

Abstract
Objective. Rheumatoid arthritis (RA) and other rheumatic diseases may present with ocular manifestations.
The purpose of our work was to determine the prevalence and type of eye involvement in RA and other connective tissue diseases through a metaanalysis and literature review.
Methods. A systematic review of the literature was performed using Medline, Web of Science, and the Cochrane Library from their inceptions until January 7, 2019. Conjunctivitis, keratoconjunctivitis sicca, xeropthalmia, uveitis, eye hemorrhage, optic neuritis, papilledema, orbital disease, retinal artery/vein occlusion, macular edema, retinitis, chorioretinitis, scleritis, iridocyclitits, choroid hemorrhage, blindness, and amaurosis fugax were searched for prevalence in patients with RA, systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS), dermatomyositis, polymyositis, systemic sclerosis, Sjögren syndrome (SS), undifferentiated connective tissue disease, giant cell arteritis, granulomatosis polyangiitis (GPA; formerly Wegener granulomatosis), systemic vasculitis, and sarcoidosis.
Results. There were 3394 studies identified and 65 included. The prevalence of eye involvement was 18% in RA, 26% in GPA, 27% in giant cell arteritis, 27% in sarcoidosis, 31% in SLE, and 35% in APS. The most common manifestation was dry eye syndrome (“dry eye”; keratoconjunctivitis sicca) in most diseases analyzed, with an especially high frequency of 89% in SS. Anterior and posterior uveitis were the most common ocular complications in sarcoidosis, occurring in 16% (95% CI 3–28) and 6% (95% CI 3–9) of patients, respectively.
Conclusion. Eye involvement is present in approximately one-fifth of patients with RA, and a one-quarter to one-third of patients with connective tissue diseases (other than SS at 89%) and vasculitis.
- connective tissue disease
- prevalence
- rheumatoid arthritis
- Sjögren syndrome
- systemic lupus erythematosus
- vasculitis
Rheumatoid arthritis (RA) is a multisystem autoimmune disease that generally damages synovial-lined joints in the hands, feet, wrists, and knees1. Extraarticular effects have been described in multiple organ systems, including the lungs2,3, kidneys4,5, cardiovascular system6,7,8, and eyes9. Subcutaneous nodules are the most common extraarticular manifestation and are present in 20–30% of patients10, although the frequency of nodules may be decreasing. Clinical observations suggest that severe complications, such as corneal “melts” and perforations in RA, are decreasing with advances in modern biologic treatments11,12.
As with RA, other inflammatory rheumatic diseases like connective tissue diseases (CTD) and vasculitis can also present with various systemic symptoms and signs. Although several organs involved in these diseases have been well categorized, the frequency of ocular involvement in some autoimmune rheumatic diseases is imprecise. While some CTD, like Sjögren syndrome (SS), nearly always manifest with dry eye syndrome (“dry eye”; keratoconjunctivitis sicca), the prevalence of ocular complications (OC) across the spectrum of RA, associated CTD, and vasculitis warrants further investigation13. In our report, we determined the frequency of eye involvement in RA and other inflammatory rheumatic diseases, including systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS), giant cell arteritis (GCA), granulomatosis with polyangiitis (GPA), and sarcoidosis. We found that ocular complications may be more stable in these conditions compared to those that occur in patients with RA. Retinal vasculitis may occur in CTD and vasculitis, whereas retinal infarctions and hemorrhages would be more likely in APS and SLE.
Here, we present a metaanalysis on our systematic review to compare the prevalence of uveitis and other OC among RA, CTD, and vasculitis.
MATERIALS AND METHODS
Study selection. Institutional review board approval was not necessary as this was a systematic literature review. The protocol for investigating the prevalence of ocular conditions in rheumatic diseases can be found at ClinicalTrials.gov (NCT03753893). The specific wording for our search strategy is listed in Supplementary Data 1 (available with the online version of this article). Medline, Cochrane, and Web of Science were used in searching papers that spanned from their inceptions (in 1964, 1997, and 2000, respectively) to January 7, 2019. All studies that included the prevalence of eye involvement in RA, CTD (SLE, APS, SS, polymyositis, dermatomyositis, scleroderma, undifferentiated CTD), and vasculitis (GCA, GPA, systemic vasculitis, and sarcoidosis) were included for further review.
Inclusion criteria. Studies were included if they investigated the prevalence of OC in the aforementioned diseases in the context of a cohort and were written in English. Review articles, case reports, cohorts in which all patients experienced the same OC, studies in which different comorbidities were not grouped independently, and studies that reported on fewer than 20 patients were excluded. When the same patient cohorts were used in more than 1 analysis, either the most recent study or the study with the largest sample size was included. The STrengthening the Reporting of OBservational Studies in Epidemiology (STROBE) checklist was used to assess the quality of cohort, case-control, and cross-sectional studies to check for bias14.
Data extraction. The following data were extracted for each study as per the registered protocol: first author, year of publication, location of study, study design, sample size, and prevalence of each OC. When studies included multiple populations with various rheumatic diseases, data extraction and analysis were done separately for each condition.
Statistical analysis. Forest plots were constructed from the extracted data to create a 95% CI using RevMan 5.3. A random effects model was used to account for bias and heterogeneity15. I2 and tau-square tests were used to determine heterogeneity and variance across studies. Differences between study frequencies were measured using 1-way ANOVA. Funnel plots were used to look for publication bias. Where possible, the frequencies of ocular manifestations in adults were compared to juvenile patients for each disease.
RESULTS
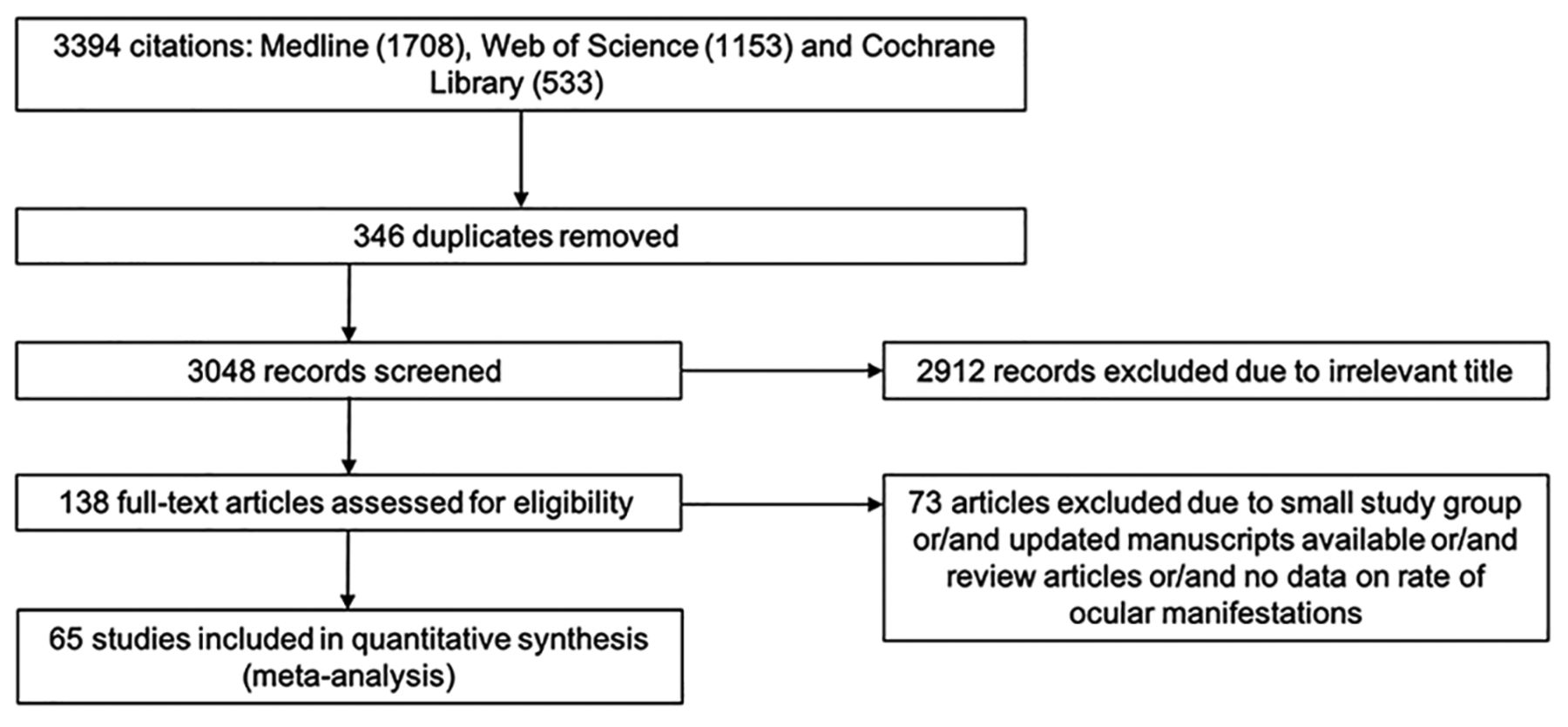
From the literature review, 3394 citations were identified and 65 were included (Figure 1; Table 1). The I2-heterogeneity statistic was high (73–100%); therefore, a random effects model was used to determine prevalence.

Summary of search strategy.
Characteristics and research quality of studies reporting the prevalence of OC in RA and other CTD.
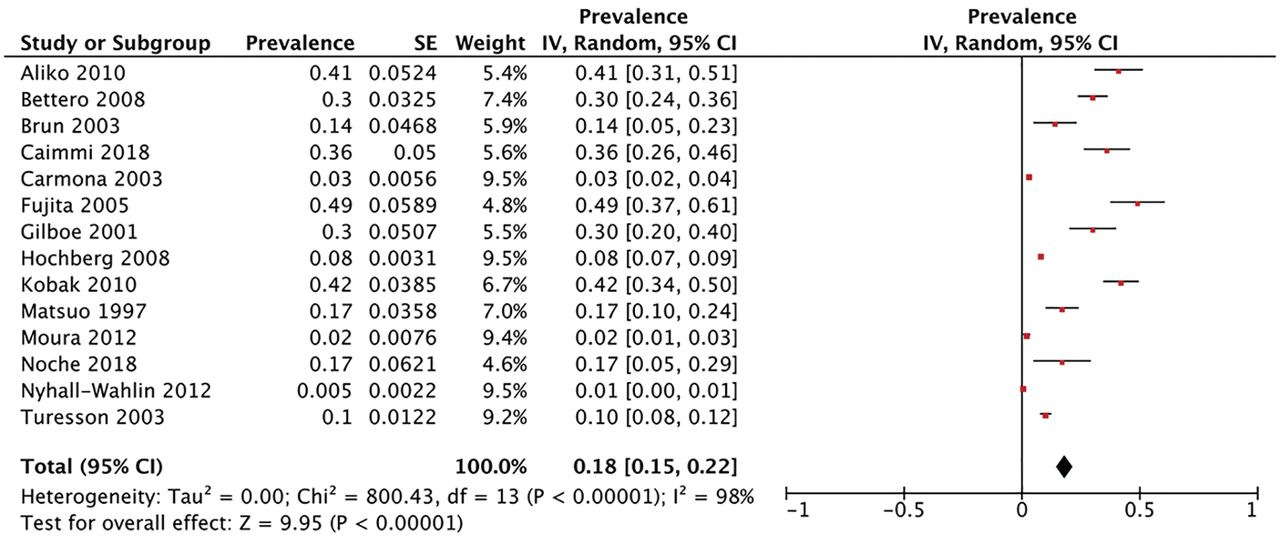
The pooled prevalence of OC in RA was 18% (95% CI 15–22; Figure 2). In other rheumatic diseases, the prevalence of OC varied by disease type. It was 27% (95% CI 18–36) in sarcoidosis, 89% (95% CI 86–92) in SS, 31% (95% CI 18–44) in SLE, 26% (95% CI 19–34) in GPA, 27% (95% CI 20-34) in GCA, 35% (95% CI 3–67) in APS, 0.07% (95% CI 0–19) in dermatomyositis, and 21% (95% CI 2–39) in systemic sclerosis (Figure 3).

The frequency of eye involvement in patients with rheumatoid arthritis. SE: standard error.

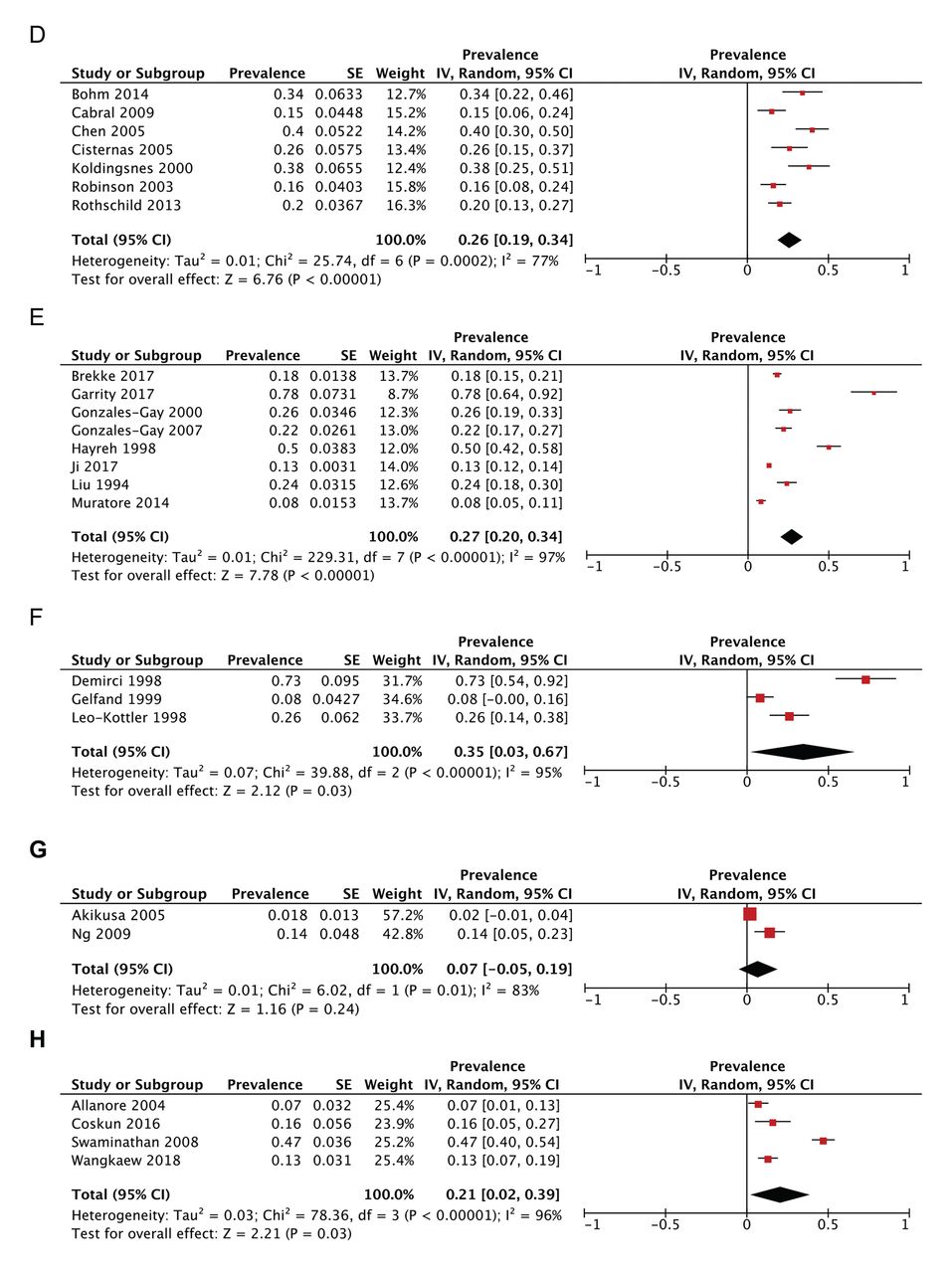
Frequency of eye involvement in patients with other investigated connective tissue diseases, including (A) sarcoidosis, (B) Sjögren syndrome, (C) systemic lupus erythematosus. SE: standard error. (D) granulomatosis with polyangiitis, (E) giant cell arteritis, (F) antiphospholipid syndrome, (G) dermatomyositis, and (H) systemic sclerosis. SE: standard error.
In RA, the most common OC was dry eye (16%, 95% CI 11–20), followed by glaucoma (5%, 95% CI 0–13; Figure 4). Dry eye was also the most common OC in SS (89%, 95% CI 86–92), SLE (33%, 95% CI 24–42), and SSc (27%, 95% CI 22–32). Anterior uveitis was the most common OC in sarcoidosis followed by posterior uveitis, occurring in 16% (95% CI 3–28) and 6% (95% CI 3–9) of patients, respectively (data not shown).

The frequency of different ocular complications in rheumatoid arthritis, including dry eye, episcleritis, glaucoma, and scleritis. SE: standard error.
A subanalysis was performed to compare the prevalence of OC in adult and pediatric patients where possible. In RA, OC occurred significantly more frequently in adults (28%, 95% CI 19–37; Supplementary Figure 1, available with the online version of this article) compared to children with RA (13%, 95% CI 12–14; P = 0.0035; data not shown). In GPA, OC were equally frequent in adults (20%, 95% CI 10–30) and children (24%, 95% CI 5–43; P = 0.38; Supplementary Figure 2, available with the online version of this article). Studies on other CTD and vasculitis did not report juvenile-specific data; however, studies with only adults did not report significantly different OC compared to the studies that included mostly adults and some patients with childhood-onset rheumatic diseases (Supplementary Figure 1).
Publication bias was negligible in all conditions except for APS and scleroderma, as evidenced by the funnel plots presented in Supplementary Figure 3 (available with the online version of this article).
DISCUSSION
Eye involvement occurs frequently across the spectrum of rheumatic diseases, although the location and type of eye complication varies. In RA, approximately 18% of patients had ocular features, such as dry eye and glaucoma. While eye involvement occurs in almost 1 in 5 patients, metrics to evaluate disease activity do not include specifically extraarticular involvement (e.g., Clinical Disease Activity Index/Simplified Disease Activity Index; Disease Activity Score in 28 joints)16,17,18. The argument is that extraarticular/other organ involvement should be more of a focus when evaluating these diseases17,19. Extraarticular symptoms can be improved with certain treatment and improve quality of life for patients with RA20.
When compared to the general population, RA and other CTD display a marked increase in OC. Within the general population, many factors contribute to the prevalence of OC, including age, sex, geographic location, and social factors. The general range of uveitis within the population is relatively low at 0.038% to 0.74%21. Dry eye syndrome is slightly more common, affecting 6.8% of the general US population; however, it occurs more frequently in CTD than in RA22. The prevalence of glaucoma among the general population is 3.5%, which is markedly lower than the prevalence seen in RA23, although the reasons for this difference are currently unknown. A 2016 study found no correlation between the use of glucocorticoids for RA treatment and the incidence of glaucoma24. More research is needed to identify the ways in which RA is associated with glaucoma, and whether the disease characteristics and/or treatment have any effect on the development of glaucoma.
Perhaps unsurprisingly, SS had the highest prevalence of OC, with dry eye occurring in nearly 9 in 10 patients, since dryness is associated with lymphocytic infiltration of lacrimal glands and reduced tear clearance caused by surface inflammation25,26. Dry eye is one of the most common manifestations of SS, so assessments of disease activity typically include OC and dry eye27,28. This pattern holds true for other CTD in which OC are less common. Assessments for disease activity in SLE and GPA all include metrics for eye involvement29,30,31,32. In sarcoidosis, diagnosis often occurs if there is lung involvement, but it can also be based on a biopsy of diseased skin or lymph nodes in conjunction with extrapulmonary symptoms, such as uveitis33,34. Geographic differences in OC have also been reported in sarcoidosis, with higher prevalence in East Asian populations35.
As with other metaanalyses of this nature, limitations to our study included high heterogeneity between the included studies, possibly due to different patient populations and nonstandardized definitions of OC. We assumed that there would be heterogeneity of definitions for each eye manifestation between publications, so we used the terms “ocular manifestations,” “involvement,” and “complications” virtually interchangeably to account for discrepancies across the studies. OC due to disease activity and ocular damage were included in our search; however, studies with a low prevalence of OC might not have been included in these publications, potentially resulting in publication bias. Our work was also limited in establishing the true cross-sectional prevalence of OC in each condition because individual cohorts did not all adjust for disease duration or activity. Most studies did not separate age at onset, so there could be differences in the frequency of various ocular manifestations, depending on the age of the patient (i.e., adults vs children). A previous publication compared the frequency of eye manifestations in various childhood rheumatic diseases; we did not include information about SpA/other arthropathy comparisons between adult and paediatric disease36. In addition, some OC may be due to a rheumatic disease itself, and some due to its treatment, further hindering our ability to accurately determine the cross-sectional prevalence of OC.
In conclusion, our metaanalysis determined the prevalence of OC across the spectrum of several rheumatic diseases. OC were most common in SS, occurring in 89% of patients, followed by APS, SLE, GCA, sarcoidosis, and GPA, in which OC occurred in 26–35% of patients. OC occurred in approximately 18% of patients with RA, highlighting it as a common extraarticular manifestation of the disease.
ACKNOWLEDGMENT
A special thank you to Brad Dishan (librarian/information specialist) for his help with our literature search.
Footnotes
This study was supported through the Canadian Rheumatology Association Roche summer studentship.
- Accepted for publication February 18, 2020.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}