

Abstract
Objective. To investigate whether trabecular bone loss is longitudinally associated with disease activity measures in patientswith axial spondyloarthritis (axSpA).
Methods. Data from patients enrolled in the Incheon Saint Mary’s axSpA prospective observational cohort were evaluated. Trabecular bone loss was assessed using the trabecular bone score (TBS). The relationship between TBS and disease activity measures [Ankylosing Spondylitis Disease Activity Score (ASDAS), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP)] was investigated using generalized estimating equation (GEE) models.
Results. Four-year followup data from 240 patients (80% males, mean age 37 ± 12 yrs) were evaluated. At baseline, higher disease activity according to ASDAS-ESR and ASDAS-CRP showed a trend toward lower TBS (p = 0.003 and p = 0.016, respectively). Univariate GEE analyses showed a significant association between TBS and disease activity measures over time, with the exception of BASDAI. Univariate analysis showed a longitudinal association between TBS and age, smoking, and spinal structural damage. In multivariate GEE analysis, ASDAS-ESR, ASDAS-CRP, ESR, and CRP were longitudinally associated with TBS after adjustment for confounding factors. ASDAS scores and inflammatory markers were longitudinally associated with TBS in patients with ankylosing spondylitis (AS; 79%), but not in patients with nonradiographic axSpA (nr-axSpA). BASDAI scores showed no relationship with TBS in either the AS or nr-axSpA groups.
Conclusion. Trabecular bone loss in patients with axSpA, assessed using the TBS, showed a longitudinal association with ASDAS scores and inflammatory markers.
Axial spondyloarthritis (axSpA) is associated with inflammation of the sacroiliac joints and spine, with erosions, syndesmophytes, and ankylosis developing in patients with more advanced disease. AxSpA includes nonradiographic axSpA (nr-axSpA), which is characterized by the absence of sacroiliitis on conventional radiographs, and radiographic axSpA, which is also referred to as ankylosing spondylitis (AS) and is characterized by sacroiliitis on radiographs1. The chronic inflammation associated with axSpA leads to a wide range of bone changes, particularly remodeling. Abnormal bone metabolism results in pathological new bone formation in the cortical zone of the vertebrae and the loss of trabecular bone from the vertebral bodies, leading to low bone density2.
The mechanism of new bone formation in axSpA has not been fully established. One hypothesis is that inflammation is the first stage, followed by a repair mechanism that replaces the subchondral bone marrow with fibrotic/granulation tissue and stimulates new bone formation3. The relative inaccessibility of the spine and the lack of established biomarkers related to bone homeostasis have limited study of the pathophysiology of axSpA4. To date, studies of the association between new bone formation and inflammation in axSpA have been performed using techniques such as magnetic resonance imaging (MRI)5,6. However, a substantial number of syndesmophytes are not preceded by lesions that are detected by MRI, such as osteitis or fatty lesions5. Thus the relationship between inflammation and activation of these pathways remains the subject of some debate. Recently, another hypothesis for the mechanism of new bone formation in axSpA has been proposed, i.e., that initial inflammation leads to inflammation-induced bone loss and therefore instability, another type of biomechanical stress. Reactive attempts to increase spinal stability could therefore occur at sites away from the inflammation7.
Cortical and trabecular compartments appear to have different reactions to inflammation; in SpA, the bone tissue directly exposed to inflammation (osteitis) is the trabecular bone of the vertebrae, but not the cortical bone surface8. Inflammation-related trabecular bone loss can lead to micro-structural changes, which affect the mechanical properties of the spine and can lead to spinal instability. Persistent inflammation may prevent an anabolic response from correcting any instability in the trabecular bone of the vertebral bodies, and relatively new bone formation in the cortical bone of the vertebrae may be increased7. However, to date, there have been no longitudinal studies of the association between inflammation and trabecular bone changes in patients with axSpA, as there are no tools that reliably reflect microstructural change in the vertebrae.
The trabecular bone score (TBS) has been introduced as a noninvasive method of estimating trabecular microarchitecture. The TBS is a texture index derived from standard lumbar spine dual-energy absorptiometry (DXA) images and has been shown to be related to bone microarchitecture and fracture risk9. Evaluation of TBS has been proposed as a surrogate marker for vertebral body microarchitecture10. In addition, a recent cross-sectional study showed that TBS values were lower in patients with axSpA than in matched controls. Also, a negative correlation was seen between TBS and systemic inflammatory markers11. However, the association between TBS and inflammation has not yet been addressed in longitudinal studies of axSpA. We evaluated the association between TBS values and clinical disease activity measures in patients with axSpA, and investigated whether TBS values are related to disease activity measures over time.
MATERIALS AND METHODS
All patients that visited the rheumatology outpatient clinic of Incheon Saint Mary’s Hospital since January 2014 (enrollment is ongoing), resided in a defined geographical area of Incheon, and fulfilled the Assessment of SpondyloArthritis international Society (ASAS) criteria12 were included in this prospective observational cohort study [Incheon Saint Mary’s AXial SPondyloArthritis study (ISAXSPA)]. The ISAXSPA focused on identifying predictors for new bone formation in the spine and bone loss, including osteoporosis and vertebral fracture, in patients with axSpA. Patients recruited into this cohort were required to fulfill the imaging arm of the ASAS axSpA criteria12, including patients with established AS13.
Patients were recruited in academic outpatient facilities, irrespective of the treatment they had received. Patients were evaluated annually according to a standardized protocol that included clinical and laboratory variables. Imaging variables included radiographs of the cervical, thoracic, and lumbar spine, and DXA assessment at baseline and annually for all patients. Patient questionnaire data (including information regarding classification, comorbidity, disease activity, and physical function) were evaluated annually.
TBS data from patients enrolled in the ISAXSPA cohort were assessed. Enrollment in the ISAXSPA study started in January 2014 and is continuing. The present study represents an interim analysis of the first 240 patients. Patients with DXA images and disease activity measures available for at least 2 consecutive visits were included in the analysis. Those with and without followup DXA data were evaluated to identify selection bias according to baseline characteristics and radiographic progression.
The study was performed in accord with the Helsinki Declaration. Written informed consent was obtained from all participants prior to inclusion into the observational cohort, and the study protocol was approved by the ethics committee of Incheon Saint Mary’s Hospital (study no. OC16OISI0138).
Clinical data
Disease-related data and disease activity measures were collected annually. Clinical data included the time after symptom onset, presence of HLA-B27, smoking status (never, ex-smoker, current), and use of medications such as antiinflammatory drugs, sulfasalazine, and tumor necrosis factor inhibitors. Patients included in the study were not treated with glucocorticoids during the study period. The Bath Ankylosing Spondylitis Functional Index (BASFI)14 and measures of disease activity using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)15 were collected and patient’s global assessment scores were also recorded. All scores were measured on a visual analog scale (0–10). The Ankylosing Spondylitis Disease Activity Score (ASDAS) was calculated as described16. Disease activity state was defined as one of 4 groups according to the ASDAS17. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were also measured.
DXA assessment
Bone mineral density (BMD) at the lumbar spine and left hip was assessed using DXA (Lunar Prodigy densitometer, GE Healthcare). All measurements were taken by experienced operators using the same machine and standardized procedures with respect to participant positioning. BMD was measured at the lumbar spine using an anteroposterior projection at L1–L4 and at the left hip from the femoral neck and total proximal femur. BMD was expressed as number of grams of bone mineral per square centimeter (g/cm2).
TBS assessment
TBS was calculated from DXA images of the lumbar spine (L1–L4). Lumbar spine DXA images were reanalyzed in an operator-independent automated manner using TBS iNight software version 2.1 (Med-Imaps). The software uses posterior-anterior images, including the BMD region of interest and edge detection; thus, the TBS is calculated over exactly the same region as the lumbar BMD. Patients were divided into 3 TBS groups according to the risk of fracture, as identified in a recent meta-analysis18: high risk (TBS < 1.23); intermediate risk (TBS 1.23–1.31); and low risk (TBS < 1.31). Low TBS was defined as ≤ 1.31. Reproducibility of the TBS (based on the coefficient of variation) was assessed using replicate scans. Average short-term reproducibility was 1.04%.
Radiographic scoring
The presence of radiographic sacroiliitis at baseline was assessed by viewing images of the sacroiliac joint according to the New York criteria13. The reader was blinded to the patients’ clinical characteristics.
For all patients, radiographs of the cervical, thoracic, and lumbar spine were obtained at baseline and every year thereafter. Lateral views of the cervical and lumbar spine were scored according to the modified Stoke AS Spinal Score (mSASSS)19. Total scores ranged from 0 to 72. The number of syndesmophytes was assessed using the mSASSS. The mSASSS data were scored by a single trained expert who was blinded to patient characteristics.
Statistical analysis
Continuous data were expressed as mean ± SD, and categorical data as percentages. Clinical variables were compared using an independent t test, and the chi-square test was used to compare categorical variables between axSpA patients with and without followup DXA data. The proportion of TBS subgroups by fracture risk was compared across ASDAS groups using chi-square tests. Spearman correlation coefficient was used to analyze correlations between variables.
The longitudinal relationships between TBS values and disease activity measures were analyzed using generalized estimating equation (GEE) models, with TBS value as a dependent variable and the separate clinical measures as independent variables. GEE is a technique for longitudinal analysis that makes use of all available longitudinal data, allows unequal numbers of repeated measurements, and has some robustness against deviation from normality20. Variables with a p value ≤ 0.10 using univariate GEE were included in multivariable GEE models. Five separate models were built for TBS, and each one included one of the disease activity measures. All models were adjusted for age, HLA-B27, smoking status, radiographic sacroiliitis, and number of syndesmophytes. Model fit was estimated with the quasi-likelihood under the independence model criterion (QIC): the lower the QIC, the better the data fit the model. P-values ≤ 0.05 were considered to be statistically significant. Statistical analyses were performed using SPSS (v. 21.0; IBM Corp.).
RESULTS
A total of 330 patients were enrolled in the ISAXSPA cohort; of these, 240 patients had available baseline and followup DXA data and were included in the analysis. Four-year followup data were analyzed. All patients were aged 20–67 years. No significant differences were seen between the baseline data of the patients included in the analysis and those of all enrolled patients (Table 1). In the 240 patients included in the analysis, 193 (80%) were male. Four patients among 47 women were postmenopausal. Nine patients (4%) had psoriasis and 2 (1%) had inflammatory bowel disease. One hundred ninety (79%) patients fulfilled the modified New York criteria for classification of AS13.
Characteristics of patients with axial spondyloarthritis.
Mean ASDAS-ESR and ASDAS-CRP were 2.7 ± 1.1 and 2.4 ± 1.3, respectively, and 97 patients (41%) had syndesmophytes at baseline. The mean TBS value was 1.385 ± 0.123.
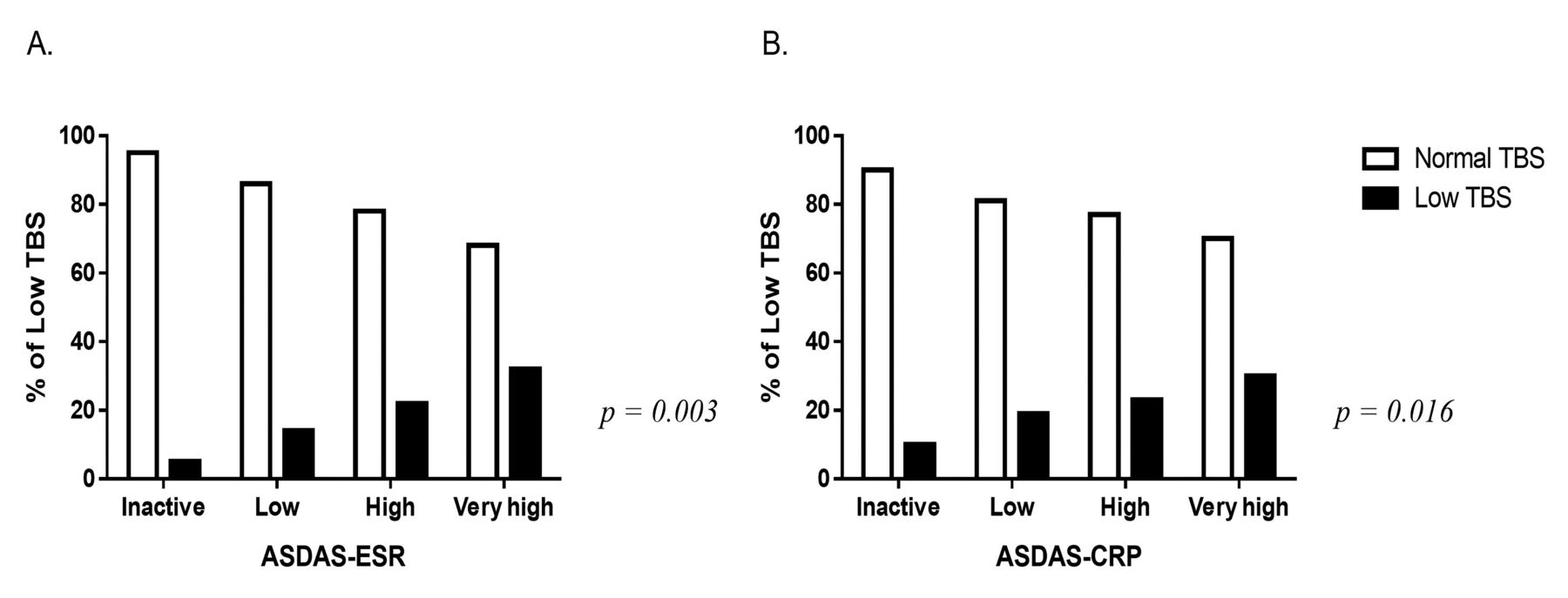
Figure 1 shows the proportion of patients with low TBS (≤ 1.31) according to disease activity at baseline. The proportion with a low TBS score was 7%, 17%, 18%, and 32% in the inactive, low, high, and very high ASDAS-ESR activity groups, respectively (p = 0.003). In the ASDAS-CRP activity groups, higher disease activity also showed a trend toward lower TBS (p = 0.016).

Proportion of patients with low trabecular bone score (TBS) values according to disease activity at baseline. A. Proportion of low TBS according to ASDAS-ESR activity group (p = 0.003). B. Proportion of low TBS according to ASDAS-CRP activity group (p = 0.016). ASDAS-ESR: Ankylosing Spondylitis Disease Activity Score based on erythrocyte sedimentation rate; ASDAS-CRP: ASDAS based on C-reactive protein.
Table 2 shows the correlation between disease activity measures, mSASSS, number of syndesmophytes, and TBS at each timepoint. Significant negative correlations were seen between TBS and ESR, CRP, mSASSS, and syndesmophyte number at baseline. ASDAS-ESR was negatively correlated with TBS at 1 year and 2 years, and ASDAS-CRP was negatively correlated at 2 years only; mSASSS and syndesmophyte number showed significant negative correlations with TBS at all times. ESR was negatively correlated with TBS at baseline and at 1 and 2 years’ followup. CRP data showed a negative correlation at baseline and 2-year followup. BMD at the lumbar spine also showed a negative correlation with disease activity measures at baseline, but at followup timepoints, ESR was negatively correlated with BMD only at 2 years. In contrast with TBS, BMD at the lumbar spine was positively correlated with mSASSS and syndesmophyte number at all followup times. The proportion of nr-axSpA at 1, 2, 3, and 4 years was 16%, 28%, 23%, and 11%, respectively.
Correlations between trabecular bone score (TBS) and bone mineral density (BMD) and disease activity scores and spinal structural damage.
Univariate GEE analyses showed that statistically significant associations for all disease activity measures were longitudinally associated with TBS, with the exception of BASDAI (Table 3). Age, smoking, radiographic sacroiliitis, and spinal structural damage were also longitudinally associated with TBS in the univariate analysis. Five separate models were built for the multivariate GEE analyses, each including the disease activity measures (Table 4). All models were adjusted for age, HLA-B27, smoking status, presence of radiographic sacroiliitis, and syndesmophyte number. With the exception of BASDAI, we observed a significant relationship between all disease activity measures and TBS, with the lower QIC values seen in the models with ESR.
Univariate generalized estimating equations for trabecular bone score.
Longitudinal relationship between disease activity measures and trabecular bone score.
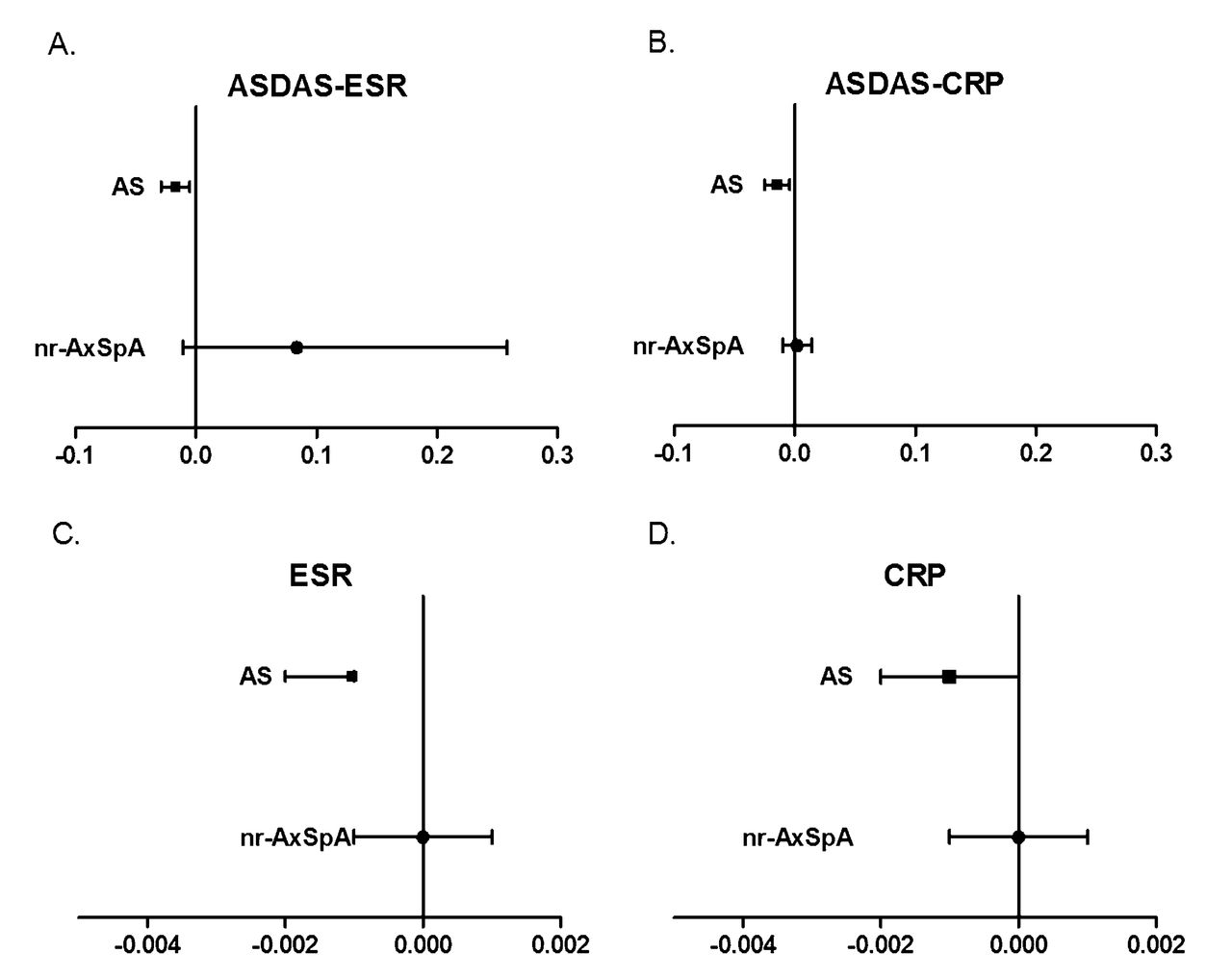
In patients fulfilling the AS criteria, ASDAS-ESR, ASDAS-CRP, ESR, and CRP were longitudinally associated with TBS. TBS values decreased by 0.001 and 0.015 per 1-unit increase in the ASDAS-ESR and ASDAS-CRP (β −0.001, 95% CI −0.029, −0.005 and −0.015, 95% CI −0.025, −0.004), respectively. Also, for each 1-unit increase in ESR and CRP, the TBS values decreased by 0.001 (β −0.001, 95% CI −0.002, −0.001 and −0.001, 95% CI −0.002, 0.000, respectively); however, none of the clinical measures were significantly related to TBS in patients with nr-axSpA (Figure 2). BASDAI showed no relationship with TBS in either AS or nr-axSpA patients.
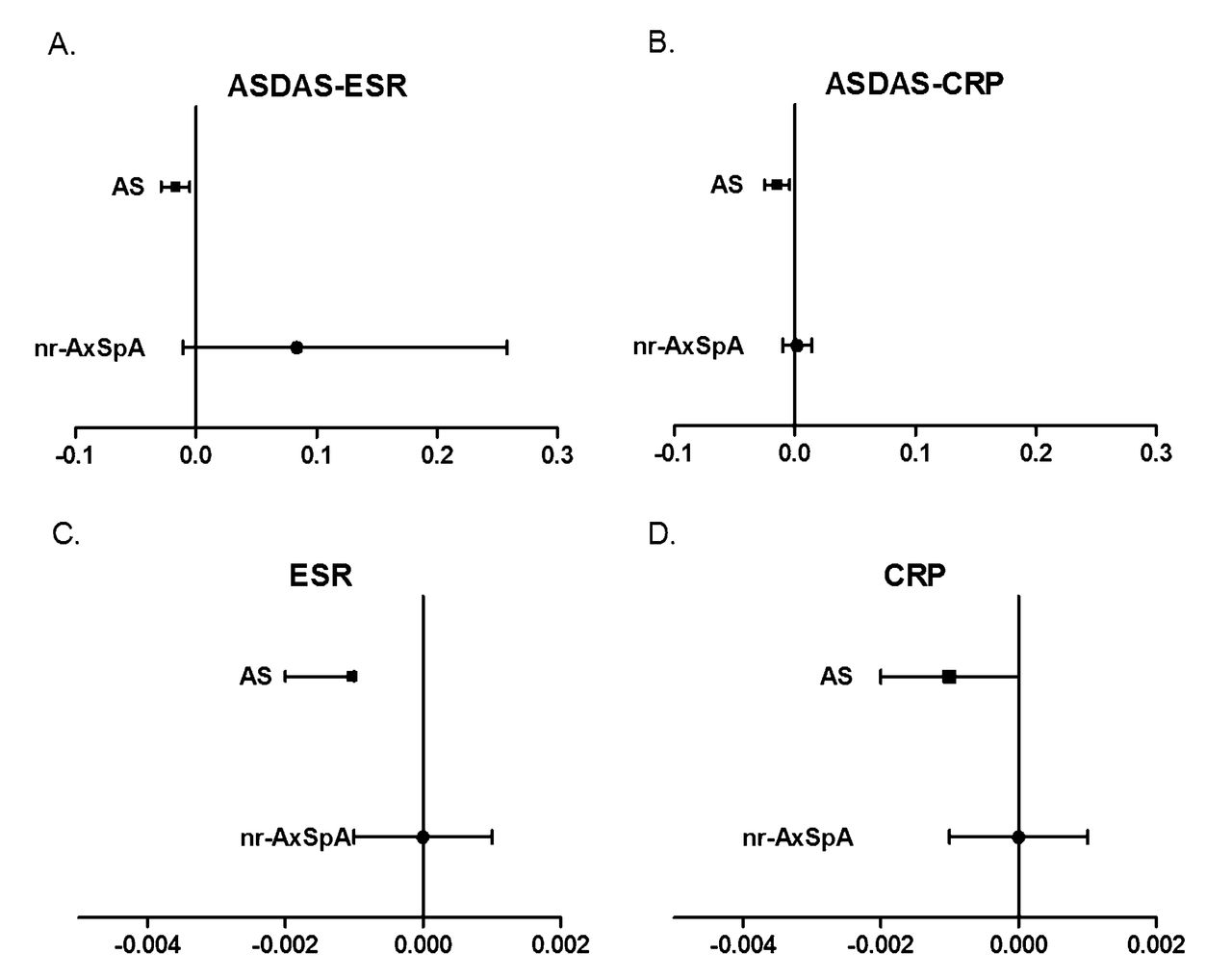
The longitudinal effect of disease activity measures on trabecular bone score (TBS) according to the presence of radiographic sacroiliitis. A. Longitudinal effect of ASDAS-ESR on TBS. B. Longitudinal effect of ASDAS-CRP on TBS. C. Longitudinal effect of ESR on TBS. D. Longitudinal effect of CRP on TBS. All models were adjusted for age, HLA-B27, smoking status, and syndesmophyte number. ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; ASDAS: Ankylosing Spondylitis Disease Activity Score; nr-axSpa: nonradiographic axial spondyloarthritis.
DISCUSSION
This study shows that disease activity measures are longitudinally associated with TBS values. ASDAS and systemic inflammatory markers (but not BASDAI) showed a significant association with TBS, and this association was seen to be specific to patients with AS.
We assessed trabecular bone loss using the TBS, which is a novel texture index derived from standard lumbar spinal DXA images. The TBS was developed as a clinical tool capable of assessing bone microarchitecture, which is a key determinant of bone strength9. Lower TBS values are known to be associated with an increased risk of major osteo porotic fracture, independent of BMD values21. Although it is not a direct measurement of bone microarchitecture, it provides information on trabecular characteristics that is not captured by the measurement of bone density. An ex vivo study has shown TBS to have a strong positive correlation with the number of trabeculae and the trabecular bone volume assessed on microcomputed tomography of transiliac bone biopsies22. Thus, the TBS is considered to be a practical and noninvasive tool for assessment of trabecular bone microarchitecture.
While the association between TBS and disease activity has previously been described in cross-sectional studies, our study is the first to reveal a statistically significant association in a longitudinal followup of patients with axSpA. In one recent cross-sectional study, TBS showed a negative correlation with ESR and CRP levels in patients with axSpA, but not in matched controls, and inflammatory markers were independently related to low TBS values in multivariate analysis11. In addition, Boussoualim, et al reported that TBS was associated with disease activity measured by ASDAS and ESR and CRP23. These data suggest that lower levels of TBS are related to disease activity, although these results are limited by the cross-sectional design. These previous studies and the current data support the use of TBS to reflect inflammation-mediated changes in lumbar spine trabecular bone in patients with axSpA.
Unlike the ASDAS, BASDAI values were not significantly associated with TBS in our study. This may reflect that the BASDAI is fully patient-reported and therefore reports patient-specific factors independent of inflammation. By contrast, the ASDAS is a better indicator of inflammation and has been shown to be associated with disease activity and inflammation on MRI24.
Subgroup analysis according to the presence of radiographic sacroiliitis showed that the longitudinal relationship between disease activity measures and TBS was present only in patients with AS. The fact that no association was seen in the nr-axSpA group may be explained by the lower level of spinal structural damage in these patients, compared with the AS group. The mean mSASSS was higher in the AS group than in the nr-axSpA group (15.5 ± 21.2 in AS and 1.1 ± 4.5 in nr-axSpA), meaning that the spinal involvement of inflammation was cumulatively greater in patients with AS than in those with nr-axSpA. Also, TBS showed a negative correlation with both disease activity measures and spinal structural damage, such as mSASSS and syndesmophyte number. These findings suggest that TBS may reflect trabecular microarchitecture changes resulting from cumulative inflammatory activity as well as current disease activity.
Bone disease in axSpA is a complex phenomenon, with both bone loss and new bone formation having an effect on clinical features of the disease25. Bone loss can appear as systemic bone loss, leading to osteoporosis and increased fractures, and as local bone loss, such as erosions. Trabecular bone in the vertebrae is the main site of inflammation in axSpA8 and trabecular bone loss is frequent in these patients11,23. More recently, trabecular bone loss has also been proposed as an important step in the pathogenesis of new bone formation in the spine7. One hypothesis for spinal progression in AS is that inflammation-induced bone loss causes instability, another type of biomechanical stress, which then leads to more bone formation to increase spinal stability. It is suggested that a change in bone microarchitecture in a part of the body where dynamic loading is important triggers a regenerative or reparative response26. Trabecular bone is the main load-bearing structure in the vertebrae27, which is directly affected by inflammation. Therefore, persistent inflammation may prevent the anabolic response from correcting any instability in the trabecular bone of the vertebral bodies, and relatively new bone formation in the cortical bone of the vertebrae may be increased at sites away from the inflammation7. This would result in the formation of syndesmophytes and/or bridging to compensate for a lack of stability in the spine28. The relative inaccessibility of the spine tissue and the lack of measures for assessing trabecular bone change means that, to date, there is little evidence to show that loss of bone and biomechanical instability may trigger new bone formation. Quantitative computed tomography has been developed to measure bone microarchitecture but cannot be performed routinely in a clinical setting due to the high radiation dose required, the cost, and limited access to such devices29. Although TBS is an indirect index for accessing trabecular bone, it has the advantage of being readily available in clinical practice using DXA images, and being able to assess the microarchitecture of trabecular bone at the lumbar spine.
We have previously shown that the inflammation on spinal MRI is negatively correlated with TBS in patients with AS and that the severity of local inflammation on spinal MRI was associated with trabecular bone loss30. The longitudinal observations in our present study show the relationship between loss of trabecular bone and disease activity measures over time in patients with axSpA. Also, TBS values were negatively correlated with mSASSS and syndesmophyte number, and the association was longitudinally observed in univariate GEE analysis. These data suggest that TBS in the vertebrae can consistently reflect microarchitectural change induced by inflammation in axSpA. Although the TBS was introduced as a tool for the assessment of osteoporosis risk, our data suggest the potential as a useful clinical method to assess inflammation-induced loss of trabecular bone in patients with axSpA. However, it is not yet clear whether the TBS could usefully predict further new bone formation in axSpA, and a prospective study would be required to evaluate this potential application.
This study has several limitations. The 4-year followup data are limited by the small sample size. The numbers of patients at Year 3 and Year 4 are small because the observation period was relatively short. Also, the proportion of patients with nr-axSpA in the study was relatively small. Although there was no association between disease activity measures and TBS over time in nr-axSpA patients (unlike in AS patients), it cannot be ruled out that the small sample size affected the results. Therefore, the results of the subgroup analysis in the nr-axSpA group should be interpreted with caution. Further studies are required to assess longitudinal associations in other patient cohorts and larger cohorts of nr-axSpA patients.
Clinical disease activity measures are longitudinally associated with trabecular bone loss, as assessed using the TBS. We found a relationship between the TBS and disease activity in patients with AS, but not in those with nr-axSpA.
- Accepted for publication November 4, 2019.








{kind=link}
{kind=link}