

To the Editor:
Brain magnetic resonance imaging (MRI) findings in craniofacial morphea including en coup de sabre (ECDS) localized scleroderma and Parry-Romberg syndrome (PRS; progressive facial hemiatrophy) are not unusual1, but the relevance of rare abnormalities is unknown. We report 2 cases in which distant cerebellar lesions on brain MRI occurred with varying clinical neurologic manifestations.
Ethics approval was not required by the University of Calgary Conjoint Health Research Ethics Board because clinical case series do not fall within the definition of research in the second edition of the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS 2). Consent to report the cases and clinical images were obtained from the patients and their families.
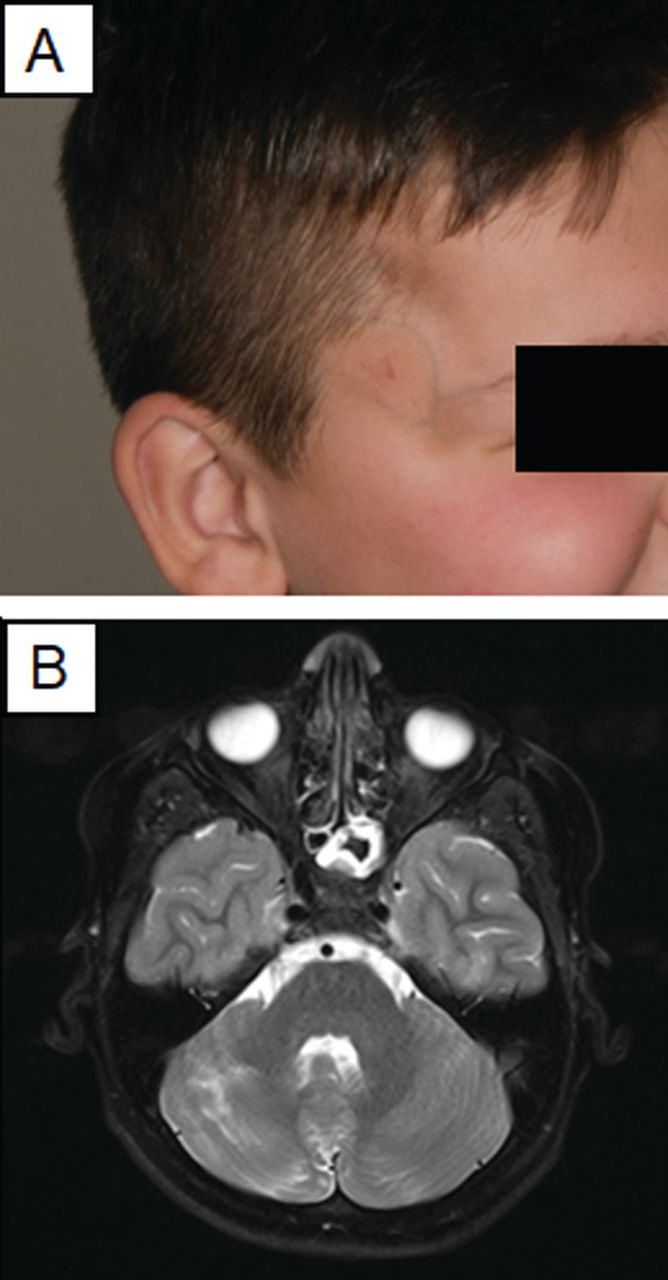
Case 1 involves a 10-year-old male who presented with a 5-year history of linear, atrophic, indurated, sclerotic, hyperpigmented, and slightly erythematous plaques involving the right frontotemporal scalp, right forehead, and right temple (Figure 1A). Prior skin biopsy was consistent with morphea (ECDS scleroderma variant). Topical corticosteroids did not provide benefit. Review of systems and neurologic assessment were unremarkable. Repeat skin biopsy revealed active inflammation and laboratory studies showed positive antinuclear antibody (ANA; 1:40 titer). Baseline brain MRI demonstrated right-sided cerebellar hemiatrophy with associated right cerebellar parenchymal enhancement (Figure 1B). He was subsequently treated with systemic immunosuppressive therapy [intravenous methylprednisolone 30 mg/kg for 3 days repeated monthly for 3 months, and oral methotrexate (MTX) 20 mg weekly]. Repeat MRI one year later showed no interval progression of cerebellar atrophy but slight improvement to the previously noted cerebellar enhancement.
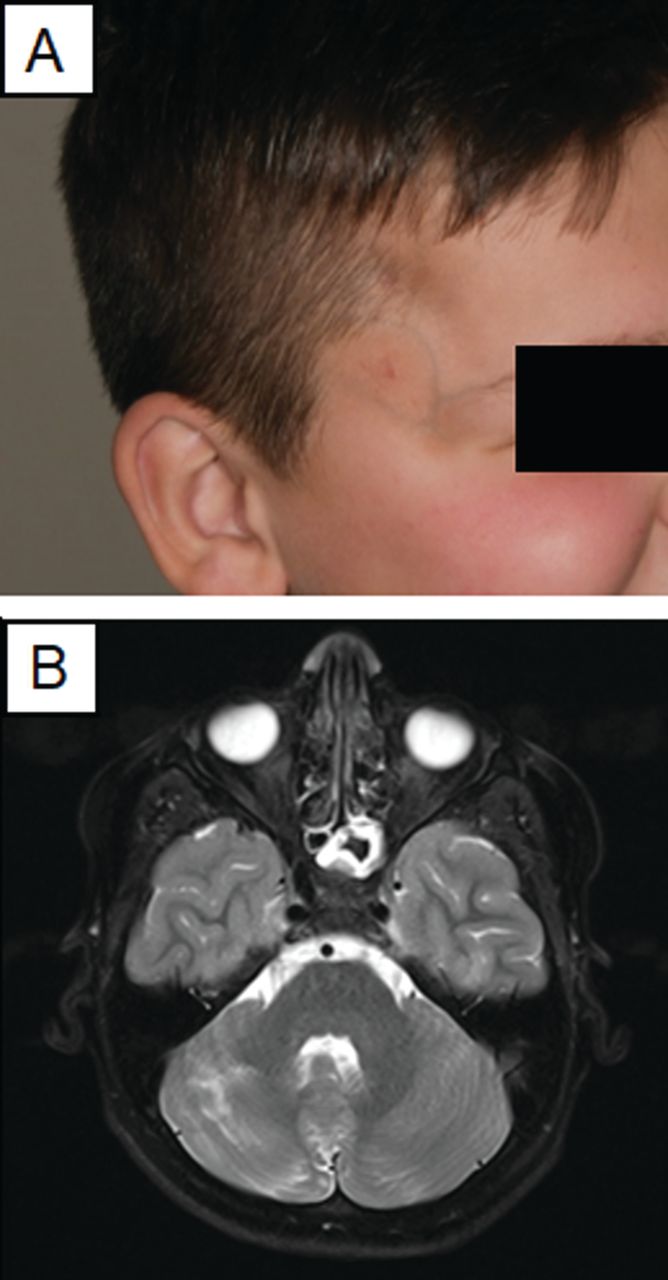
Case 1. A. Clinical image showing atrophic, indurated, hyperpigmented, and slightly erythematous plaques involving the scalp and face, consistent with en coup de sabre scleroderma subtype of linear morphea. B. Axial T2-weighted post-gadolinium MRI image showing subtle right cerebellar hemisphere atrophy compared to the left cerebellar hemisphere, with associated parenchymal enhancement in the right cerebellar hemisphere. MRI: magnetic resonance imaging.
Case 2 is a 17-year-old female with a presumptive diagnosis of lipodystrophy who presented with a 15-year history of atrophic, sclerotic, indurated, hypopigmented plaques involving the trunk and extremities (lesions traversed the left elbow, wrist, and hand, plus right hip, knee, ankle, and foot joints). She was noted to have right facial asymmetry, right tongue atrophy, and right microtia (Figure 2A). Dysmetria, difficulty with tandem gait, slightly reduced left upper and right lower extremity muscle strength, and significant left upper extremity muscle atrophy were observed. Joint range of motion was normal. Multiple skin biopsies from the right lower extremity revealed subcutaneous fat atrophy without significant inflammation. Laboratory studies showed positive ANA (1:80 titer) as well as positive anti-Th/To and weakly positive anti-PM/Scl-75 antibodies, with negative multigene lipodystrophy panel. A diagnosis of linear morphea involving the head (PRS variant), trunk, and extremities was made. Baseline brain MRI demonstrated significant cerebellar atrophy, including the vermis, without parenchymal changes as well as a slightly smaller right cerebral peduncle compared to the left with right-sided cerebral volume loss. The patient was subsequently treated with oral MTX 20 mg weekly. Minimal progression of cerebellar and brainstem atrophy, but slight progression of cerebral atrophy was observed on repeat brain MRI one year later (Figure 2B).

Case 2. A. Clinical image showing subtle right facial asymmetry and significant right tongue atrophy, consistent with Parry-Romberg syndrome subtype of linear morphea. B. Sagittal T1-weighted MRI showing significant vermian atrophy. MRI: magnetic resonance imaging.
Morphea (localized scleroderma) is rare with an incidence of about 1–3 per 100,0002, making systematic study of craniofacial morphea variants such as ECDS scleroderma and PRS very challenging. In an international retrospective chart review of 750 cases, 113 (23%) had involvement of the head. Of these, 21 (18%) had neurologic symptoms or neuroimaging abnormalities1. Brain MRI findings most commonly identified in ECDS scleroderma/PRS include bone/soft tissue thinning, T2-weighted hyperintensities, calcification, and atrophy3. When localized below the site of cutaneous disease, direct morphea extension to underlying structures could be a proposed mechanism. However, most neuroimaging reports of ECDS scleroderma/PRS patients suggest brain lesions are often distant from the site of cutaneous disease and do not correlate well with clinical symptoms3,4,5, raising the question of whether these distant neuroimaging findings are caused by, associated with, or independent of the morphea.
While few prior cases of cerebellar hyperintensities and focal scalp atrophy have been reported in morphea3,4,5, to our knowledge, cerebellar atrophy with longitudinal MRI followup have not been documented previously. From our cases, it is unclear whether brain MRI findings occurred before, simultaneously with, or after onset of cutaneous disease, affecting our ability to draw temporality. While an autoimmune basis is believed for morphea, and distant cerebellar lesion biopsies in morphea patients have been in support of mild vasculitis4, the pathophysiological mechanism by which patients would have brain involvement that is distant rather than adjacent to the site of cutaneous disease remains unclear. An important consideration is that among general pediatric populations, as many as 25% may have incidental brain MRI findings, including 0.18% with focal hyperintensities6. Additionally, in Case 2, brain MRI findings progressed while cutaneous disease appeared inactive, but it is unclear whether this simply reflects poor central nervous system effect of the treatment (MTX), a different treatment threshold between cutaneous and neurological disease, or an alternate disease process entirely. Adding further complication, brain MRI findings improved over time in Case 1. Indeed, little agreement between skin morphology, neurologic abnormality, and immunologic variables has been found in patients with morphea7, yet some patients have experienced improvement of neurological disease with systemic immunosuppressive therapy8.
It is yet unclear whether there is a conclusive association between morphea and distant neuroimaging findings; however, these 2 cases with cerebellar abnormalities certainly raise the possibility. We advocate for further studies to gain insight on the incidence, patterns, and treatment response of neurologic symptoms and imaging abnormalities in craniofacial morphea patients, to guide clinical management.








{kind=link}
{kind=link}