

Abstract
Objective. To examine the reproductive pattern of women with idiopathic inflammatory myopathy (IIM) compared to the general population.
Methods. Population-based, nationwide registers were used to identify offspring of women with IIM and comparators.
Results. Women with IIM in general had similar reproductive patterns as the comparators, whereas in those diagnosed between 26 and 45 years of age, there was an overall trend for fewer children as well as a higher proportion of nulliparity and a lower fertility rate in women with dermatomyositis than their comparators.
Conclusion. Reproductive attention should be paid to patients with IIM diagnosed during the childbearing period.
There is an increased interest in the reproductive health of patients with rheumatic diseases1. The potential reproductive health issues include reduced sexual libido, sexual disability, subfertility/infertility, low fecundity, and reduced family size1. Though the research attention has particularly been focused on patients with rheumatoid arthritis and systemic lupus erythematosus1, a few studies suggest that women of childbearing age with idiopathic inflammatory myopathy (IIM) have reduced ovarian reserve2,3, decreased fertility rate4, and increased need of assisted reproductive therapy5. Two qualitative studies have also found that patients with IIM have problems with sexual dysfunction6,7. To our knowledge, there are no studies investigating the reproductive pattern in women with IIM using population-based methods. We therefore aim to study the proportion of nulliparity, age at first delivery, fertility rate, and interdelivery interval in women with IIM and women from the general population.
MATERIALS AND METHODS
Registers
The Swedish National Patient Register (NPR) has collected nationwide data on inpatient care since 1987 and holds data on all outpatient visits in nonprimary care since 2001. The overall validity of diagnosis in the NPR ranges from 85% to 95%8. The Swedish Multigeneration Register (MGR) was established in 1947 and has parental and offspring information on all individuals born in Sweden since 1932. The coverage of data on offspring is nearly 100%9.
Study subjects
In this population-based study, we included all women born in 1932 and onward who had a first registration indicating IIM between 2001–2016 and at least 1 followup visit within 1–12 months after the first IIM visit in the NPR. This algorithm has been validated with a positive predictive value up to 94% and a sensitivity up to 96%10. Between 1998 and 2000, we had data only on inpatient care; therefore, individuals who were discharged with a diagnosis of IIM from inpatient care during that period were also included. International Classification of Diseases, 10th revision (ICD-10) codes used were M33.0, M33.1, M33.2, and M33.9, and only ICD-10 codes registered from the internal medicine, rheumatology, dermatology, neurology, or pediatrics clinics were considered. IIM was further categorized into juvenile IIM (M33.0), dermatomyositis (DM; M33.1), and other IIM (M33.2 and M33.9). Polymyositis (PM) was studied with other types of IIM, because its code (M33.2) is often used for inclusion body myositis. Whenever a patient with IIM was diagnosed, up to 5 women without IIM, alive and living in Sweden when the case met our inclusion criteria, were randomly selected from the Total Population Register (TPR) and were matched to the IIM patient on birth year and residential area.
Outcomes and other variables
Data linkage to the MGR through the unique identification number enabled us to identify offspring of the study subjects. Nulliparity was defined as not having any registered children, age at first delivery was the mother’s age at the birth of the first registered child, the fertility rate was defined as the number of children per woman, and interdelivery interval was defined as the average time period from a prior birth to a subsequent birth. Maternal country of birth was identified using the TPR.
Statistical analyses
Characteristics and outcomes in women with IIM were stratified by age at IIM diagnosis (≤ 25, 26–45, and > 45 yrs) and analyzed versus the comparators without IIM, overall and by IIM subtypes. Results were presented using means with SD and medians with interquartile ranges (IQR) for continuous variables, and frequencies with proportions for categorical variables. Mann-Whitney U test or chi-square test with 0.05 α-level of significance was used.
Additional analyses were performed including only women born between 1932 and 1972 whose entire reproductive period (15–45 yrs old) was covered. Because most women diagnosed with IIM ≤ 25 years of age were born after 1972, the analyses were stratified into either ≤ 45 or > 45 years of age at the time of IIM diagnosis. We used the SAS version 9.4 package for all statistical analyses (SAS Institute Inc.). The regional ethics board approval number was 2017/2000-31. Patient consent was waived because this is a register-based study.
RESULTS
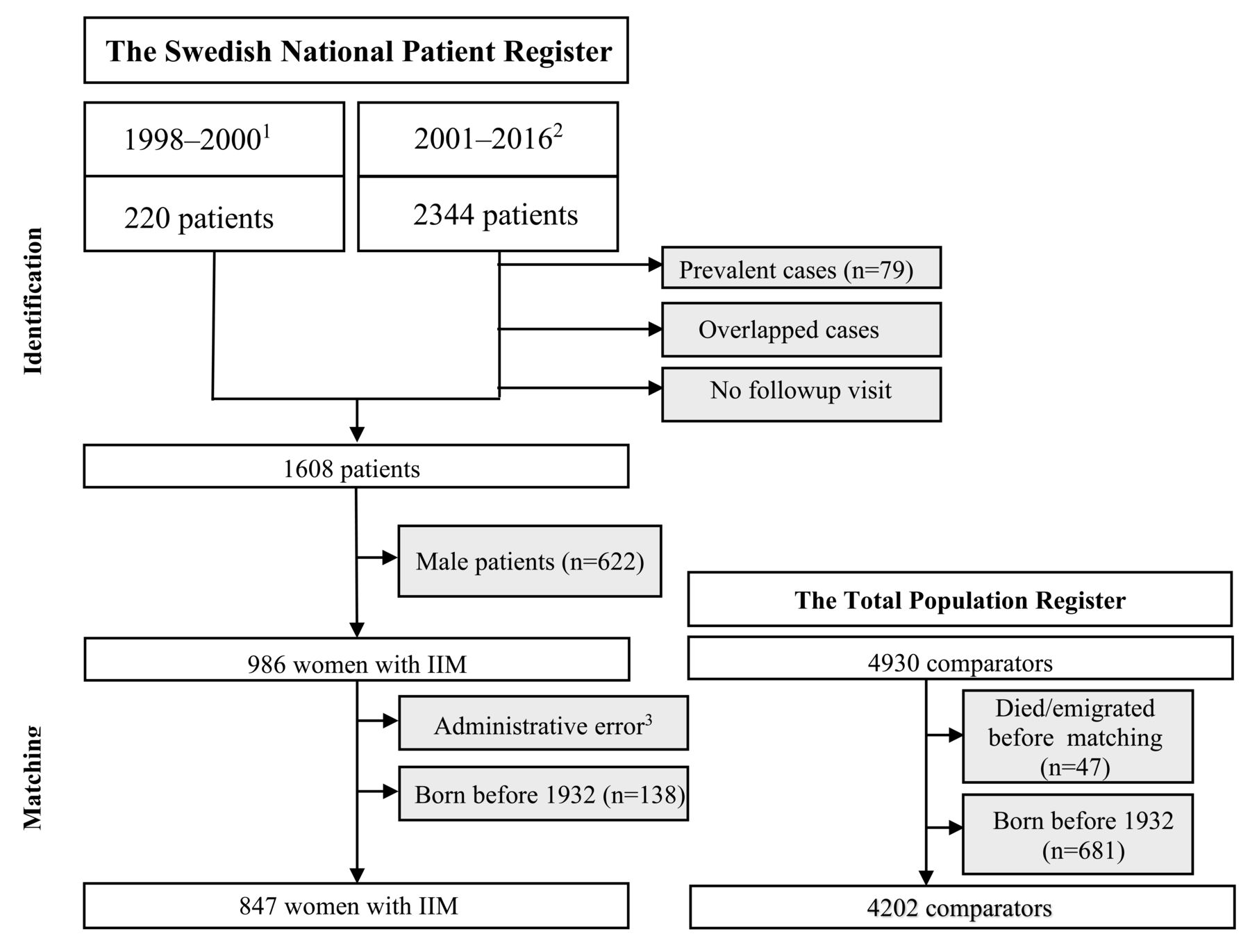
We included 847 women with IIM and 4202 comparators (Figure 1), most of them born in Nordic countries. Among 847 women with IIM, 236 (27.86%) were diagnosed with IIM at ≤ 45 years of age (Table 1).
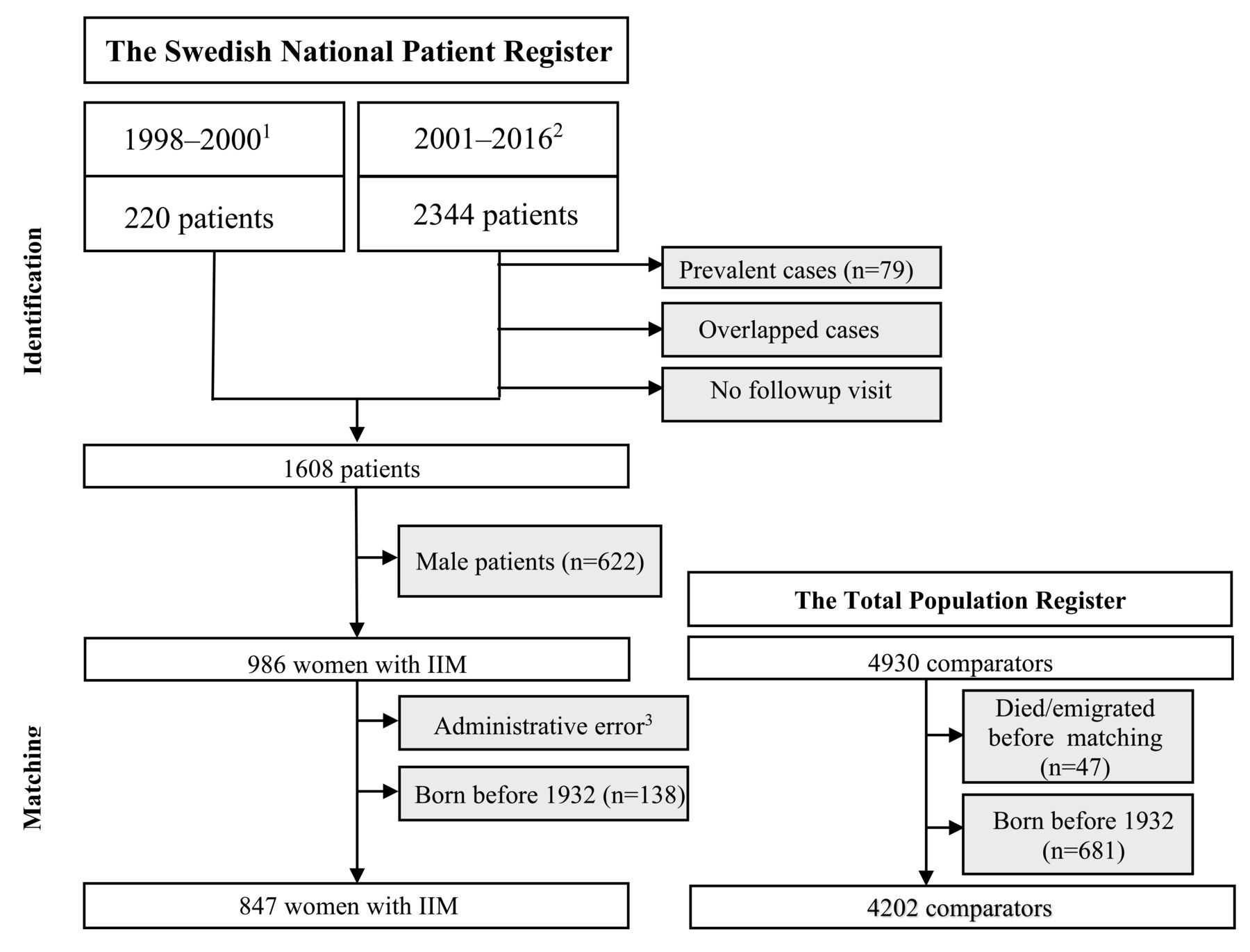
The flow chart of the study population. 1 A hospitalization indicating incident IIM.2 Diagnosis of incident IIM with at least 1 followup visit within 1–12 months after the first IIM indication. 3 Potential case of administrative error as this patient had record of followup visit during emigration time. However, the 5 comparators matched to this patient were kept. IIM: idiopathic inflammatory myopathy.
The characteristics of women with IIM (n = 847) and comparators without IIM (n = 4202) by age at IIM diagnosis.
Overall, the proportion of nulliparity, age at first delivery, fertility rate, and interdelivery interval among women with IIM did not significantly differ from the comparators (Table 2). However, women with IIM diagnosed between 26 and 45 years of age had a lower fertility rate than the comparators [medians with IQR: 2 (1–2) vs 2 (1–3), p = 0.08; means with SD: 1.66 ± 1.11 vs 1.86 ± 1.25]. In the same age group, women with DM had a fertility rate [median (IQR)/mean (SD)] of 2 (0–2)/1.49 (1.16) children/woman and 26.39% of them were nulliparous, versus 2 (1–2)/1.75 (1.19) children/woman (p = 0.09) and 19.50% (p = 0.19) in the comparators, respectively. Moreover, women with juvenile IIM and women with IIM diagnosed between 26 and 45 years of age were younger at first delivery than their comparators [medians with IQR: 23 (19–25) vs 25 (20–26), p = 0.07, and means with SD: 22 ± 3 vs 25 ± 3; and medians with IQR: 26 (22–29) vs 27 (23–31), p = 0.04, and means with SD: 26 ± 5 vs 27 ± 5, respectively; Table 2]. Consistent results were found in the additional analyses (Supplementary Tables 1 and 2, available from the authors on request).
The reproductive pattern of women with IIM (n = 847) compared to the comparators without IIM (n = 4202) by age at IIM diagnosis.
DISCUSSION
We could not detect any differences in nulliparity, age at first delivery, fertility rate, and interdelivery interval in women with IIM compared to the comparators. A case review reported 12% of nulliparity among 78 patients with DM/PM and found no difference from the general population though indirect comparison with data from previously published literature11. In that case review, women with DM were analyzed together with all others with IIM. This could explain the apparent discrepancy between the results in the case review and our study, given that only women with DM diagnosed in mid- to late reproductive age were more likely than the comparators to be childless in our study. We also observed a tendency of reduced fertility in women with DM diagnosed between 26 and 45 years of age. A Mexican study interviewing patients with DM/PM found a fertility rate of 4.5 children/woman among 17 patients having children before diagnosis and a fertility rate of 1.7 children/woman in 7 patients delivering after diagnosis; however, the differences in study design make it difficult to compare their results to our findings4. Somewhat unanticipated findings of our study were that patients with juvenile IIM and women with IIM diagnosed in mid-to late reproductive age entered motherhood earlier than the comparators, which contrasts to the ovarian dysfunction among patients with juvenile IIM seen in a Spanish study12 and the observed low level of anti-Müllerian hormone and low astral follicle count in patients with DM and PM2,3. This inconsistency may mean that the improved treatment regimens in IIM, resulting in lower accumulated doses of corticosteroids, may lessen the effect on reproduction1,13.
There are many factors related to reproduction that could have an effect on fertility in women with IIM. Rider, et al reported that 3 to 5% of adult patients with IIM had sexual dysfunction, infertility, and irregular menses14. A Swedish qualitative study of patients with DM/PM identified sexual disability as one of the most common disabilities reported besides traditional IIM symptoms7. The suggested factors associated with affected sexuality in IIM were muscle weakness and pain6, use of cyclophosphamide or high-dose corticosteroids1,6, and medical advice against pregnancy during active disease status1. It could also be that patients with IIM are as likely as any woman to conceive but are involuntarily nulliparous or have reduced family size owing to frequent miscarriages15. This would be in line with our findings that DM patients diagnosed during the childbearing period had tendencies of nulliparity and lower fertility rate.
Being limited to register data, we lacked information on individuals’ views on childbearing, occurrence of miscarriage, use of contraception, disease activity, autoantibody profile, and medication. This precluded us from further analysis and comprehensive interpretation of our study. However, data ascertained from the NPR and the MGR had long followup and high quality8,10, allowing inclusion of a large representative sample of women with IIM and ensuring high ascertainment of data on offspring. Matching women with IIM to the comparators by birth year also helped to minimize the bias of cohort differences in childbearing. Inclusion of women still of reproductive age might not reflect the absolute fertility rate. However, additional analyses limited to women whose entire reproductive period was covered demonstrated similar results.
We observed that the reproductive pattern in women with IIM was, overall, reassuring versus the comparators without IIM. But patients with DM diagnosed in the mid- to late reproductive period showed tendencies of nulliparity and reduced fertility, directing further attention to reproductive health among patients with IIM diagnosed during childbearing years.
Footnotes
This work was supported by the Nanna Svartz Foundation, the Swedish Rheumatism Association, by grants provided by the Stockholm County Council (ALF project), and the Gustaf V 80-year Foundation.
- Accepted for publication August 2, 2019.








{kind=link}