

Abstract
Objective. Youth with systemic lupus erythematosus (SLE) transferring from pediatric to adult care are at risk for poor outcomes. We describe patterns of rheumatology/nephrology care and changes in healthcare use and medication adherence during transfer.
Methods. We identified youth ages 15–25 with SLE using US private insurance claims from Optum’s deidentified Clinformatics Data Mart. Rheumatology/nephrology visit patterns were categorized as (1) unilateral transfers to adult care within 12 months, (2) overlapping pediatric and adult visits, (3) lost to followup, or (4) continuing pediatric care. We used negative binomial regression and paired t tests to estimate changes in healthcare use and medication possession ratios (MPR) after the last pediatric (index) visit. We compared MPR between youth who transferred and age-matched peers continuing pediatric care.
Results. Of the 184 youth transferred out of pediatric care, 41.8% transferred unilaterally, 31.5% had overlapping visits over a median of 12 months before final transfer, and 26.6% were lost to followup. We matched 107 youth continuing pediatric care. Overall, ambulatory care use decreased among those lost to followup. Acute care use decreased across all groups. MPR after the index date were lower in youth lost to followup (mean 0.24) compared to peers in pediatric care (mean 0.57, p < 0.001).
Conclusion. Youth with SLE with continuous private insurance coverage do not use more acute care after transfer to adult care. However, a substantial proportion fail to see adult subspecialists within 12 months and have worse medication adherence, placing them at higher risk for adverse outcomes.
- pediatric systemic lupus erythematosus
- longitudinal studies
- outcome assessment
- patient compliance
- epidemiology
Pediatric-onset systemic lupus erythematosus (pSLE) is a lifelong autoimmune condition with a high healthcare burden and greater risk of mortality and organ damage compared to adult-onset disease1,2,3. Youth with pSLE may be particularly vulnerable when transferring care from pediatric to adult health systems. Previous studies have demonstrated higher in-hospital mortality and hospital readmission rates among transition-age youth with SLE compared to children or older adults with SLE4,5. These findings are potentially mediated by gaps in care and medications during transfer to adult care6,7.
Although transfer to adult care has been linked to worse outcomes in other chronic pediatric conditions, such as sickle cell disease and juvenile-onset diabetes8,9, there are very few studies on transfer outcomes among young adults with pSLE. Further, there is a relative paucity of literature regarding the third and final phase of transition, when young adults begin engaging with adult healthcare systems10. Timeliness of the first visit to adult care after discharge from pediatric care is a key indicator of successful transfer11. However, it remains challenging to quantify or assess the effect of gaps in care among geographically mobile young adults because of challenges linking data between pediatric and adult healthcare systems. Consequently, prior studies of transition outcomes among youth with pSLE have focused on transfers from or to a single-center institution12,13,14. Since practice-based transition models range from no systematic approach to dedicated adolescent clinics and combined pediatric/adult transition clinics10,15,16, population-based studies can better approximate what occurs in real-world settings.
Administrative data present a unique opportunity to evaluate patterns of transfer at a national level. In addition, relevant outcomes of transfer such as emergency department visits, hospitalizations, frequency of ambulatory care, and medication prescription fills are well identified. Therefore, the objectives of this study were to (1) describe patterns of transfer from pediatric to adult rheumatology/nephrology in youth with pSLE, (2) compare healthcare use before and after the last pediatric subspecialty visit, and (3) compare rates of medication adherence by subspecialty transfer pattern. We hypothesized that youth who fail to see an adult subspecialist within 12 months of the last pediatric visit would have decreases in overall ambulatory care use and increases in acute care use, as well as lower medication adherence than those with timely transfers to an adult provider.
MATERIALS AND METHODS
Study population. We identified SLE cases with ≥ 12 months of continuous enrollment at age 15–25 years in Optum’s de-identified Clinformatics Data Mart Database, which is derived from a national, commercial health insurer covering about 20% of US residents from 2000 to 2016. The database contains deidentified patient-level demographics, billable healthcare encounters, encounter-level diagnosis and procedure codes, and prescription drug fills. Pediatric and adult subspecialties are defined by provider category codes. Because reimbursement is tied to claims, use is well recorded.
SLE was defined by the presence of ≥ 3 International Classification of Diseases-9-Clinical Modification (ICD-9-CM; 710.0) or ICD-10-CM (M32.1x, M32.8, M32.9) diagnosis codes for SLE, each at least 30 days apart17,18. SLE cases were required to have ≥ 1 physician claim from a nephrologist or rheumatologist. Youth remaining exclusively in pediatric rheumatology/nephrology care throughout enrollment were randomly sampled with replacement and frequency-matched by age with youth who transferred to adult care or were lost to followup. Because of the deidentified feature of the dataset, an exemption was approved for our study by the institutional review boards of the Children’s Hospital of Philadelphia and the University of California San Francisco (18-25472), which means written consent and approval by a research ethics board were not required.
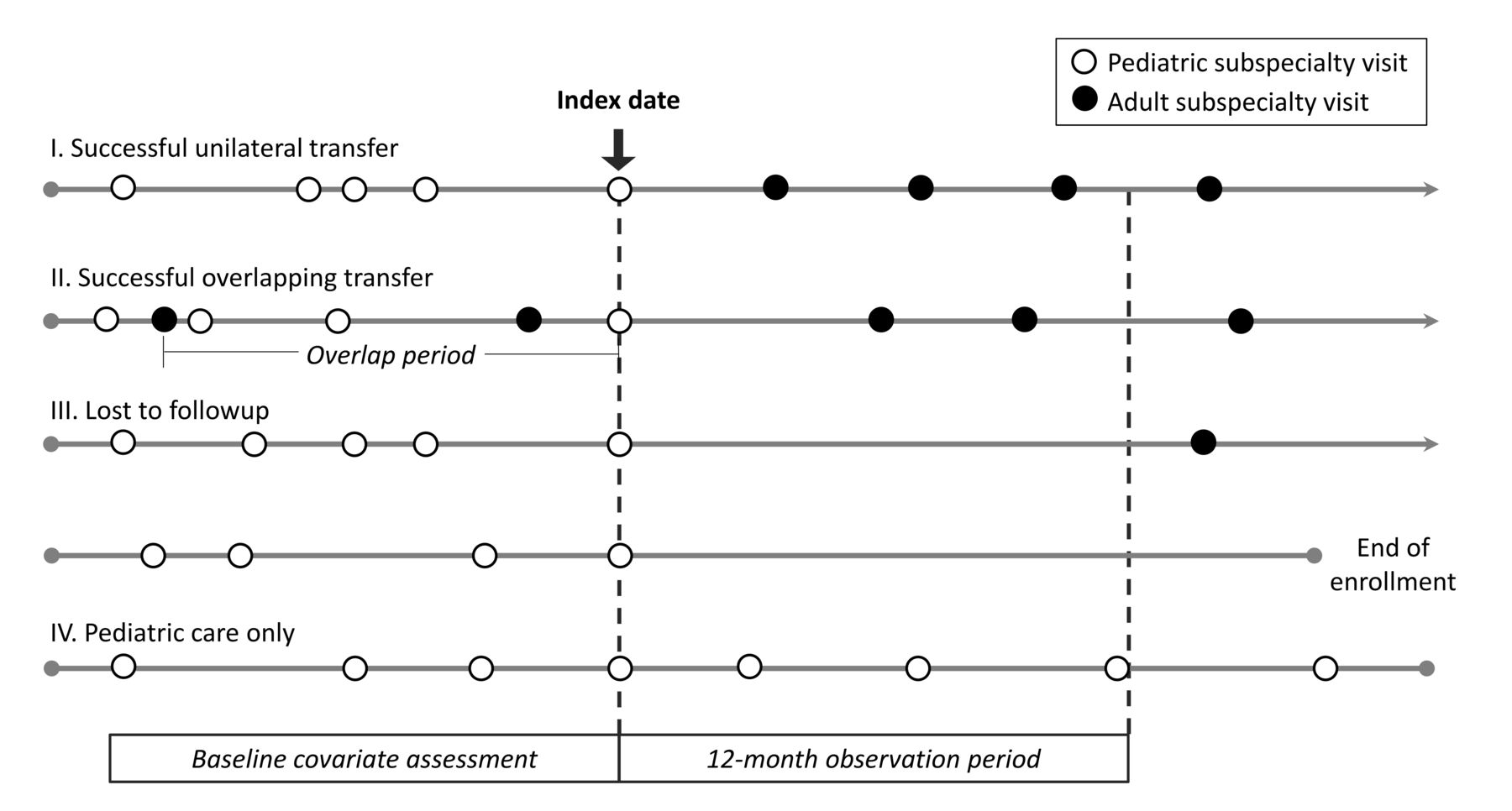
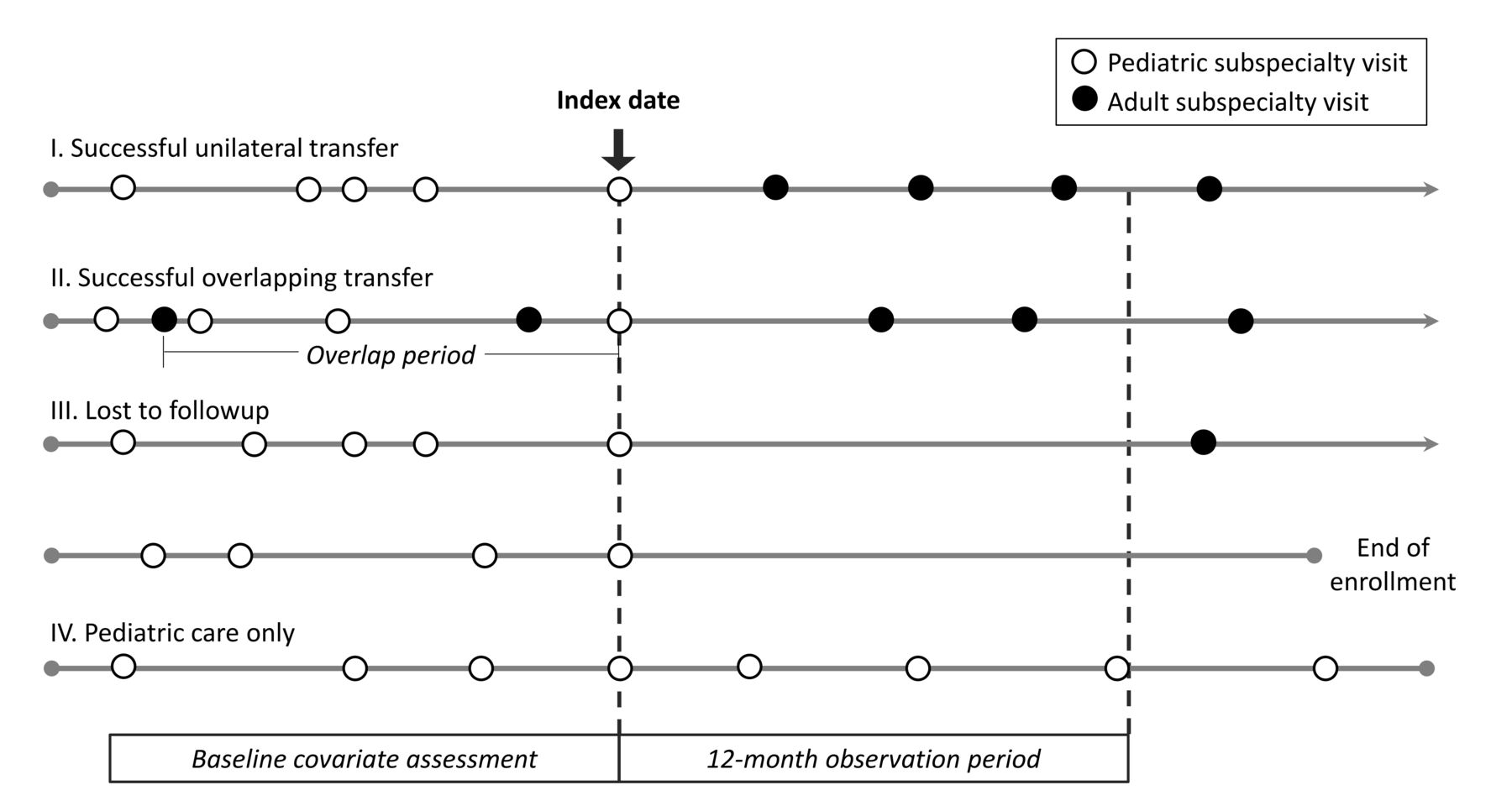
Study measures. Successful transfers were defined by the occurrence of an adult rheumatology/nephrology visit within 12 months after the last pediatric subspecialist visit. Youth were categorized by pattern of rheumatology and nephrology subspecialty care as follows: (1) successful unilateral transfer from a pediatric to adult subspecialist, (2) successful transfer with overlapping pediatric and adult visits preceding final transfer to adult care (with < 12 mo between the last pediatric and subsequent adult visit), (3) lost to followup (> 12 mo between the last pediatric visit and first adult visit or end of enrollment), or (4) continuing pediatric care throughout enrollment without seeing an adult subspecialist (Figure 1). As a descriptive reference, we also characterized a fifth group that received only adult care. For youth in each of the 3 transfer groups, the last pediatric visit during enrollment was considered the index date (Figure 2). For those continuing pediatric care, the index date was the age-matched pediatric visit. A minimum of 6 months of eligibility before and after the index date were required for inclusion. By definition, those categorized as lost to followup had ≥ 12 months of eligibility after the index date.

Categorization of ambulatory rheumatology and nephrology healthcare use patterns among transition-age youth with SLE. Successful transfer of care was defined as < 12 months between the last pediatric visit and the first adult visit during the eligibility period. *Sampled with replacement from youth remaining in pediatric care throughout enrollment. SLE: systemic lupus erythematosus.
Categorization of systemic lupus erythematosus subspecialty transfer patterns and age-matched peers continuing pediatric care. Outcomes were assessed during the observation period up to 12 months after the index date.
The primary healthcare use outcomes were the rate of all ambulatory encounters (primary and specialty care) and acute care encounters (emergency/urgent care visits and hospitalizations) in the year following the index date. Medication adherence among prevalent hydroxychloroquine (HCQ) users was estimated using prescription fill data to calculate HCQ medication possession ratios (MPR), defined as the number of days’ supply over total observation days in the year following the index date (excluding hospital days from numerator and denominator). Prevalent use was defined by the presence of ≥ 1 HCQ prescription fill preceding the index date.
Covariates of interest included demographic characteristics (age at index date, sex, race/ethnicity, geographic region, highest household education), disease characteristics preceding the index date as proxies for disease severity (nephritis, dialysis/transplant, central nervous system involvement defined by seizure or stroke, psychiatric diagnosis, as previously described)19, as well as baseline MPR and ambulatory/acute care use in the year preceding the index date. Time between the first adult and last pediatric visit was assessed in youth with overlapping care.
Statistical analysis. Demographics, disease characteristics, and baseline use rates were assessed using standard descriptive statistics and compared across transfer groups using chi-square tests for categorical variables and Kruskal-Wallis tests for continuous variables. Multinomial logistic regression was used to identify baseline characteristics independently associated with each transfer group. Differences between transfer groups were tested using likelihood ratio tests.
Negative binomial regression was used to estimate incidence rate ratios (IRR) comparing use rates during the observation period to baseline use. MPR before and after the index date were compared within transfer groups using paired t tests. Two-sample t tests were used to compare MPR in each transfer group to age-matched peers continuing pediatric care.
We performed several sensitivity analyses. To address potential ascertainment bias in IRR and MPR estimates, we limited the sample to subjects with at least 1 encounter or prescription fill during the observation period. To address asynchronous transfers by subspecialty, we re-ran the multinomial logistic regression analysis in those with observation periods defined using pediatric and adult providers within the same subspecialty (rheumatology or nephrology).
RESULTS
Transfer patterns and baseline characteristics. We identified 184 youth who transferred out of pediatric subspecialty care, of whom 77 (41.8%) transferred unilaterally to adult care within a year, 58 (31.5%) had successful overlapping transfers, and 49 (26.6%) were lost to followup. Of the 226 youth remaining in pediatric care, 107 were age-matched to the transfer groups using the index date. Among the youth who transferred, 18% (33/184) were black, 11% (20/184) were Hispanic, and 7% (13/184) were Asian. Baseline characteristics were well balanced between youth in each transfer group and their age-matched peers in pediatric care, save for longer eligibility after the index visit and fewer minorities in the group lost to followup (Supplementary Table 1, available with the online version of this article). There was also an increased proportion of youth from the Midwest with overlapping successful transfers compared to pediatric matches (29% vs 16%, p = 0.03).
The mean age at the index date was 18.4 (SD 2.1). On average, youth with successful unilateral transfers to adult care were older at the index date than those with successful overlapping transfers or those lost to followup (mean age 19.4 yrs vs 18.7 and 18.5, respectively, p = 0.02; Table 1). Median time between the index date and first adult visit was 99 days [interquartile range (IQR) 50–225] among unilateral transfers, compared to 577 days (IQR 453–936) among youth lost to followup who saw an adult subspecialist before the end of enrollment (n = 34). In youth with successful overlapping transfers, the median period of overlap between the first adult and last pediatric visit was 12 months (IQR 4–27), and the median time from the index date to the next adult visit was 35 days (IQR 12–96). Of note, 21 patients (43%) who were lost to followup also had 1 or more adult subspecialty visits before the index date with a median overlap of 22 months (IQR 8–37).
Baseline characteristics by transfer group.
Among 120 youth whose index visit was with pediatric rheumatology, the majority of transfers were to adult rheumatology (96%, 86%, and 96% in the unilateral transfer, overlapping transfer, and lost-to-followup groups, respectively). Among the 58 subjects whose index visit was with pediatric nephrology, 11/20 (55%) unilateral transfers were to adult nephrology, compared to 2/21 (10%) of overlapping transfers and 4/17 (24%) of those lost to followup. The remainder of transfers were to adult rheumatology.
Predictors of subspecialty transfer pattern. Age at index date, geographic region, and baseline ambulatory care use rates were independently associated with transfer pattern (Supplementary Table 2, available with the online version of this article). Each 1-year increase in age at the index visit was associated with a significantly lower likelihood of belonging to either the successful overlapping transfer group or the lost-to-followup group, relative to the unilateral transfer group [relative risk ratio (RRR) 0.82, p = 0.04 and 0.80, p = 0.03, respectively]. In contrast, living in the Midwest instead of the Northeast was independently associated with a > 5-fold increased risk of being lost to followup relative to unilateral transfer (RRR 5.52, p = 0.03). The relative risk of overlapping instead of unilateral successful transfers was higher in the Midwest compared to both the Northeast (RRR 7.96, p < 0.01) and the South (RRR 5.22, p < 0.01). Higher baseline ambulatory care use was associated with overlapping transfer, in keeping with how this group was defined (p = 0.01). Race/ethnicity, sex, and the presence of major organ manifestations or psychiatric diagnoses were not significantly associated with transfer pattern (Supplementary Table 2). Upon restricting the analysis to transfers between pediatric and adult providers within the same subspecialty, we identified the same predictors of transfer pattern.
Healthcare use outcomes. After the index date, ambulatory visit rates decreased by 0.7-fold among youth lost to followup or with overlapping successful transfer (p < 0.01; Figure 3A), but remained unchanged among those with unilateral transfers or those continuing pediatric care (Table 2). Rates of acute care use decreased across all groups, including those continuing pediatric care (IRR 0.14–0.30, p < 0.01; Figure 3B).

A. Incidence rate ratios representing within-group comparisons of posttransfer to pretransfer rates of ambulatory care use. B. Incidence rate ratios representing within-group comparisons of posttransfer to pretransfer rates of acute care use, including emergency department visits and hospitalizations.
Healthcare use during transfer period compared to pretransfer.
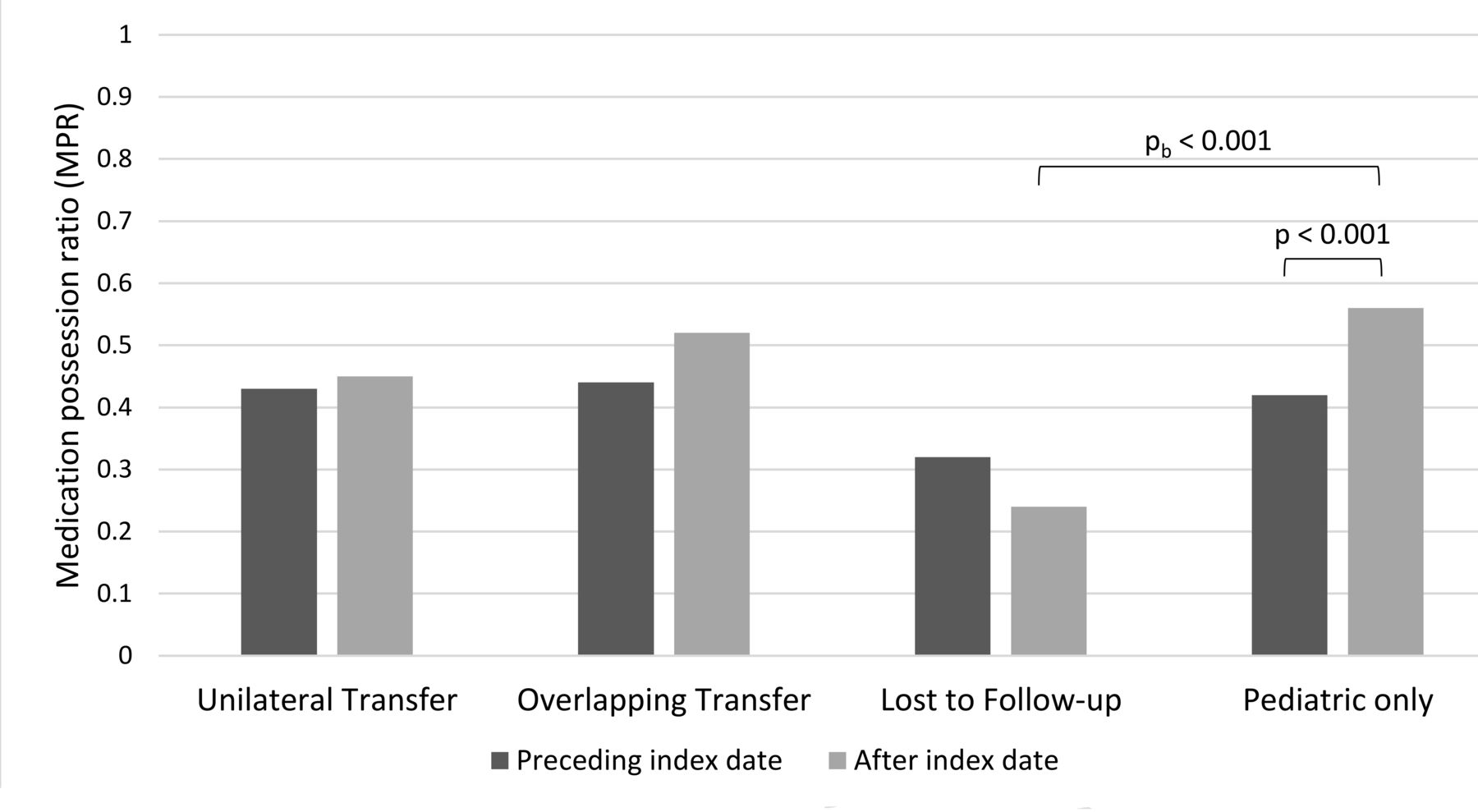
Medication adherence outcomes. HCQ MPR were low across all transfer groups, with a mean MPR of 0.40 (SD 0.36) at baseline and 0.42 (SD 0.35) during the observation period. Youth who were lost to followup had the lowest MPR before and after the index date (Figure 4). There was a trend toward a 25% decrease in average MPR after transfer among youth lost to followup, albeit not statistically significant (p = 0.096). In contrast, those remaining in pediatric care had a 33% increase in mean MPR after the index date (p < 0.001), and MPR for unilateral transfers remained unchanged. For reference, peers who received only adult care with an SLE code before the age of 18 had an average MPR of 0.45 (SD 0.35) at 1 year of followup, which remained stable at 0.44 (SD 0.33) after 2 years of followup.
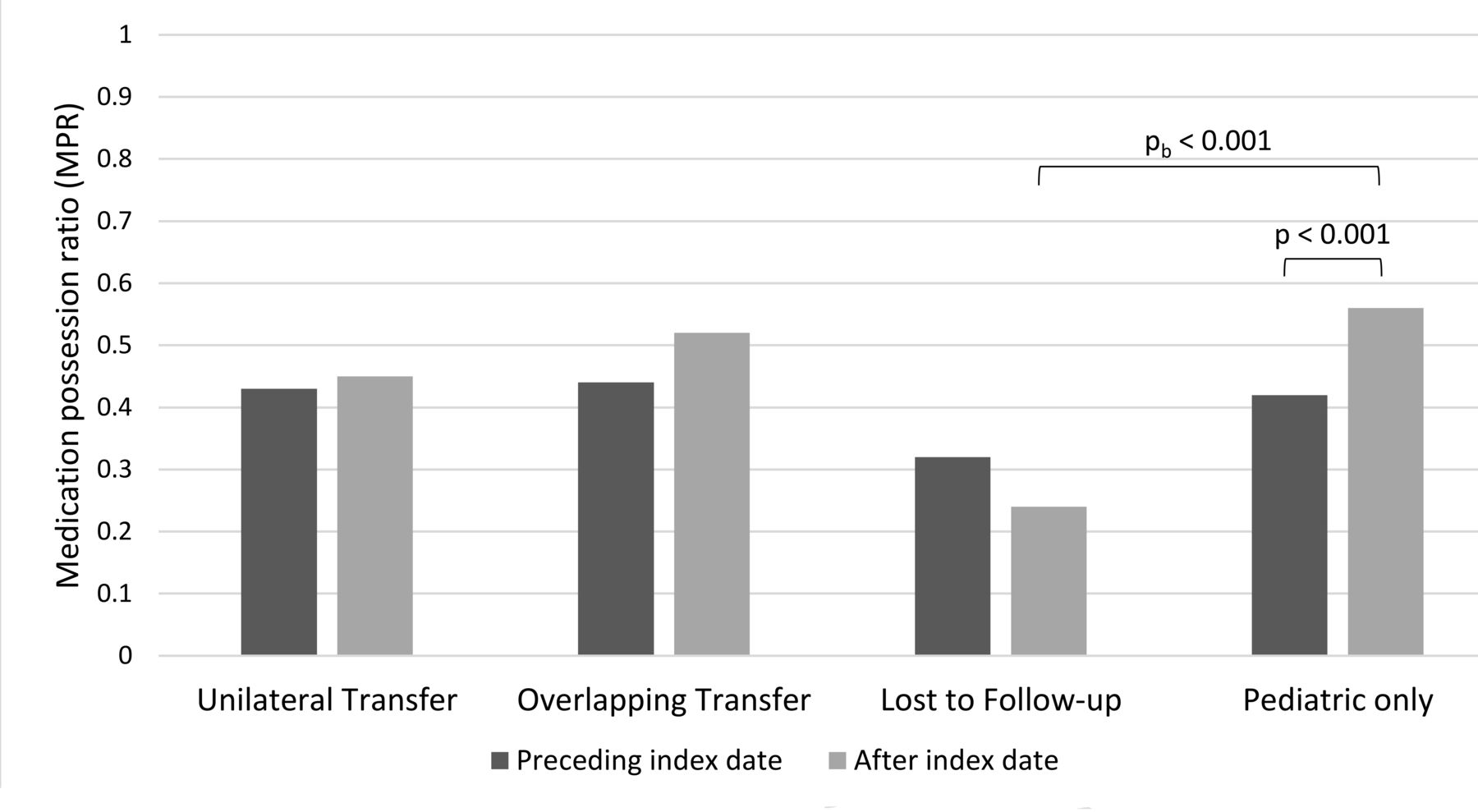
Comparison of average medication possession ratios (MPR) 1 year before and after transfer using paired t tests. Between-group differences were tested using 2-sample t tests; their statistically significant differences are shown (pb).
The mean MPR after the index date was significantly lower in the lost-to-followup group compared to age-matched peers remaining in pediatric care (pb < 0.001). There were no significant differences in postindex date MPR among unilateral or overlapping successful transfers and peers remaining in pediatric care.
There were only 2 subjects in the lost-to-followup group who did not have any healthcare encounters or SLE-related prescription fills during the observation period. Exclusion of these subjects did not significantly change IRR estimates (IRR 0.71 for ambulatory visits, 95% CI 0.54–0.94, and 0.14 for acute care, 95% CI 0.04–0.43) or MPR (mean pre- and post-MPR 0.33 and 0.25, respectively).
DISCUSSION
In our population-based study of transfer outcomes among youth with SLE in the United States, a quarter of youth failed to see an adult rheumatologist or nephrologist within 12 months of their last pediatric subspecialty visit, despite uninterrupted health insurance coverage and relatively high household educational attainment. Those who were lost to followup had the lowest ambulatory care use and medication adherence during the observation period. Although gaps in care and decreases in medication adherence did not correspond with short-term increases in acute care use, the high risk of morbidity and excess mortality in young adults with SLE underscores the importance of ongoing evaluation of medication adherence and followup care in this age group. Our findings highlight the need for coordinated transfer planning as part of the transition process and can inform improvement strategies by identifying individuals who are most likely to require additional support when transferring from pediatric to adult SLE care.
Seeing an adult provider within an appropriate timeframe has been considered one of the key indicators of successful transition11,20,21. In addition, a shorter interval between the last pediatric and first adult visit is associated with a higher likelihood of establishing consistent adult care22. In our study, failure to see an adult subspecialist within 12 months was associated with decreases in rates of overall ambulatory care use and medication adherence. Although maintaining access to health care is critical, our results emphasize that continuous insurance coverage alone will not ensure timely visits to adult care. Similar observations have been made among pediatric rheumatology practices in settings with universal healthcare models, such as the United Kingdom and Canada23,24. These findings support the need for systematic approaches to confirm timely transfer completion25.
We identified several risk factors that can help clinical teams focus interventions and resources on youth with SLE who are most likely to experience prolonged gaps in care. Those with less frequent ambulatory care at baseline were more likely to be lost to followup. This has also been observed in primary care settings, in which low transfer completion was associated with difficulties bringing youth back to the pediatrician to facilitate transfer26. Population management strategies to monitor high-risk patients and ensure frequent visits during transfer planning remain important opportunity areas. Other risk factors for untimely transfers included geographic region, which could reflect regional rheumatology workforce shortages27. Regional variation in health outcomes can also suggest opportunities for standardization, though more granular data are needed to direct improvement efforts28. Last, older age was a determinant of successful unilateral transfer, which is consistent with findings in other chronic conditions and may relate to differences in levels of social and emotional maturation29. There has been significant attention toward assessment of transition readiness, which more specifically identifies skills and behaviors needed for healthcare independence than chronologic age25,30. However, transition readiness scores from existing tools have yet to be correlated with better transfer outcomes31. Additional predictors of transfer success, including baseline healthcare use, access issues, and socioeconomic factors, will be important to consider in addition to transition readiness when determining the right age for transfer to adult care.
Various periods of overlapping pediatric and adult care were common and not explained by asynchronous rheumatology/nephrology transfers. Changes in ambulatory care use are difficult to assess in this group, because decreased visits after discharge from pediatric care was partly a consequence of how the group was defined. Differences in presence and duration of overlap likely reflect variation in transitional practice models32. Meeting adult providers before transfer is associated with better transition outcomes in other chronic diseases33, and “transition clinics” where adult rheumatologists see patients with the pediatric team have been described16. However, experience suggests young adults may return to pediatric care because of negative experiences in adult-centered care34. In our study, overlapping care occurred with the same frequency in successful and unsuccessful transfers; therefore the reasons for overlap (i.e., practice vs patient-driven) may be more important determinants of success. The observed regional differences despite similar rates of major organ involvement suggest practice norms likely contribute to overlap; however, there were no practice-level indicators to assess preference-based drivers. Further research is needed to understand reasons for and effect of overlapping care.
Medication adherence is another component to key indicators of successful transition, including self-management and maintenance of disease control35. In our study, baseline levels of adherence to HCQ were low across the entire cohort. Adherence became significantly lower in those lost to followup compared to age-matched peers remaining in pediatric care, while adherence remained stable among youth with timely unilateral or overlapping transfers. In the juvenile diabetes literature, transfer was associated with worse glycemic control compared to remaining in pediatric care9; however, our results suggest that timely transfers may be protective in pSLE. Low overall adherence rates in pSLE may be due to a combination of factors, including concerns about side effects, direct effects of SLE on neurocognition, mood disorders36, poor adaptation/coping with illness37, and delayed maturation of self-management skills because of onset of chronic illness in childhood, including deficits in ordering prescription refills6,38,39,40. In addition, prolonged gaps in care during transfer can result in lapses in prescription supply, so clinical teams should ensure that primary prescribers are clearly delineated during transfer. Previous studies have demonstrated that damage accrual from pSLE continues through adulthood41,42, and onset of SLE in childhood is an independent predictor of excess mortality in young adults with SLE, emphasizing the importance of ongoing evaluation of medication adherence3.
Contrary to our initial hypothesis, one somewhat reassuring finding from our study was that acute care use decreased during transfer to adult SLE care among youth with uninterrupted insurance coverage. There are several potential explanations. First, pediatric subspecialists may wait to transfer patients with SLE during periods of disease stability, particularly if formal transfer planning processes have been implemented13,43. Second, acute care use among patients with SLE has been shown to decline with disease duration, which could drive our results44. Third, a decreased frequency of overall acute care encounters may be driven by a reduction in scheduled hospitalizations for infusions after transfer to adult care, as demonstrated in 1 academic center13. Last, our observation period was relatively short, so it is possible that a longer latency period following transfer is needed to observe increased acute care use as an effect of prolonged gaps in care or medication nonadherence. Adolescents with other chronic conditions also demonstrate relative stability of short-term patterns of healthcare use during transfer to adult care45, but data on longterm patterns of acute care use are needed.
There are several strengths to our study. To our knowledge, this is the largest and only population-based study of transfer outcomes among youth with pSLE in the United States. More importantly, we were able to measure outcomes across healthcare institutions and state lines. We also identified several important factors associated with becoming lost to followup that can guide targeted interventions when resources to support transition are more limited, as is often the case. There were also several limitations to our approach. First, we were unable to assess disease activity or psychosocial factors, which are important individual-level determinants of healthcare use. Second, we were unable to assess the effect of gaps in insurance coverage, which affect up to one-third of patients with pSLE transferring to adult care12. Last, our results need to be interpreted in the context of commercial insurance enrollees, which underrepresent minorities and families with lower socioeconomic status. Only 18% of our cohort was black compared to 34% in a national registry and 40% in Medicaid enrollees18,46. Racial and socioeconomic disparities exist in both disease severity and outcomes36,47,48, and therefore our findings have limited generalizability to publicly insured or uninsured individuals who are at higher risk for poor outcomes49,50. Transition outcomes research in Medicaid enrollees poses separate methodologic challenges from loss of eligibility upon reaching adulthood, and it remains an important area for further study.
Access to continuous insurance coverage is necessary but not sufficient to ensure successful transfer to adult care among young adults with SLE. Transition interventions and resources should be targeted toward youth who are at the highest risk for being lost to followup after discharge from pediatric subspecialty clinics. Particular attention is needed to ensure adequate ambulatory followup care and medication adherence during transition and confirm transfer completion. Adult SLE subspecialists should consider routine assessment of medication adherence in recently transferred young adults. Our study highlights the need for future research to include outcome assessment during the third phase of transition. Additional data are needed to determine whether interventions targeting healthcare use and medication adherence patterns during transfer improve longitudinal health outcomes.
ACKNOWLEDGMENT
We thank Craig W. Newcomb, MS, and Qing (Jean) Liu for data management and programming services.
Footnotes
This work was funded by the US National Institute of Arthritis and Musculoskeletal and Skin Diseases, the Childhood Arthritis and Rheumatology Research Alliance, and the Arthritis Foundation. Support for JC from US National Institutes of Health grant F32HL142176.
- Accepted for publication January 10, 2020.
REFERENCES
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.








{kind=link}
{kind=link}
{kind=link}
{kind=link}