

Although tracheobronchial stenosis (TBS) is a relatively uncommon clinical manifestation of granulomatosis with polyangiitis (GPA)1,2, it can cause severe airway obstruction, leading to fatal consequences1,2,3,4,5.
A 43-year-old woman with biopsy-proven GPA presented with sudden severe chest pain and dyspnea without any other symptoms such as cough or fever. She had a 7-year history of recurrent orbital lesions, sinusitis, and septal perforation, controlled with 10 mg/day of prednisolone (PSL), tacrolimus, azathioprine, and rituximab. Her breathing sound was diminished in the left lung field. C-reactive protein and proteinase 3–antineutrophil cytoplasmic antibodies were negative. Chest radiography showed significant mediastinal shift due to atelectasis (Figure 1–A1). Computed tomography demonstrated complete obstruction of the left main stem bronchus (MSB; Figure 1–A2 to 1–A4). Bronchoscopy confirmed that the bronchial lumen was blocked with inflamed and necrotic tissue and bleeding (Figure 2). Cytology and culture of bronchoalveolar lavage fluid were negative. She was treated with pulsed methylprednisolone followed by 50 mg/day of PSL. On Day 5, the MSB obstruction was relieved without any mechanical therapies. Followup chest imaging in 2 months showed reopening of the obstructed bronchial lumen (Figure 1–B1 to 1–B4).

Chest radiographs (A1 and B1) and corresponding computed tomographic scans in axial (A2 and B2) and coronal (A3 and B3) planes, and with 3-D reconstruction (A4 and B4). A. Significant mediastinal shift due to total atelectasis of the left lung (A1) resulted from complete obstruction of the left main stem bronchus on Day 0 (A2–4: arrowhead). B. The atelectasis was drastically improved (B1) by reopening of the obstructed bronchial lumen after high-dose steroid therapy for 2 months (B2–4: arrowhead).

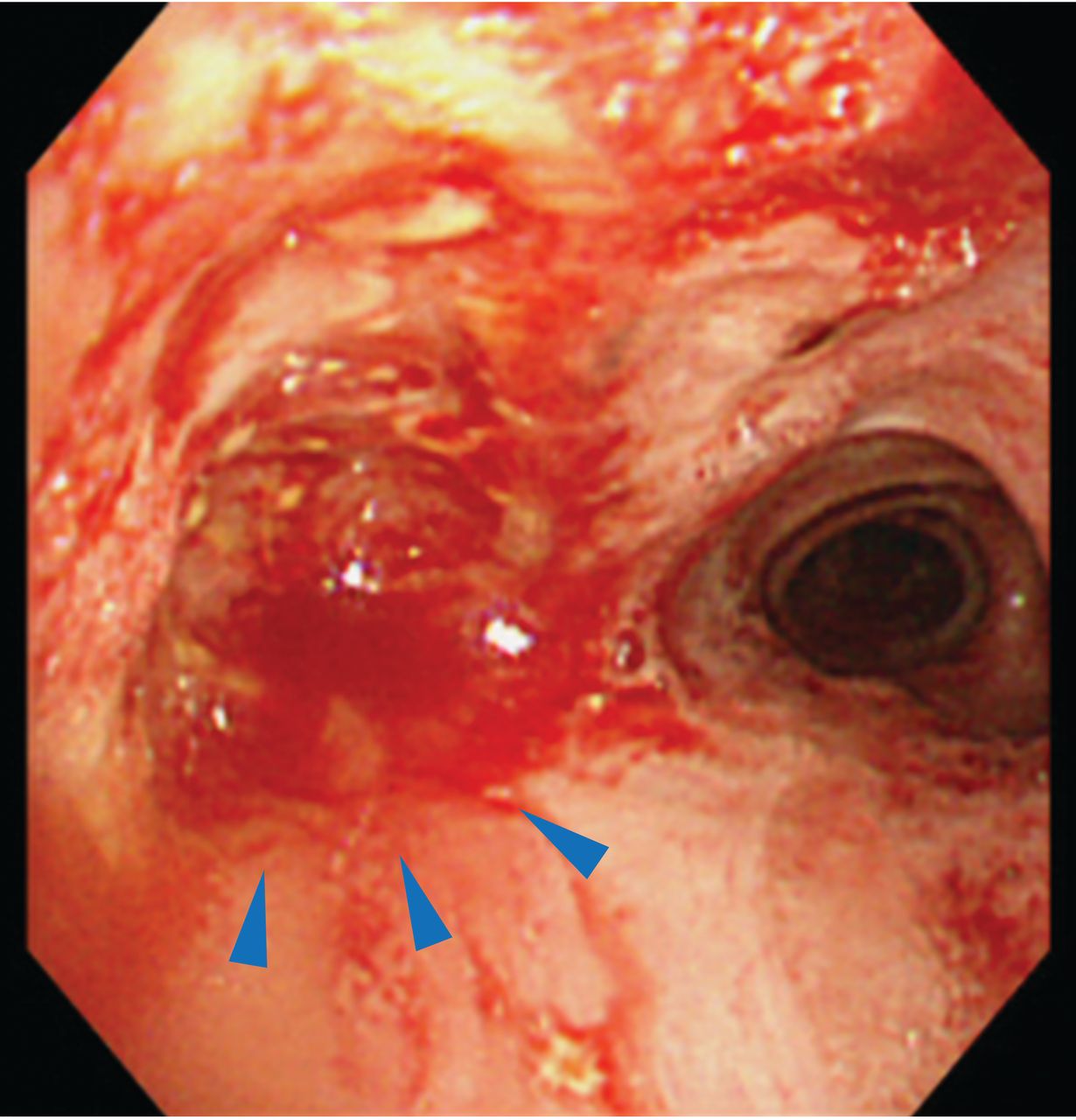
A bronchoscopic image of the tracheal bifurcation. The lumen of the left main stem bronchus was blocked with inflamed and necrotic tissue and bleeding (arrowheads).
There are relatively few reports focusing on treatments for TBS with GPA so far2,4,5. This is a highly notable case of unpredictable complete MSB obstruction without any other active symptoms, showing drastic improvement following high-dose steroid therapy. As previously reported, ENT manifestations are frequently associated with TBS1. Practitioners need to be aware of the importance of surveillance chest imaging for patients with GPA having ENT involvement, to detect TBS1.
Footnotes
The ethics review board at Tohoku University Hospital approved this report (#16840). The patient gave written informed consent to publish the material.








{kind=link}
{kind=link}