by age. Median survival times are shown in Table 2. Discontinuation of first TNFi was earliest in patients in the Swiss database (median 2.8 yrs, 95% CI 1.5–3.7); patients in the Greek database had the longest median survival time (6.9 yrs, 95% CI 4.9–not available, defined as < 50% dropout).

Kaplan-Meier survival estimates from TNFi initiation to discontinuation of first TNFi or data censoring stratified by baseline treatment regimen, monotherapy compared with TNFi + csDMARD combination therapy. csDMARD: conventional synthetic disease-modifying antirheumatic drug; TNFi: tumor necrosis factor inhibitor.

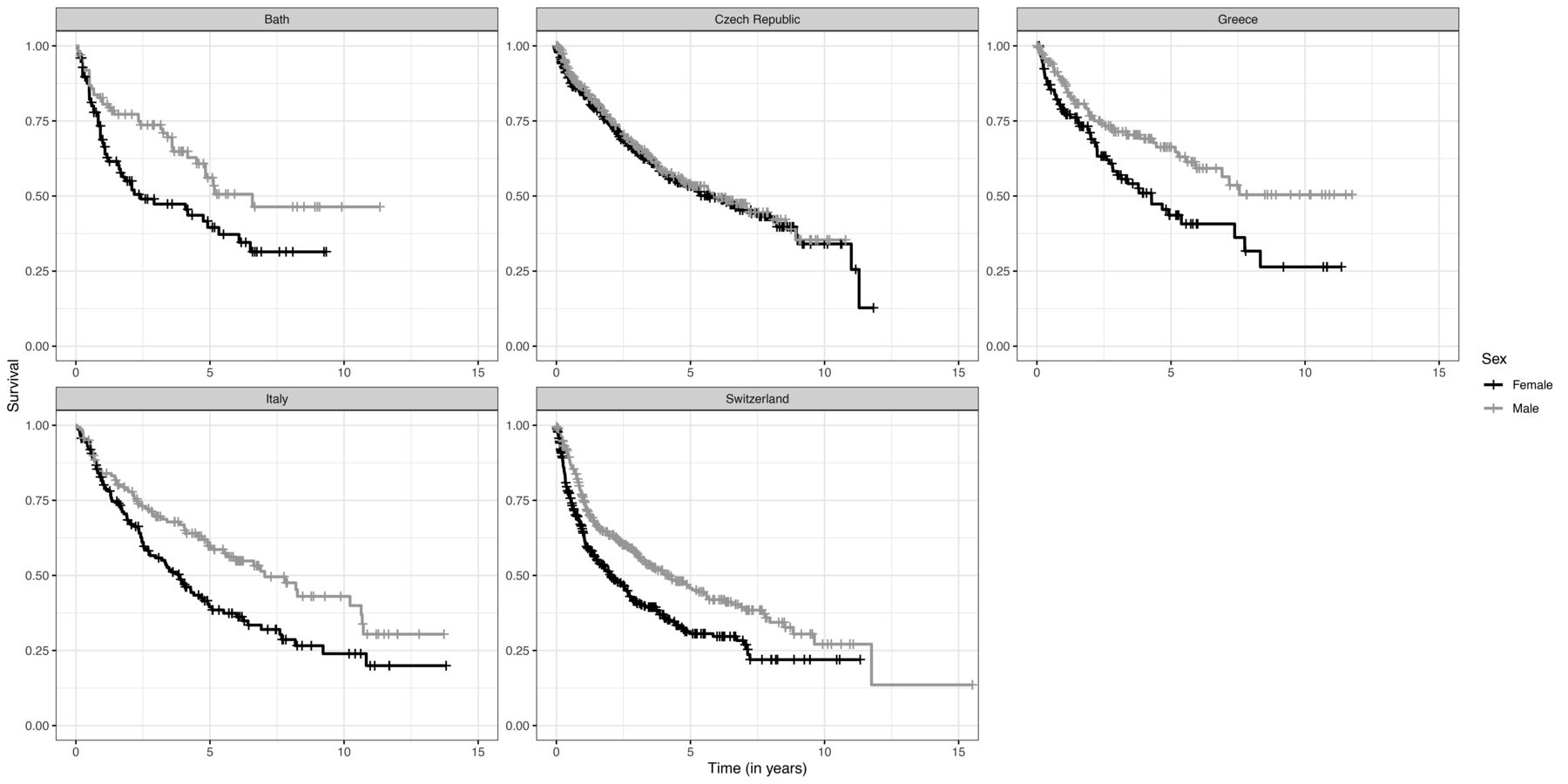
Kaplan-Meier survival estimates from TNFi initiation to discontinuation of first TNFi or data censoring stratified by sex. TNFi: tumor necrosis factor inhibitor.
Median survival times from TNFi initiation to discontinuation of first TNFi stratified by baseline treatment regimen and database.
In all but the Italian database, patients on combination therapy had longer survival on their first TNFi than those on monotherapy. This ranged from 0.5 to 2.9 years and the difference was statistically significant in the Bath and Swiss databases for any combination and in the Bath, Greek, and Swiss databases for combination with MTX (Figure 1, Table 2). In the Italian database, patients on monotherapy persisted significantly longer on their first TNFi than those on combination therapy, but this difference did not remain significant when the analyses were limited to combination therapy with MTX. In all but the Czech database, where we observed no difference, men persisted significantly longer on their first TNFi than women (Figure 2 and Table 2).
Comparative effectiveness. The analysis of rate of change in DAS28 included 1056 patients from the Swiss and Italian databases with a DAS28 score recorded; 441 were prescribed TNFi monotherapy at baseline and 615 were prescribed combination therapy with any csDMARD, of whom 442 were prescribed TNFi + MTX. Sixty-eight patients from the Swiss database were excluded because they did not have a DAS28 score recorded. The analysis of rate of change in HAQ included 1205 patients from the Bath, Swiss, and Italian databases (504 monotherapy and 701 combination therapy with any csDMARD of whom 505 were exposed to TNFi + MTX). We excluded 107 Swiss patients and 11 Bath patients who had no HAQ scores recorded before their censoring dates.
Within the database-specific PS models for both the DAS28 and HAQ analyses, patients who had previously used csDMARD had a higher baseline HAQ and those who had a history of dactylitis were significantly more likely to be prescribed combination therapy. None of the recorded comorbidities were significant in the models and there was no difference in the PS for TNFi + any csDMARD, and TNFi + MTX groups. None of the variables included in the Bath PS model were significantly associated with treatment allocation.
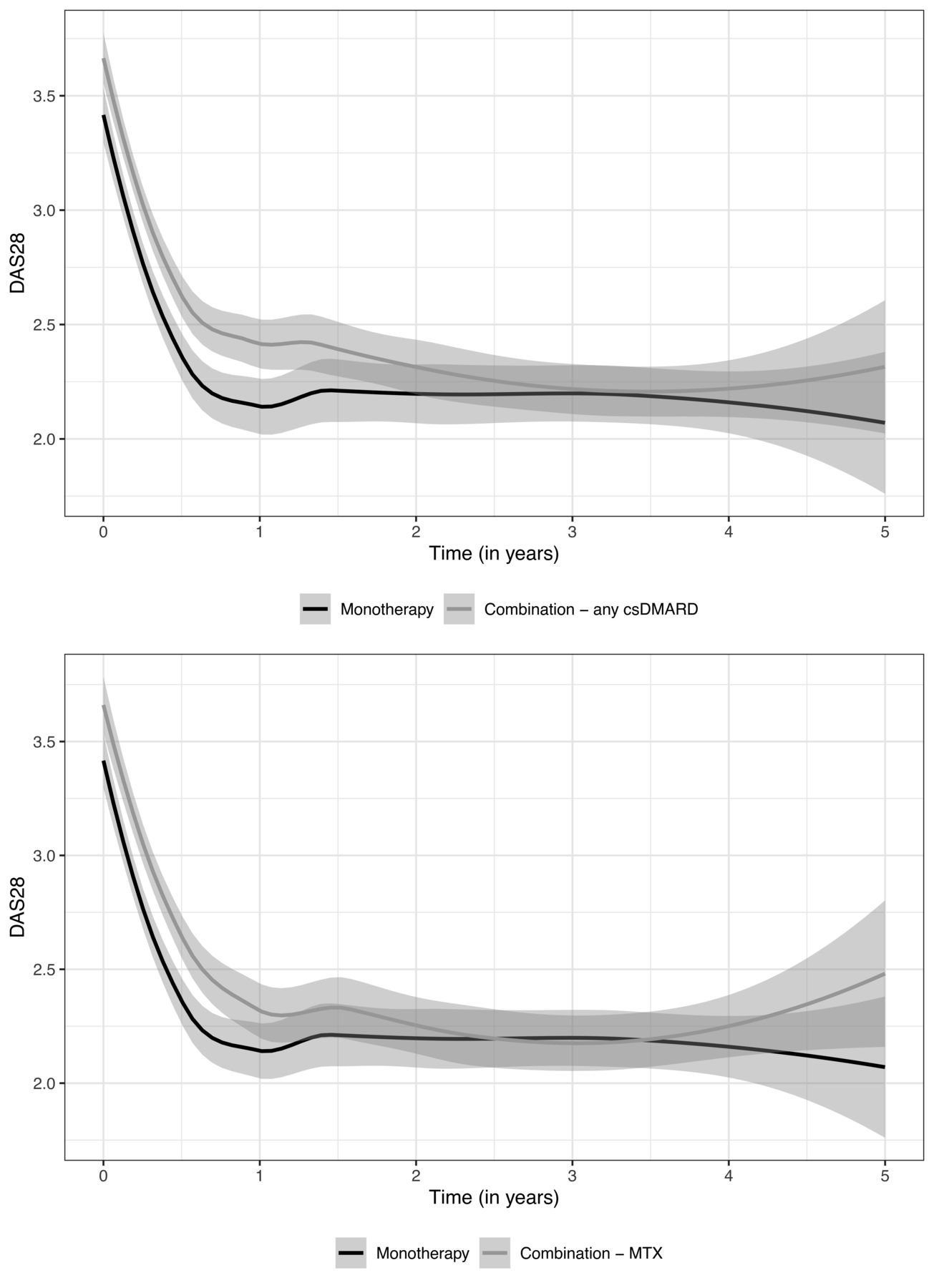
Figure 3 and Figure 4 show the change in DAS28 and HAQ over time, respectively, unadjusted for any covariates. In both the DAS28 and HAQ analyses, patients on combination therapy had higher baseline scores than patients on monotherapy. The pattern of rate of change was similar in both analyses, with scores dropping sharply in the first year after treatment initiation, increasing slightly then stabilizing from 12 months onwards.

DAS28 over time, unadjusted for any covariates, among patients from the Italian and Swiss databases from TNFi initiation to the earliest of: (1) discontinuation of first TNFi; or (2) date of data censoring; or (3) 60 months follow-up for (3a) monotherapy versus combination TNFi + any csDMARD and (3b) monotherapy versus combination TNFi + MTX. csDMARD: conventional synthetic disease-modifying antirheumatic drug; DAS28: Disease Activity Score in 28 joints; MTX: methotrexate; TNFi: tumor necrosis factor inhibitor.
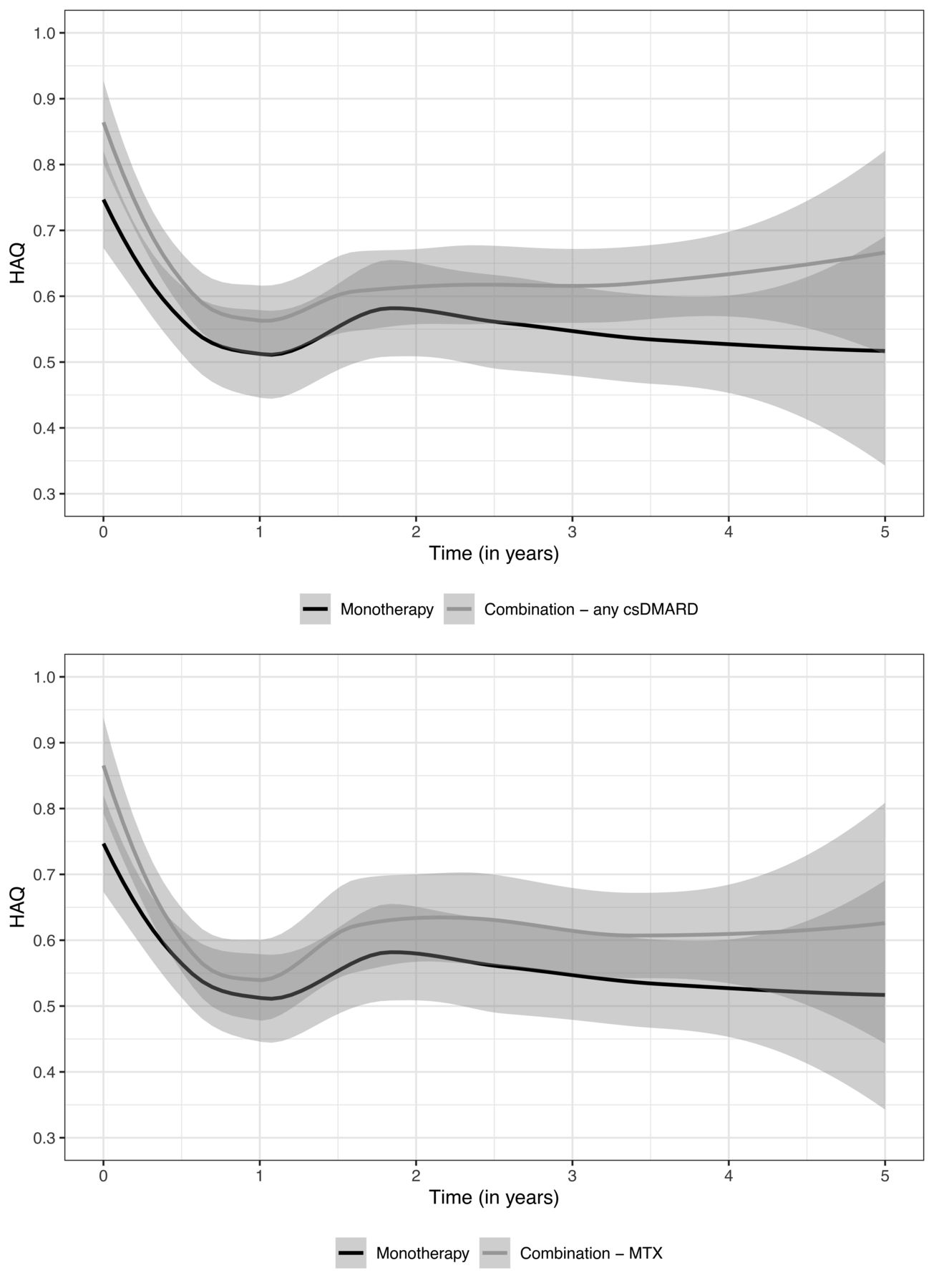
HAQ over time, unadjusted for any covariates, among patients from the Bath, Italian, and Swiss databases from TNFi initiation to the earliest of: (1) discontinuation of first TNFi; or (2) date of data censoring; or (3) 60 months follow-up for (4a) monotherapy versus combination TNFi + any csDMARD and (4b) monotherapy versus combination TNFi + MTX. csDMARD: conventional synthetic disease-modifying antirheumatic drug; HAQ: Health Assessment Questionnaire; MTX: methotrexate; TNFi: tumor necrosis factor inhibitor.
There was no statistically significant difference in rate of change of DAS28 between patients on TNFi monotherapy with those on combination therapy with any csDMARD [combined adjusted RR (RRadj) 0.98, 95% CI 0.95–1.03] or on monotherapy compared with TNFi + MTX (combined RRadj 0.98, 95% CI 0.95–1.02). There was no statistically significant difference in rate of change of HAQ in patients on monotherapy compared to those on combination therapy with any csDMARD (combined RRadj 1.02, 95% CI 0.98–1.06) or when compared to those on TNFi + MTX (combined RRadj 1.02, 95% CI 0.99–1.07). Inclusion of the PS in the models did not significantly change the combined RR.
There were no notable differences in reasons for stopping the first TNFi between the databases. Supplementary Table 4 (available with the online version of this article) summarizes the reasons for treatment discontinuation stratified by database and baseline treatment regimen. Overall 23.5% of the 1323 patients from the Bath, Italian, and Swiss databases discontinued treatment in the first year after TNFi initiation and the proportion was lower in patients exposed to TNFi + MTX (21.8%) than those on monotherapy (25.9%) or TNFi + non-MTX csDMARD (26.5%). Lack of treatment efficacy was the most frequently recorded reason for discontinuation (9.8% overall; 11.3% monotherapy, 7.9% TNFi + MTX, and 10.8% TNFi + non-MTX csDMARD) followed by adverse drug reactions (7.6% overall; 7.0% monotherapy, 6.5% TNFi + MTX, and 9.4% TNFi + non-MTX csDMARD). Lack of treatment efficacy remained the most frequently recorded reason for treatment discontinuation at any time after TNFi initiation, followed by adverse drug reactions.
DISCUSSION
The results of this multiregistry study are consistent with previous studies of TNFi monotherapy versus combination therapy treatment in patients with PsA. We found no significant difference in clinical outcome between the treatment groups, which is in line with observational studies in Sweden11, Norway12,13, the UK14, Denmark15, and Finland16. A recent RCT found that combination therapy of ETN and MTX may not improve radiographic progression compared with ETN monotherapy, although combination therapy had slightly greater efficacy for dermatologic endpoints17. In the Bath, Greek, and Swiss databases, patients were found to persist significantly longer on their first TNFi when prescribed in combination with MTX than patients on TNFi monotherapy. This has also been observed in studies in Denmark15,18, Norway13, Sweden11, and Italy19,20; in Denmark, however, this was only found when adjustments were made for other baseline variables15. Although some studies have not reported significantly longer persistence with MTX16,21,22, no study has reported longer persistence for patients on monotherapy as was observed in the Italian database. One study in the US, however, did report different findings for the individual TNFi, with significantly longer persistence for ETN as monotherapy although the opposite was observed for IFX and there was no difference between treatment groups for ADA22. Our study, however, did not look at individual TNFi and so could not determine whether the benefit of combination therapy varied by TNFi. Our study did find some evidence that a lower proportion of patients on TNFi + MTX stop in the first year of treatment due to a lack of treatment efficacy or adverse drug reactions. The reason for this finding is not clear and whether there is an explanatory biological mechanism such as the inhibition of the development of antidrug antibodies needs further investigation.
A study in Sweden had found patients without MTX showed significantly lower drug survival due to adverse events but did not find a difference for treatment failure11. Our study found that in all but the Czech database, males persist significantly longer on their first TNFi than females, and this has been observed in some studies looking at PsA15,19,20,21,23,24,25,26 but not others11,13. This finding has also been reported for RA and ankylosing spondylitis27,28,29. Other predictors that have been found to be associated with drug survival include having a higher baseline C-reactive protein11,15, a low baseline visual analog scale score for global health15, being a nonsmoker13, and absence of baseline comorbidity21,26,30, including a metabolic syndrome–related comorbidity31 and obesity32. Predictors have also been reported to vary depending on the reason for discontinuation, with some being associated with discontinuation for adverse events and others for a lack of efficacy11,15.
This study aimed to combine European biologics registry data to investigate treatment utilization patterns and outcomes in PsA. The prescribing criteria and disease activity scores, however, were not standardized across databases and as such the drug utilization analyses were carried out separately. For the comparative effectiveness analyses, limitations included the fact that individual patient-level data were not available for all databases and also that HAQ was the only outcome measure commonly recorded. For the databases where individual-level data was available and outcome measures were common, we have, however, demonstrated that statistical models using individual patient data can be developed to combine data that have been collected in different healthcare contexts but using similar study designs. Although patients from the different databases had differing baseline disease activity and severity scores due to differences in access requirements to TNFi across Europe, we have demonstrated that clinical outcome measures can be combined by analyzing rate of change rather than absolute change in DAS28 or HAQ from baseline, which is a methodological strength of the study.
Another limitation of the data was that the actual dates of follow-up varied considerably. It was therefore necessary, when performing the modeling for the comparative effectiveness, to include all follow-up data and model time as a continuous covariate, as restricting to specific time periods would have resulted in a significant loss of data and the potential for bias.
We designed the study to use DAS28 as the primary outcome measure and HAQ as the secondary outcome measure because the majority of biologics databases have been set up to primarily collect treatment effectiveness and safety data in patients with RA and we therefore expected that DAS28 would be the outcome measure more readily available. While DAS28 has been validated for use in PsA, its usefulness is limited by the exclusion of the ankle joints and feet, which are frequently affected in PsA. We did, however, find that all databases collected data on HAQ, which is arguably a more relevant outcome measure for studies of PsA. However, none of the databases collected data on all of the outcome measures in the more disease-specific Outcome Measures for Rheumatology (OMERACT) core set of outcomes for PsA33. As a result, our analysis of the effectiveness of TNFi treatment is limited to physical function and cannot take into account other domains such as pain, fatigue, work productivity, enthesitis, or skin disease activity and health-related quality of life, which are important to people with PsA; these other domains are also important when carrying out cost-effectiveness analyses of treatment.
We used PS modeling to attempt to minimize the effect of confounding by indication and channeling bias; however, the effectiveness of PS adjustment for treatment allocation is limited by the variables collected in the databases and whether they are the variables that might be associated with treatment allocation. We used all available data within the PS models, and both a history of dactylitis and higher baseline HAQ scores predicted the use of combination treatment. However, there were issues with large amounts of missing data for some variables and we had no measures of previous treatment compliance, tolerance, or success. Therefore, we cannot rule out the potential for uncontrolled confounding by indication and it is not possible to predict the effect that this might have on the findings of the study.
In conclusion, we have demonstrated the feasibility of combining biologics registry and database data to investigate the comparative effectiveness of TNFi treatment for PsA, but as with all observational studies, the results need to be interpreted with caution. We have found that while there is no significant difference in treatment outcome, as measured using DAS28 and HAQ, patients on combination therapy persist longer on their first TNFi than those on monotherapy. Sex appears to be a major risk factor in determining TNFi survival, with males persisting for longer.
ACKNOWLEDGMENT
We would like to thank all patients and rheumatologists for contributing data to the respective registries. For the SCQM, a list of rheumatology offices and hospitals that contribute data can be found on www.scqm.ch/institutions. The SCQM is financially supported by pharmaceutical companies (www.scqm.ch/sponsors).
Footnotes
The study was funded by a nonrestricted investigator-initiated award from Pfizer.
NM, AN, RC, MT and CC report grants from Pfizer during the conduct of the study. NM reports personal fees from AbbVie and Lilly and grants from Lilly outside the submitted work. CC reports grants from Celgene, Lilly and Novartis and personal fees from Novartis outside of the submitted work. FI reports personal fees from AbbVie, BMS, Novartis, Pfizer, Lilly, UCB and MSD outside the submitted work. GL reports personal fees from AbbVie, BMS, Novartis, Pfizer, and MSD outside the submitted work. KP reports honoraria for consultations and speaker fees from AbbVie, Pfizer, UCB, Lilly, Novartis, and Roche outside the submitted work. PS reports that the Hellenic Registry for Biologic Therapies was supported in part by the Hellenic Rheumatology Society through unrestricted grants from Schering-Plough, AbbVie, Pfizer, Bristol Myers Squibb, and Roche during the conduct of the study. These companies had no role in study design, collection, analysis, and interpretation of the data and in the writing of the manuscript. PS also reports grants and personal fees from the pharma industry through the University of Crete Special Account for Research, outside the submitted work.
- Accepted for publication March 18, 2020.
REFERENCES
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.








{kind=link}
{kind=link}
{kind=link}
{kind=link}