

Abstract
Objective. To develop a consensus-based, standardized, short (< 3 min) clinical examination protocol to assess the multidimensional, orofacial manifestations of juvenile idiopathic arthritis (JIA).
Methods. The study was conducted by a multidisciplinary task force from the Temporomandibular Joint Juvenile Arthritis Working Group (TMJaw). The study used an acknowledged sequential approach involving (1) a global multidisciplinary online questionnaire study, (2) a systematic literature review and consensus meetings to identify items for inclusion, (3) pilot testing of included items, (4) test of reliability in 22 subjects with JIA by 4 examiners, (5) test of construct validity in a case-control study involving 167 subjects, and (6) establishment of final recommendations.
Results. Six items were recommended for the final examination protocol: (1) clinician-assessed pain location, (2) temporomandibular (TMJ) joint pain on palpation (open and closed mouth), (3) mandibular deviation at maximal mouth opening (≥ 3 mm), (4) maximal unassisted mouth opening capacity, (5) frontal facial symmetry, and (6) facial profile. All recommended items showed acceptable reliability and construct validity. The average mean examination time was 2 min and 42 s (SD ± 38.5 s).
Conclusion. A consensus-based, short clinical examination protocol was developed. The protocol takes less than 3 min to complete and provides information about orofacial symptoms, TMJ dysfunction, and dentofacial deformity. The standardized examination protocol is applicable to routine clinical care, as well as future research studies.
In recent years, increased attention has been paid to the consequences of temporomandibular joint (TMJ) arthritis in patients with juvenile idiopathic arthritis (JIA). TMJ arthritis is a frequent feature of JIA1,2,3.
TMJ involvement may lead to abnormal dentofacial development and significant orofacial disabilities, including chronic orofacial pain and reduced TMJ mobility and masticatory function4–10. The orofacial manifestations of JIA can have a severe effect on health-related quality of life that may persist into adulthood8,11,12,13. Gadolinium-enhanced magnetic resonance imaging (MRI) is currently the gold standard for diagnosing active TMJ arthritis3,7,14,15,16.
The clinical orofacial examination constitutes an essential component of the clinical assessment of individuals with JIA, and serves 4 equally important purposes: (1) the detection of clinical signs of active TMJ arthritis that should prompt further clinical and imaging investigations; (2) the detection of orofacial manifestations caused by previous TMJ arthritis (TMJ involvement); (3) the assessment of dentofacial growth and development in skeletally immature subjects; and (4) the assessment of the longitudinal progression of orofacial symptoms and dysfunction in patients who have already been diagnosed with active TMJ arthritis or TMJ involvement.
Contemporary orofacial examination techniques are based on validated criteria and indices such as the Research Diagnostic Criteria for Temporomandibular Disorders, the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD), and the Helkimo index17,18. However, these tools vary in their complexity and the time required for completion, and do not specifically focus on the orofacial manifestations of JIA. In 2017, general, consensus-based, recommendations were published for clinical orofacial examination in JIA19. However, to date, no JIA-specific, interdisciplinary, consensus-based protocol exists for the clinical orofacial examination in JIA.
The objective of our present study was to develop a consensus-based, standardized short clinical examination protocol to assess aspects of JIA-induced orofacial manifestations to be used routinely in the clinical setting and in future research studies. The examination protocol should be applicable to all healthcare providers regardless of educational background.
MATERIALS AND METHODS
The study was conducted by a task force from the Temporomandibular Joint Juvenile Arthritis Working Group (TMJaw). TMJaw (formerly known as “EuroTMjoint”) is an international, multidisciplinary research network dedicated to studying TMJ arthritis in JIA. The initial task force represented researchers from Europe and North America and consisted of 3 pediatric rheumatologists, 3 specially trained orthodontists, and 2 specialists in orofacial pain. Using a sequential-based approach, the present study included the following aspects20: (1) conceptual phase and preliminary decision making, (2) item generation, (3) pilot testing, (4) test of reliability, (5) test of construct validity, and (6) establishment of final recommendations.
Phase 1: Conceptual phase and preliminary decision making
Initially, the conceptual framework was defined by the task force. In phase 1, a global online questionnaire was created, asking about JIA management and approaches to the clinical orofacial examination in JIA. In February 2013, members on the mail distribution lists of the Pediatric Rheumatology Bulletin Board and TMJaw group were invited to participate in a questionnaire study using the Survey Monkey online platform (www.surveymonkey.com). This assessed the following: (1) respondent-related characteristics (professional background, practice setting, geographic location, self-reported expertise in clinical orofacial examination in JIA); (2) maximum amount of time that can be devoted to the clinical orofacial examination during a full-body examination; and (3) ranking of the 5 most important examination items to include in the clinical orofacial examination of patients with JIA. The outcome of the online survey was used to inform item generation.
Phase 2: Item generation
From April 2013 to January 2017 the task force developed general interdisciplinary consensus-based recommendations for orofacial examination in JIA19. Following acknowledged steps for the generation of consensus-based guidelines, this project involved a comprehensive systematic literature review and subsequent consensus meetings. The systematic literature review provided evidence to support inclusion of specific examination items relevant for clinical orofacial examination in JIA. Details about the systematic review and the results are presented in Stoustrup, et al (2017)19. The importance of each of the proposed examination items was assessed during a 3-round Delphi study completed by participants on the TMJaw mailing list. During a consensus meeting in Tampere, Finland, in April 2014, the task force used the Delphi study outcome to identify preliminary examination items for inclusion in a short clinical orofacial examination protocol.
Phase 3: Pilot testing
The task force created a clinical form that included the preliminary examination items together with detailed instructions on how to perform each clinical examination item. The feasibility and the clinical applicability of the form and instructions were tested at the Section of Orthodontics, Aarhus University, Denmark, from April 2014 until December 2016. The ongoing clinical pilot test led to modification of the examination form and the instructions. The task force decided on a final set of examination items in March 2017.
Phase 4: Test of reliability
In September 2017, subjects with JIA, followed at the Section of Orthodontics, Aarhus University were randomly selected and invited to participate in a reliability study to assess intrarater and interrater agreement of the proposed examination items. Inclusion criteria were as follows: (1) JIA diagnosis according to the International League of Associations for Rheumatology (ILAR) classification criteria21; (2) ≥ 7 years and ≤ 18 years of age; and (3) able to cooperate with the clinical orofacial examination. All subjects were examined by 4 raters: 2 pediatric rheumatologists (TH, MT) and 2 orthodontists (PS, TKP). Subjects were assessed in a random sequence, and were examined twice by all 4 raters, with a 1- to 3-h time lag between the first and the second examinations. Prior to the reliability study, a 3-h clinical calibration session, involving 5 patients, was conducted among the 4 raters.
Phase 5: Test of construct validity
To assess construct validity, intergroup differences were calculated for each of the examination items between consecutive subjects with JIA and a random group of age-matched non-JIA controls. The JIA group consisted of consecutive subjects seen at the Section of Orthodontics, Aarhus University in compliance with the inclusion criteria: (1) JIA diagnosis according to ILAR criteria21; and (2) ≥ 7 years and ≤ 18 years and compliant with the clinical orofacial examination. The control group consisted of non-JIA subjects followed at the pediatric dental municipal clinics in the districts of Syddjurs and Vesthimmerland, Denmark. Inclusion criteria for the non-JIA controls were ≥ 7 years and ≤ 18 years, and able to cooperate with the clinical orofacial examination.
Associations between the 2 groups were assessed following predefined hypotheses (H):
H1: Subjects with JIA have more frequent orofacial pain in comparison to age-matched non-JIA control subjects.
H2: Subjects with JIA demonstrate reduced mandibular function in comparison to non-JIA control subjects.
H3: Subjects with JIA demonstrate more severe dentofacial growth abnormalities in comparison to non-JIA subjects.
Phase 6: Establishment of final recommendations
The results of the field testing (reliability and construct validity) were used to establish the final recommendations. A consensus-driven approach was used, and all authors accepted the final recommendations.
Statistics
Descriptive statistics were computed. Multirater Cohen’s κ was calculated to assess reliability for categorical data. Intraclass correlations coefficient was calculated to assess reliability in quantitative data (maximal mouth opening). Construct validity was tested against the predefined hypotheses using chi-square tests for categorical data. The Fisher’s exact test was used in outcome variables with < 5 subjects in either the control group or the JIA group. An unpaired t test was used for intergroup difference for quantitative data (maximal mouth opening capacity). Construct validity was only accepted if all predefined hypotheses were accepted. The level of significance was p < 0.05.
Miscellaneous
The study was approved by the Danish Data Protection Agency (1-16-02-16-16 and Aarhus University 20016-051-000001) and conducted in agreement with Danish Health Authority regulations on noninterventional studies. Prior to inclusion, informed and signed consent was provided by all participants ≥ 15 years of age, or by their parents for participants below age 15. All examination items are approved for use in pediatric patients. The study adheres to TMJaw consensus-based standardized terminology22.
RESULTS
Conceptual phase and preliminary decision making
The online questionnaire was completed by 167 healthcare providers. The majority of the respondents were pediatric rheumatologists (85.6%) and orthodontists (6.6%; Figure 1A). Respondents represented the following continents: North America (56.6%), South America (6.5%), Europe (35.5%), and Australia and Oceania (1.2%). The vast majority were affiliated with academic hospitals (90.5%). The respondents rated their own experience with TMJ and orofacial examination as follows: no experience (1.2%), minimal experience (9.5%), average experience (44%), moderate experience (32.7%), and expert experience (12.5%). Respondents were asked to suggest important clinical examination items and to assess the maximal time needed to complete a clinical orofacial examination during a full-body examination: < 1 min (9.5%), 1–3 min (43.5%), 3–5 min (24.4%), 5–10 min (16.1%), > 10 min (6.5%; Figure 1B). Based on the results of the questionnaire, the task force decided on a 3-min time limit for the final examination protocol.
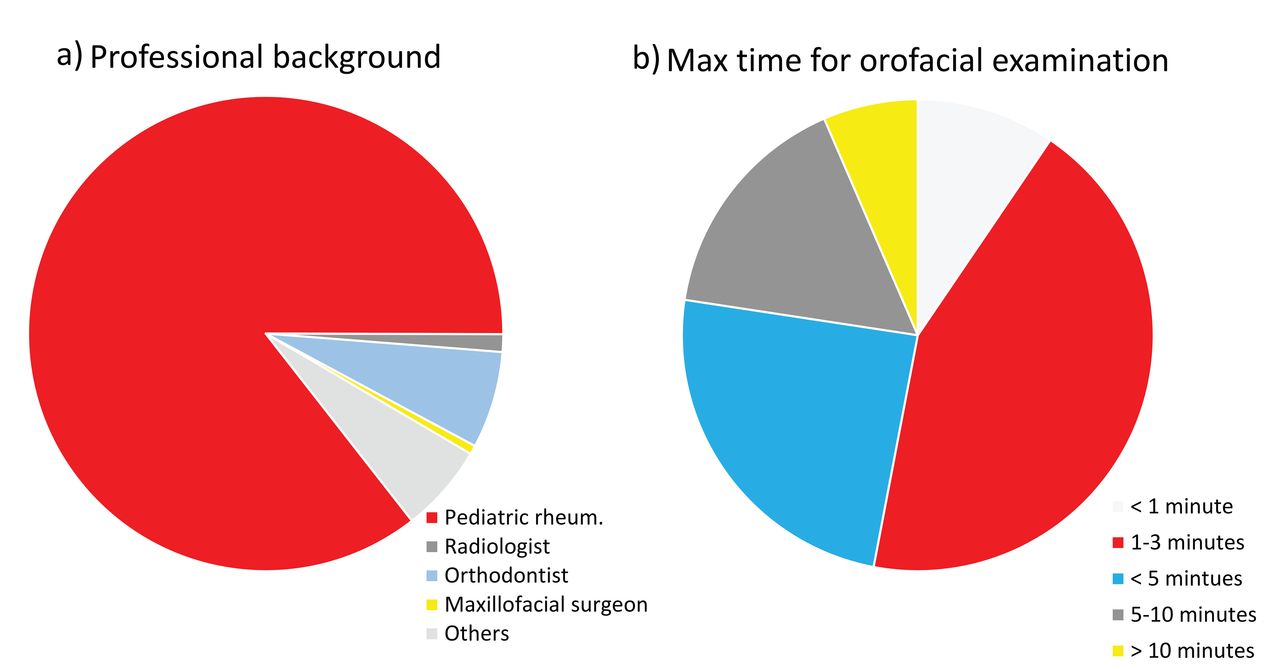
Conceptual phase and preliminary decision making: (a) Professional background of responders (n = 167) to online survey dealing with orofacial examination in JIA. (b) Response to the question: “What is the maximal time that can be devoted to clinical orofacial examination during a full-body examination of subjects with JIA?” JIA: juvenile idiopathic arthritis.
Item generation
The systematic literature review provided evidence to include 12 general items relevant for the clinical orofacial examination in patients with JIA19. The importance of each of the 12 examination items was assessed during a 3-round Delphi study by members on the TMJaw mailing list (n = 40). Each of the 12 proposed examination items was rated on a 10-point numerical scale (0 = not important, 10 = of utmost importance). Examination items were then subcategorized based on their ratings of importance: “high importance” (score ≥ 8), “moderate importance” (score ≥ 6 and < 8), “low importance” (score < 6)19. Based on the Delphi study results, the task force recommended 6 examination items for the short clinical examination protocol: (1) clinician-assessed pain location; (2) TMJ pain on palpation with open and closed mouth (unilateral, bilateral); (3) mandibular deviation at maximal mouth opening (≥ 3 mm deviation to the right or left side); (4) maximal unassisted mouth opening capacity measured in mm, with the vertical incisal overlap taken into account; (5) frontal facial symmetry (presence of asymmetry); and (6) facial profile (straight, mild convex, moderate convex, micrognathic). To ensure content validity, only items receiving a “high importance” Delphi survey categorization were included in the clinical examination protocol. Specific descriptions of outcomes for examination items are given in Table 1 and Figure 2.

Clinical examination items in the short screening protocol. (a) TMJ palpation with closed mouth. (b) TMJ palpation with open mouth. (c) Maximal mouth opening capacity. Please see Online Supplementary Material (available with the online version of this article) for instructions on how to account for the vertical incisal overlap. (d) Mandibular deviation at maximal mouth opening. “X” indicates the chin point. (e) Assessment of facial symmetry. (f) Assessment of facial profile (e.g., convexity). TMJ: temporomandibular joint.
Description of items included in the short clinical examination protocol.
Test of reliability
Twenty-two subjects with JIA were enrolled in this phase of the study. The mean age was 11.6 years (SD ± 2.5 yrs) and 55% were girls (n = 12). Acceptable intrarater and interrater κ values were calculated for all examination items ranging from 0.41 to 0.81 (Table 2). According to Landis and Koch, a κ statistic agreement is “moderate” between 0.41–0.60, “substantial” between 0.61–0.80, and “almost perfect” when > 0.8023. The average mean examination time across all 4 raters was 2 min and 42 s (SD ± 38.5 s, range 90–277 s).
Test of reliability.
Test of construct validity
Two groups with a total of 167 subjects were included in the test of construct validity: JIA group (n = 76, mean age 12.22 yrs, SD ± 3.0 yrs) and the control group (n = 91, mean age 13.45 yrs, SD ± 2.6 yrs). The control group was significantly older and included significantly more boys in comparison to the JIA group. Characteristics of included subjects are displayed in Table 3. The results of construct validity testing are displayed in Table 4:
H1 was accepted: A significantly larger proportion of JIA subjects (17%) reported orofacial pain within the last 2 weeks when compared to controls (7%).
H2 was accepted: JIA subjects had a significantly higher frequency of TMJ pain on palpation with open mouth (20% vs 7%) and mandibular deviation at maximal mouth opening (22% vs 4%). Additionally, maximal mouth opening was significantly reduced between JIA and control groups (difference: −3.17 mm, 95% CI −4.95 to −1.38 mm).
H3 was accepted: The JIA group displayed a significantly greater proportion of facial asymmetry (65% vs 34%) and presence of micrognathic profiles (7% vs 0%) when compared to controls.
Cohort characteristics for test of construct validity.
Test of construct validity. Intergroup proportional difference for examination items included in the clinical examination protocol.
Establishment of final recommendations
The results were presented to members of the task force and consensus of the final recommendations was created through e-mail correspondence. The clinical examination protocol and specific instructions for each item are found in the Online Supplementary Material (available with the online version of this article).
DISCUSSION
This project proposes a consensus-based, short, clinical examination protocol for routine use in clinical care and research settings in subjects with JIA. The screening protocol consists of 6 unique items, which encompass features of TMJ symptoms, TMJ dysfunction, and dentofacial deformity. Detailed instructions for each of the items have been developed to support clinical training and enhance reliability across healthcare providers (Online Supplementary Material, available with the online version of this article). The items show acceptable interrater reliability and construct validity, and represent some of the most consistently used outcome variables in the existing literature dealing with the orofacial examination in JIA19. Most included items originate from traditional orofacial examination methods such as the Helkimo index and the DC/TMD criteria17,18. However, unique to this project, we have identified a group of “traditional” items that are specifically relevant to JIA-related orofacial manifestations and combined those with additional items to assess dentofacial growth and development.
Identification of TMJ involvement in patients with JIA is the first step to appropriate management. The protocol can be completed in < 3 min. This meets the optimal time limit determined by the online questionnaire regarding the maximal amount of time the pediatric rheumatologist can devote to a dentofacial examination. The short completion time makes this protocol a valuable addition to the routine full-body assessment of patients with JIA. The standardized clinical examination provides a first-line, noninvasive, solid foundation for the dentofacial evaluation when conducted in combination with contemporary imaging and radiological examination standards24.
According to the recent consensus-based recommendations on TMJ arthritis-related terminology, TMJ arthritis is defined as active inflammation in the TMJ, whereas TMJ involvement is defined as abnormalities presumed to be the result of TMJ arthritis22. In general, the absence of orofacial symptoms is not a valid predictor for the absence of TMJ inflammation and vice versa7. Standardized TMJ MRI examinations were not available for participants in the JIA group. It is therefore unclear whether the orofacial symptoms and dysfunctions in the JIA group are due to active TMJ arthritis or TMJ involvement.
Across the literature, assessment of mouth opening capacity is the most frequently used clinical orofacial examination item in JIA7,19. In our study, the maximal mouth opening capacity in the JIA group was significantly reduced. Cross-sectional studies have shown a limited diagnostic sensitivity of reduced maximal mouth opening capacity of < 40 mm in subjects with TMJ arthritis1,9,16. Abramowicz, et al have reported that patients with a limited mouth opening capacity of 2 SD below age-related normative values were 6.7 times more likely to have TMJ arthritis14. Further, Abramowicz, et al have also demonstrated that limited mouth opening capacity in combination with mandibular deviation at maximal mouth opening was associated with a predictive value of 1.00 for the presence of MRI-verified TMJ synovitis14. More recent systematic reviews have shown that the presence of mandibular deviation at maximal mouth opening is one of the most sensitive predictors for the presence of TMJ inflammation in JIA7,19.
Assessment of mouth opening capacity is also the most frequently used outcome variable in TMJ arthritis followup studies. Changes in mouth opening capacity have been used as an indirect measure of TMJ functional status; post-interventional increase in opening capacity has been regarded as a sign of TMJ functional improvement. Commercial products exist to assist assessment of maximal mouth opening. In addition, methods such as the “3 finger assessment method,” and standardized cutoff values for assessment of mouth opening capacity have been proposed25,26. We recommend including the vertical incisal overlap when measuring maximal mouth opening capacity in JIA in relation to age-related normative values. This takes into account the substantial change of mouth opening capacity with growth and development, during transition between primary and permanent dentition27,28,29.
TMJ arthritis is a subcategory within the general term temporomandibular disorders (TMD)18. TMD diagnoses encompass both dysfunctional and autoimmune etiologies as well as pain conditions. The conditions vary from mild, temporary, non-symptomatic disc issues, to severe conditions such as TMJ degeneration, myalgia, and chronic orofacial pain conditions18. The reported prevalence of TMD is 10–16% in the non-JIA adolescent population, which is greater than the prevalence of 4–7% in the control group of the present study30,31. This substantial difference is explained by differences in methodology. In the current protocol, we decided to exclude assessment of TMJ noise (clicking and crepitation) because of low diagnostic sensitivity for TMJ arthritis in JIA1. A metaanalysis performed by Da Silva, et al demonstrated that the most prevalent clinical finding of TMD in the non-JIA population was asymptomatic TMJ noises30.
It is noteworthy that the symptoms and clinical findings of arthritis-induced dysfunction are comparable to those encountered in other TMD18,30. Differential TMD should be considered in patients with JIA who present orofacial dysfunction or dentofacial deformities during the clinical examination. Such findings may not exclusively be caused by active TMJ arthritis from JIA; dentofacial asymmetry was found in 34% of the control group in our present study. This is consistent with research by Liukkonen, et al, who reported dentofacial asymmetry to be a common clinical finding in the background population32.
A standardized orofacial examination will provide complex information about dentofacial function, growth, and development. Regardless of etiology, abnormal clinical findings are a red flag, and should prompt increased attention during followup visits, and referral for appropriate imaging when indicated. Followup imaging should be guided by recent consensus-based protocols for TMJ MRI15,33 and 3-D assessment of TMJ deformity and dentofacial deformities in JIA10,15. The various TMJ imaging techniques come with their own benefits, drawbacks, and limitations34.
Attention to dentofacial growth and development is an important examination item to help detect dentofacial deformities. Economou, et al demonstrated a significant correlation between dentofacial hard-tissue and soft-tissue asymmetries in JIA where even minor mandibular asymmetries were detected by visual inspection during the clinical examination35. Findings by Ikavalko, et al also support the valid use of profile assessment to identify subjects with micrognathic mandibles36. This study demonstrates that moderate dentofacial convexity may be found in JIA as well as in the background population. In contrast, micrognathia was only identified in JIA. Management of arthritis-induced dentofacial deformity can be guided by recent recommendations37.
Longitudinal, interventional studies have documented a poor association between the fluctuation of orofacial symptoms/dysfunction and post-interventional MRI findings38,39,40. From a clinical standpoint, this highlights the important contribution of both clinical and MRI examinations and underlines the relevance of both modalities in the dentofacial health assessment in JIA. Previous research has focused on the ability to predict the presence of TMJ inflammation based on items from the clinical examination. Less attention has been devoted to studying the implications of dentofacial signs and symptoms on longterm outcomes regardless of TMJ status. Recent data from a Danish cohort study revealed that 56% of the cohort presented with at least 1 clinical sign of dentofacial dysfunction and 35% were diagnosed with an arthritis-induced dentofacial deformity within the first 5 years after JIA diagnosis41. These findings underscore the importance of routine, standardized orofacial examination in patients with JIA.
There are certain limitations to our study that warrant further consideration. Not all of the proposed examination items reached above a “moderate” agreement level (r = 0.41–0.60) during assessment of intrarater and interrater reliability. Although this protocol consists of the outcome variables with the widest used for assessment of TMJ arthritis in interventional studies19, its ability to detect changes in orofacial dysfunction (responsiveness) still needs to be evaluated in future studies. There was a significant difference in age and sex between the JIA group and the control group in the construct validity test: intergroup differences in age and sex are potential sources of biases to the test of construct validity because general TMD is most often found in pubertal girls30,31. Also, the absence of routine MRI examination for assessment of TMJ arthritis/involvement in all JIA group subjects is considered a limitation to our study.
There are significant strengths in our study. The protocol was meticulously developed by using an established sequential-phased approach in an interdisciplinary setting. In phase 1, the global online questionnaire strengthened the clinical usability of the proposed examination protocol. Because treatment of TMJ arthritis involves an interdisciplinary approach, a primary goal of our recommendations was to create a protocol that can be used by healthcare providers without specialized training in the TMJ and dentofacial examination. Another strength is the detailed instructions provided with each item in the Online Supplementary Material (available with the online version of this article). An important future focus is to produce educational video material to ensure reliability and validity among healthcare providers who are less experienced with orofacial examination.
We have developed a consensus-based short clinical examination protocol showing acceptable construct validity and test-retest reliability. This protocol takes < 3 min to complete and will generate essential information about TMJ symptoms, TMJ dysfunction, and dentofacial deformity. It is our hope that this screening protocol will be integrated into standard clinical care and will be incorporated in future research studies.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
We thank Willemeijn vanBryggen, Michel Steenks, Lukas Muller, Nikolay Tzaribachev, Malene Leddet, and Annelise Küseler for their contributions to this project. We thank Carina Carels for her help with the illustration of facial profiles in the Online Supplementary Material (available with the online version of this article).
- Accepted for publication November 13, 2019.








{kind=link}
{kind=link}