

Abstract
Objective. Behçet disease (BD) is a chronic inflammatory multiorgan disease. An increased risk of cardiovascular disease (CVD) and heightened death rate with BD have been suggested, but to our knowledge, a nationwide large-scale study has not been conducted to date. This study aimed to determine the overall CV risk and death rate in patients with BD versus controls using the Korean National Health Insurance Service claim database.
Methods. Patients with BD (n = 5576) with no previous history of CVD were selected from 2010 to 2014. An age- and sex-matched control population of individuals without BD (n = 27,880) was randomly sampled at a ratio of 5:1. Both cohorts were followed for incident CVD or all-cause death until 2015.
Results. The risks of myocardial infarction (HR 1.72, 95% CI 1.01–2.73) and stroke (HR 1.65, 95% CI 1.09–2.50) were significantly higher in patients with BD than in controls. Patients with BD also had a significantly higher risk of all-cause death (HR 1.82, 95% CI 1.40–2.37) compared to controls.
Conclusion. Korean patients with BD had a higher overall risk of CVD than did those without BD. Therefore, patients with BD must be carefully monitored for the potential development of CVD to ensure that appropriate early treatments are delivered.
Behçet disease (BD) is a chronic inflammatory multisystem disease of unknown etiology. It is characterized as a multi-system vasculitis that affects all types and sizes of blood vessels1. According to the International Study Group of Behçet’s Diseases, oral aphthosis is mandatory. The presence of any 2 of the following manifestations will diagnose the patients as having BD: genital aphthosis, uveitis or retinal vasculitis, erythema-nodosum like and papulopustular skin lesions, and a positive pathergy test2. The incidence of this disease varies according to geographical location, in that its prevalence is higher in the Mediterranean, Middle East, and Far East, including Korea3. Our group recently reported that the incidence of BD in Korea is relatively high at up to 3.98 per 100,000 person-years (PY)4. Both genetic susceptibility and environmental factors are thought to contribute to BD development.
BD is an inflammatory vascular disease; therefore, various vascular manifestations are prevalent in patients with BD. Several studies have previously investigated thrombophlebitis and thrombosis in both arteries or veins in patients with BD5,6,7,8,9. In a Turkish study, 14.7% of patients with BD had vascular involvement and the most frequent vascular event was deep vein thrombosis (67.1%)5. Another retrospective study reported that 13% of BD patients had superficial thrombophlebitis with vascular occlusion7. The incidence of arterial diseases in patients with BD varies from 0.5% to 17%10 and the reported prevalence of myocardial disease is only 1.1%11.
Caliskan, et al reported that endothelial and coronary microvascular functions are compromised in patients with BD, who present with significantly impaired coronary flow reserve compared to controls12. In a metaanalysis, patients with BD showed impaired flow-mediated dilatation and greater intima-media thickness of the carotid arteries compared to controls13. Ha, et al reported that patients with BD who underwent cardiac valve replacement surgery had frequent surgical complications, high treatment failure, and high postoperative mortality rates14.
Identification of an association between cardiovascular disease (CVD) and BD would both improve our understanding of BD and help to identify an appropriate diagnostic investigation for CV risk in affected patients. Therefore, in the present study, we investigated the CV risk in patients with BD using a nationwide insurance database in Korea.
MATERIAL AND METHODS
Database
Nearly all Korean citizens are enrolled, as required by law, in the Korean National Health Insurance Service (KNHIS) either as an employee or a community member. The KNHIS manages the National Health Insurance Sharing Service, which oversees a comprehensive health-related database. This database is available to researchers for use in policy or academic study efforts. This study was a nationwide population-based retrospective cohort study that used the KNHIS Claims Database [in which diagnoses are recorded using the International Classification of Diseases, 10th revision (ICD-10) code]. This database contains all claims data for the KNHIS program, the Korean Medical Aid program, and longterm care insurance. The KNHIS is a universal healthcare system that covers about 98% of the entire Korean population (including 50,455,745 individuals in 2010). The KNHIS database has been used in prior population-based studies15. Each patient’s identification number was anonymized to protect the individual’s privacy. This study was approved by the Institutional Review Board of the Korean National Institute for Bioethics Policy (NHIS-2017-1-121) and by the Ethics Committee of Seoul St. Mary’s Hospital, Catholic University of Korea (KC16EIS0917). The study was conducted according to the principles of the Declaration of Helsinki. Anonymized and deidentified information was used for analyses; therefore, informed consent was not required.
Study sample
The Korean government has enhanced benefit coverage for the following 4 major conditions: cancer, CVD, cerebrovascular disease, and rare intractable diseases. BD is categorized as a rare intractable disease. Within this system, the KNHIS has established a registration program for such diseases. All the patients diagnosed with BD (ICD-10 codes M35.2 and V139) between 2010 and 2014 were extracted from the database. Of these, patients younger than 20 years and/or those with a history of CVD between 2002 and 2010 were excluded. The control cohort was composed of age- and sex-matched patients without BD. The control groups were randomly extracted at a ratio of controls to cases of 5:1 (Figure 1), with the study’s exclusion criteria. Randomization was performed using an algorithm within the SAS version 9.4 software program (SAS Institute). These retrospective cohorts were followed for incident CVD or all-cause death until 2015.
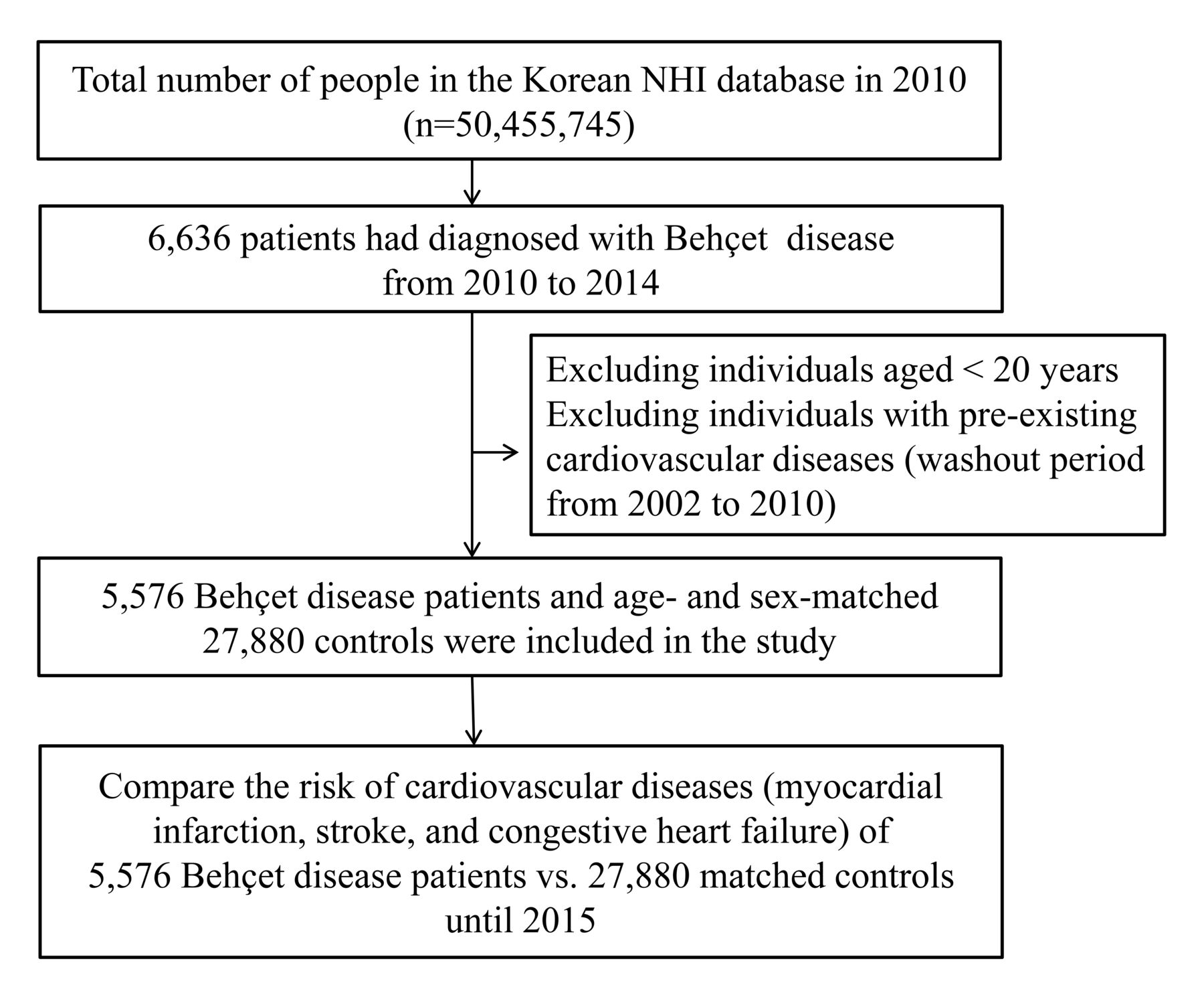
Study flowchart. NHI: National Health Insurance.
Outcome variables
The primary endpoint was the occurrence of CVD, including myocardial infarction (MI), stroke, and congestive heart failure (CHF). MI was defined according to the presence of at least one ICD-10 code for acute MI (I21-22), with hospitalization or more than 2 outpatient clinic visits. Stroke was defined according to the corresponding ICD-10 code (I63-43) for diagnoses made during hospitalization supported by a brain imaging study (e.g., computed tomography, magnetic resonance imaging). CHF was defined according to the presence of its corresponding ICD-10 code (I50) for hospitalization more than once.
The secondary endpoint was the death rate in both groups. Death rates regardless of causes of death were analyzed in both the BD group and the control group.
Covariate variables
Baseline characteristics relating to comorbidities were extracted from the medical claims according to their corresponding ICD-10 codes, prescription codes, and procedure codes. The presence of hypertension (HTN) was defined as at least 1 claim per year for the prescription of an antihypertensive agent under the ICD-10 codes I10–I15. The presence of dyslipidemia was defined by at least 1 claim per year for the prescription of an antihyperlipidemic agent under ICD-10 code E78. Type 2 diabetes mellitus (DM) was diagnosed according to its ICD-10 diagnostic codes (E11–E14) and the prescription of antidiabetic drugs.
Statistical analysis
Continuous variables are presented as means ± SD, while categorical variables are presented as numbers and percentages. To compare the characteristics between cohorts, the Student t test was used for continuous variables and the chi-square test was used for binary and categorical variables. The incidence of CVD was calculated per 1000 PY. The cumulative CVD incidence for each group was plotted with Kaplan–Meier curves and compared using the log-rank test. Multivariate Cox regression models were used to assess the risk of CVD. Results are presented as HR with 95% CI. All the statistical tests were 2-tailed with a significance level set at p < 0.05. Statistical analyses were performed using SAS version 9.4 (SAS Institute).
RESULTS
Baseline characteristics
A total of 5576 patients with BD and 27,880 matched controls were included in the study. Table 1 summarizes the baseline characteristics of the patient population and control cohorts. Because the cohorts were age- and sex-matched, the proportion of male patients (32.5%) and the mean ± SD age (43.4 ± 11.9 yrs) were the same between groups. There were no significant differences between the groups regarding the percentage of patients living in an urban habitat and those in the lowest quartile for income status. The proportions of HTN and dyslipidemia were significantly higher in patients with BD versus controls (11.4% vs 10.2% and 10.3% vs 7.0%; p < 0.01 and p < 0.0001, respectively). However, there was no difference regarding the prevalence of DM between patients with BD and healthy controls (4.1% vs 3.9%; p = 0.4).
Baseline characteristics by group.
Risk of CVD and all-cause death between the BD and control groups
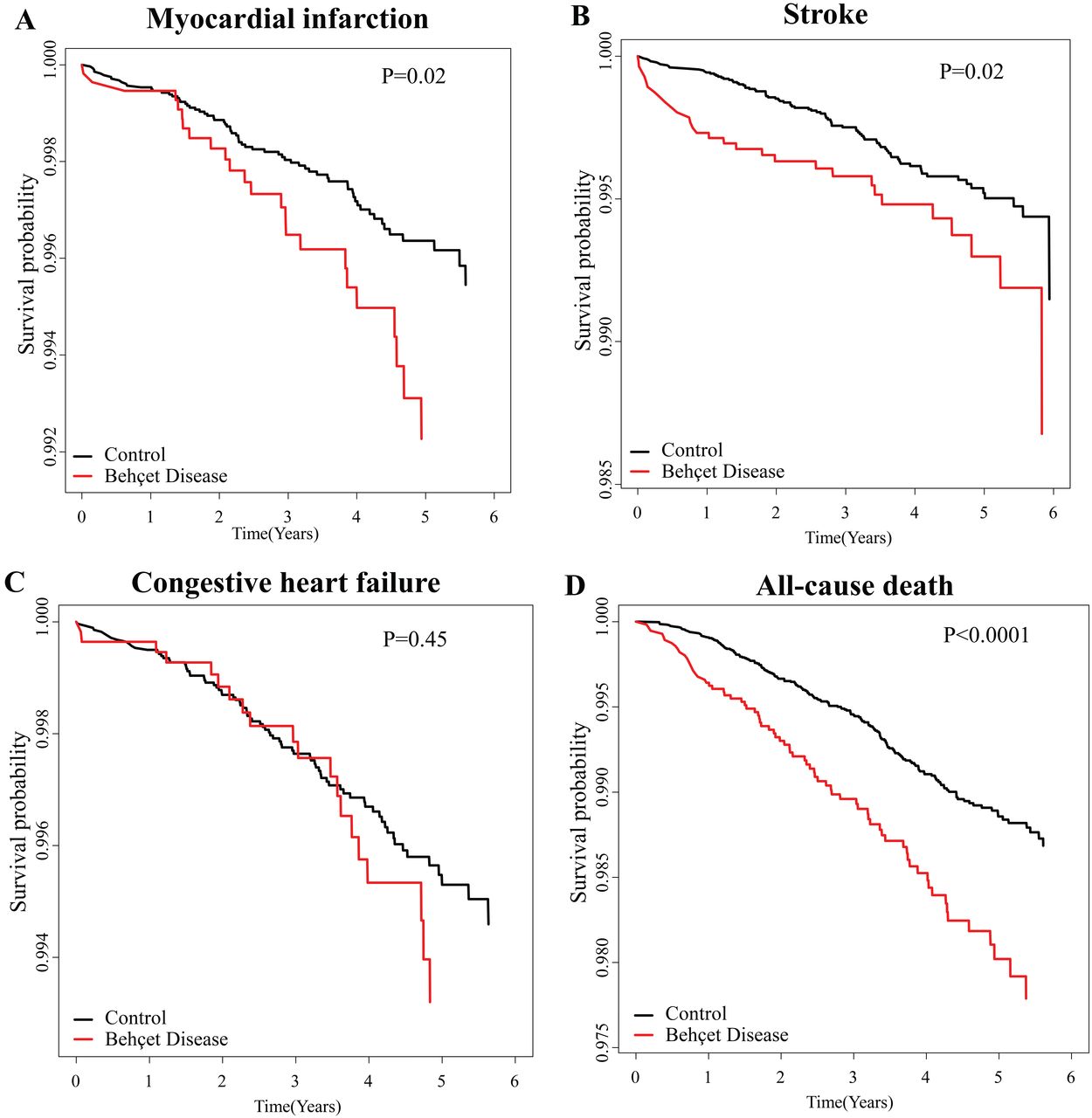
Figure 2 and Table 2 show the comparisons of CV events and all-cause death rate between controls and patients with BD. The risks of MI (HR 1.72, 95% CI 1.01–2.73) and stroke (HR 1.65, 95% CI 1.09–2.50) in patients with BD were significantly higher than in the controls. However, the risk of CHF was not statistically different between the 2 groups (HR 1.20, 95% CI 0.74–1.96). The risk of all-cause death in patients with BD was also significantly higher (HR 1.82, 95% CI 1.40–2.37) than in controls. The increased risk of MI, stroke, and all-cause death persisted following adjustment for covariates including income status, DM, HTN, and dyslipidemia (Table 2, Model 2).
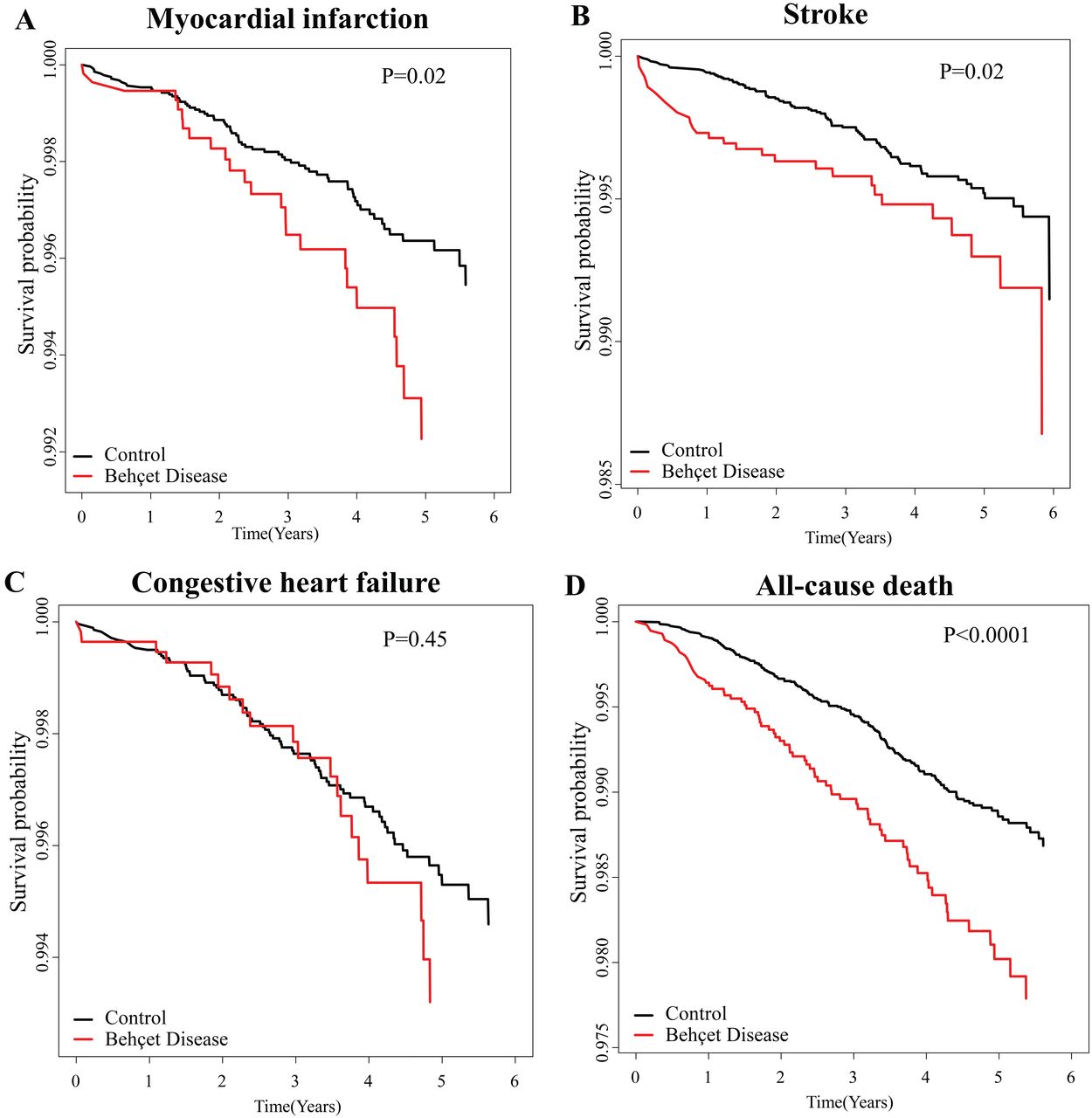
Comparing (A–C) cardiovascular events and (D) all-cause death between healthy controls and patients with Behcet disease with a log-rank p value.
Cardiovascular events and HR between healthy controls and patients with BD.
Subgroup analyses by age, sex, DM, HTN, and dyslipidemia
In female BD patients, the risks of MI (HR 2.48, 95% CI: 1.36–4.54), stroke (HR 2.05, 95% CI 1.20–3.50), and all-cause death (HR 1.91, 95% CI 1.31–2.78) were remarkably increased, whereas in male patients with BD, only the risk of all-cause death (HR 1.94, 95% CI 1.34–2.81) was increased significantly compared to females. Both younger patients (< 65 yrs) and older patients (65 yrs and older) showed an increased risk of all-cause death (HR 1.96, 95% CI 1.43–2.70 and HR 1.71, 95% CI 1.05–2.79, respectively). BD patients without DM showed increased risk of MI (HR 1.71, 95% CI 1.03–2.83), stroke (HR 1.66, 95% CI 1.06–2.60), and all-cause death (HR 1.96, 95% CI 1.48–2.61). BD patients without HTN had an increased risk of CHF (HR 1.78, 95% CI 1.01–3.15) and all-cause death (HR 1.75, 95% CI 1.28–2.41). The risk of MI (HR 1.96, 95% CI 1.14–3.36) and all-cause death (HR 1.99, 95% CI 1.50–2.63) was markedly increased in BD patients without dyslipidemia. BD patients with dyslipidemia showed remarkably increased risk of stroke (HR 2.43, 95% CI 1.09–5.40). All HR values were adjusted for age, sex, income status, DM, HTN, and dyslipidemia (Table 3).
Subgroup analysis of association between Behçet disease and the occurrence of myocardial infarction (MI), stroke, congestive heart failure (CHF), and all-cause death according to age, sex, DM, hypertension (HTN), and dyslipidemia.
DISCUSSION
This study used data from the KNHIS database to investigate CV risk in patients with BD. To the best of our knowledge, this is the first study to use a nationwide database to compare the incidence of CVD in BD patients and age- and sex-matched controls. Despite adjusting well-known risk factors of CVD (including age, sex, income status, HTN, DM, and dyslipidemia), the risk for CVD remains increased in patients with BD compared to those without BD.
The pathogenesis of CVD in BD is not well understood. It is possible that BD enhances inflammation in patients with underlying metabolic disorders prior to their BD diagnosis. In this study, the ratio of HTN and dyslipidemia was higher in the BD group than it was in the control group. It can be speculated that the elevated rates of HTN and dyslipidemia in patients with BD directly correlate with an increased rate of CV complications. However, the incidences of MI and stroke remained significant even after adjusting for these diseases. The results of subgroup analyses showed higher risk of CVD and death rate in female patients with BD, higher stroke rate in BD patients without DM, higher risk of CHF both in patients without HTN and dyslipidemia, or higher risk of MI and death rate in patients without dyslipidemia. The results proved that BD itself increased the risk of CVD.
BD is a systemic vasculitis that affects both small and large blood vessels. It is characterized by relapsing episodes of inflammation. The occurrence of MI and stroke in BD may be explained by various mechanisms. In particular, they are closely associated with vascular inflammation. C-reactive protein (CRP), which is used as an inflammatory biomarker, is increased in acute-phase BD, MI, and stroke16,17. Elevated CRP and systemic inflammation in BD are thought to increase the risks of MI and stroke.
In our study, the incidence of CHF was not significantly increased in patients with BD versus controls. This discrepancy, compared with the other cardiac findings, presumably occurred because CHF has many potential causes that are not necessarily directly related to systemic inflammation. MI is one of the major causes of CHF. However, there are also multiple non-ischemic causes of CHF, including valvular heart disease, hyperthyroidism, and dilated cardiomyopathy18.
We found that the HR of all-cause death (1.82, 95% CI 1.40–2.37) was significantly higher in patients with BD than in the control group. Additionally, the HR of all-cause death was higher than those of MI (1.72, 95% CI 1.01–2.73) and stroke (1.65, 95% CI 1.09–2.50). After adjusting for variables including HTN, DM, and dyslipidemia, the HR of all-cause death increased to 1.92 (95% CI 1.47–2.50). A possible explanation is that patients with BD have an increased risk of death owing to a severe disease course, including CVD or cancer. In particular, our group recently found that BD was associated with leukemia, lymphoma, cancers of the oral cavity and pharynx, thyroid cancer, and prostate cancer19. Other CV complications including thrombophlebitis, thrombosis, aneurysmal change, valvular heart disease, and pericarditis can also be associated with an increased death rate in patients with BD.
The mechanism and relationship between BD and CVD have not been elucidated yet, but we could find a clue in the relationship between psoriasis and CVD. Psoriasis, another well-known inflammatory skin disease, increases the risk of CVD including MI, stroke, and CV mortality20,21. The mechanism by which psoriasis contributes to CVD involves common inflammatory pathways, shared genetic factors, the secretion of adipokines, insulin resistance, lipoprotein composition and function, angiogenesis, oxidative stress, microparticles, and hypercoagulability22. This relationship between psoriasis and CVD can be used as a reference to further understand that of BD and CVD. Just as tumor necrosis factor (TNF)-α inhibitors have therapeutic effects on psoriasis, a recent large retrospective study revealed the therapeutic effects of TNF-α inhibitors for inducing the resolution of venous thrombosis in patients with BD23.
This study has several limitations. The first limitation is that we did not obtain data regarding potential CV-associated covariates, including smoking habits, alcohol consumption, body mass index, and family history. Especially, there can be the bias of lack of data for history of smoking as a major risk factor for CVD. In addition, the disease severity and the drugs used to treat BD, which may influence the risk of CVD, were unclear. Third, the causes of death in patients with BD were neither confirmed nor analyzed. Fourth, the followup time in our study was considered relatively short and insufficient for observing the development of incident CVD or death rate. Concerns have been raised about ascertainment bias, i.e., that patients with BD were more likely to see their doctors. Therefore, further studies regarding the relationship of BD and the increased risk of CVD and death rate are needed to substantiate our findings. Fifth, although the exact causes of stroke or MI of affected patients with BD (whether vascular events, central nervous system involvement, or other arterial involvement of BD) might be evaluated by chart review of individuals, chart review was not possible when using the KNHIS database, which is composed of deidentified information.
We evaluated CV risk in Korean patients with BD compared to age- and sex-matched controls. We found that patients with BD had a higher incidence of MI, stroke, and all-cause death than did those without BD. Patients with BD, therefore, must be carefully screened regarding CV risk, and the early treatment of underlying diseases is necessary in patients with BD.
Footnotes
This study was supported by the National Research Foundation of Korea grant funded by the Korean government (MSIP; no. 2016R1C1B1008288 and 2019R1F1A1056601).
- Accepted for publication July 8, 2019.








{kind=link}
{kind=link}