

Abstract
Objective. To estimate the frequency of patients with psoriatic arthritis (PsA) achieving minimal disease activity (MDA) status in real-world studies and randomized controlled trials (RCT).
Methods. A systematic literature search for 2009–2017 was performed in PubMed, Embase, Cochrane Library, and LILACS. Study selection and data extraction were performed by 2 independent researchers. Random-effects single-arm metaanalyses were performed and heterogeneity was assessed using I2.
Results. A total of 405 records were identified and 45 studies were analyzed: 39 (86.7%) observational studies and 6 (13.3%) RCT; they included 12,469 patients. The overall prevalence of MDA in cross-sectional studies was 35% (95% CI 30%–41%, I2 = 94%), varying from 17% (95% CI 7%–34%) in patients taking synthetic disease-modifying antirheumatic drugs (DMARD) to 57% (95% CI 41%–71%) in those taking biological DMARD. Prevalence of MDA in cohort studies increased with longer followup time, ranging from 25% (95% CI 15%–40%) with 3- to 4-month followup to 42% (95% CI 38%–45%) with > 24-month followup. Patients with PsA receiving biological DMARD in a real-world context and RCT had similar prevalence of MDA at 6-month followup: 30% (95% CI 21%–41%, I2 = 85%) versus 32% (95% CI 26%–39%, I2 = 79%), respectively.
Conclusion. Patients with PsA included in real-world studies had similar prevalence of MDA compared to those in controlled clinical trials. This finding suggests that MDA is a useful treatment target for PsA in the real-world setting.
Psoriatic arthritis (PsA) is a chronic inflammatory disease that affects 20%–33% of individuals with psoriasis, and about 130 in every 100,000 individuals worldwide1,2. PsA has heterogeneous manifestations, affecting peripheral and axial joints, skin, nails, and entheses3.
Minimal disease activity (MDA) criteria have been recommended as a therapeutic target in PsA4,5. Patients are classified as achieving MDA if they fulfill 5 out of 7 outcome measures: tender joint count (TJC) ≤ 1; swollen joint count (SJC) ≤ 1; Psoriasis Area and Severity Index ≤ 1 or body surface area ≤ 3; patient pain on visual analog scale (pain VAS) score ≤ 15; patient global disease activity (global VAS) score ≤ 20; Health Assessment Questionnaire score ≤ 0.5; and tender entheseal points ≤ 16.
The prevalence of MDA has been assessed in several trials and its frequency varies according to the study design, drug used, and time of evaluation. According to a recent publication, the frequency of MDA in randomized controlled trials (RCT) varies from 24% to 52% with tumor necrosis factor (TNF) inhibitor therapy and from 14% to 41% with secukinumab therapy, and from 40% to 64% in observational studies7.
Participants in RCT usually present higher levels of disease activity, fewer comorbidities8, and better adherence rates to therapy than patients analyzed in observational studies9. In real life, factors such as poor adherence and restricted access to drugs preclude the achievement of MDA status in a treat-to-target strategy10.
The aim of our investigation was to analyze the frequency of patients with PsA achieving MDA status in real-world studies and RCT.
MATERIALS AND METHODS
Our study is a systematic review with metaanalysis of observational and interventional studies reporting MDA in patients with PsA.
Study protocol
The protocol for this systematic review is found in the international prospective register of systematic reviews (PROSPERO), record number CRD42016050502.
An extensive literature search was performed in April 2017 in PubMed, Embase, Cochrane, and LILACS with no limits or filters. The following search strategies were used.
PubMed and Cochrane: ((“minimal disease activity” OR “minimal disease activities” OR “MDA”)) AND “Arthritis, Psoriatic” [MESH] OR “Psoriasis, Arthritic” OR “Arthritic Psoriasis” OR “Psoriatic Arthritis” OR “Psoriasis Arthropathica” OR “Psoriatic Arthropathy” OR “Arthropathies, Psoriatic” OR “Arthropathy, Psoriatic” OR “Psoriatic Arthropathies” OR “Spondylarthropathies” [MESH] OR “Marie-Strumpell Spondylitis” OR “Marie Strumpell Spondylitis” OR “Spondylitis, Marie-Strumpell” OR “Spondyloarthropathy” OR “Spondyloarthropathies” OR “Bechterew Syndrome” OR “Syndrome, Bechterew” OR “Spondylarthropathy” OR “Spondylarthritis” [MESH] OR “Spondylarthritides” OR “Spinal Arthritis” OR “Spinal Arthritides” OR “Arthritis, Spinal”).
Embase: ‘minimal disease activity’ OR ‘minimal disease activities’ OR ‘MDA’ AND ‘psoriatic arthritis’/exp OR ‘psoriatic arthritis’ OR ‘alibertbazin disease’ OR ‘arthritis psoriatica’ OR ‘arthritis, psoriatic’ OR ‘arthritis, psoriasis’ OR ‘arthritis, psoriatic’ OR ‘arthropathic psoriasis’ OR ‘arthropathy, psoriatic’ OR ‘disease, alibertbazin’ OR ‘polyarthritis, psoriatic’ OR ‘psoriasis arthropathica’ OR ‘psoriasis pustulosaarthropathica’ OR ‘psoriasis, arthritis’ OR ‘psoriatic arthropathy’ OR ‘psoriatic polyarthritis’ OR ‘psoriatic rheumatism’ OR ‘psoriatic rheumatoid arthritis’ OR ‘rheumatoid arthritis, psoriatic’.
LILACS: Minimal AND disease AND activity AND psoriatic arthritis.
An active search was carried out for abstracts presented from 2009 to 2017 in the European League Against Rheumatism (EULAR) Annual European Congress of Rheumatology, the American College of Rheumatology Annual Meeting, the World Psoriasis and Psoriatic Arthritis Conference, the International Congress of Spondyloarthropathies, and the Brazilian Congress of Rheumatology.
Inclusion criteria were original studies reporting the prevalence of MDA status among adult patients with PsA.
Exclusion criteria were (1) duplicates (in case of duplicates, the most complete publication was included, e.g., in case of abstracts and original articles reporting the same results, only the complete original article results were considered); (2) review articles, letters to the editor, case reports; (3) articles not describing MDA according to Coates and Helliwell6, e.g., studies that evaluated number of swollen joints other than 66 and tender joints other than 68, studies that did not evaluate enthesitis, etc.; and (4) articles reporting only the prevalence of sustained MDA.
Selection of studies: 2 reviewers (MZ and CK) independently selected the articles by title and abstract. In the next step, 2 researchers (MZ and PP) independently selected the articles based on full text. Disagreements were resolved by consensus.
Data collection
The following data were extracted: first author, year of publication, country where study was conducted, duration of study, type of publication (original article vs abstract presented in congress), study design (RCT, cohort, cross-sectional), total number of patients included in study, total number and relative frequency of women included in study, mean age of population, PsA duration, number of comorbidities, time of evaluation, number and percentage of participants achieving MDA status, and mean and SD of each component of MDA criteria. The type of treatment was assessed and classified as biological disease-modifying antirheumatic drug (bDMARD) monotherapy, synthetic DMARD (sDMARD) monotherapy, combined bDMARD + sDMARD therapy, nonsteroidal antiinflammatory drugs (NSAID), and unspecified treatment.
These data were independently extracted from articles by 2 reviewers (MZ and CS), and disagreements were resolved by consensus.
Statistical analyses
To analyze the prevalence of MDA in observational trials, a single-arm metaanalysis was performed, grouping both cohort and cross-sectional studies and including all observational trials irrespective of treatment evaluated. The final followup time of each cohort study was considered in the analysis.
Subsequently, the studies were separated according to design: a single-arm metaanalysis including only cross-sectional studies was performed and another analysis including only cohort studies according to followup time (baseline, 3–4 mos, 6–8 mos, 12–13 mos, and 24–60 mos) was conducted.
RCT
Single-arm metaanalysis was performed to estimate the frequency of MDA in RCT, considering maximum followup time and including all RCT irrespective of treatment evaluated.
A single-arm metaanalysis was also performed to analyze the frequency of MDA in patients treated with bDMARD in real-world studies and RCT at the 6-month followup.
The results of the metaanalyses were represented by forest plots. The I2 index was used to assess heterogeneity. When relevant heterogeneity was found (I2 index ≥ 50%), the results from the random-effects model were shown, and in cases in which I2 was < 50%, the fixed-effects model was used11.
RESULTS
A total of 405 records were identified from databases. Of them, 274 were excluded by title and abstract and 96 studies were excluded after full-text analysis. Ten abstracts were identified. The 45 eligible studies included in the final analysis are listed in Table 1. An illustration summarizing the selection of studies is given in Figure 1.

A summary of the selection of studies. MDA: minimal disease activity.
The 45 studies eligible for inclusion in our analysis comprised data for 12,469 patients.
The 45 selected studies included 12,469 patients, mean age 51.0 (SD ± 3.3) years, mostly men (n = 6386, 51.2%), with a mean PsA disease duration of 8.1 (SD ± 3.6) years. Thirty-nine (86.7%) were real-world studies and only 6 (13.3%) were RCT. Observational studies, on average, had larger populations and longer followup times compared to RCT. Among the 39 observational studies, 19 (48.7%) were carried out in Europe and 10 (25.6%) in North America, and 37 (94.9%) were conducted in university hospitals.
The characteristics of studies included in the analysis are shown in Table 2.
Characteristics of studies included in the analysis.
The assessment of bias is described in Supplementary Tables 1–3, available from the authors on request.
Frequency of MDA in real-life studies
The frequency of PsA patients achieving MDA status in real-world studies was 37% (95% CI 34%–41%, I2 = 93%) when both cross-sectional and cohort studies were grouped and all types of treatment were considered. When only cross-sectional studies were considered (n = 22), the overall frequency of MDA was 35% (95% CI 30%–41%, I2 = 94%; Figure 2), varying from 17% (95% CI 7%–34%) in the sole study that specified that patients were taking sDMARD to 57% (95% CI 41%–71%, I2 = 87%) in studies evaluating patients in use of anti-TNF therapy. Assessment of the prevalence of MDA in a real-world context in different treatment subgroups was restricted because 81.8% (n = 18) of cross-sectional studies did not specify the patients’ current therapy.
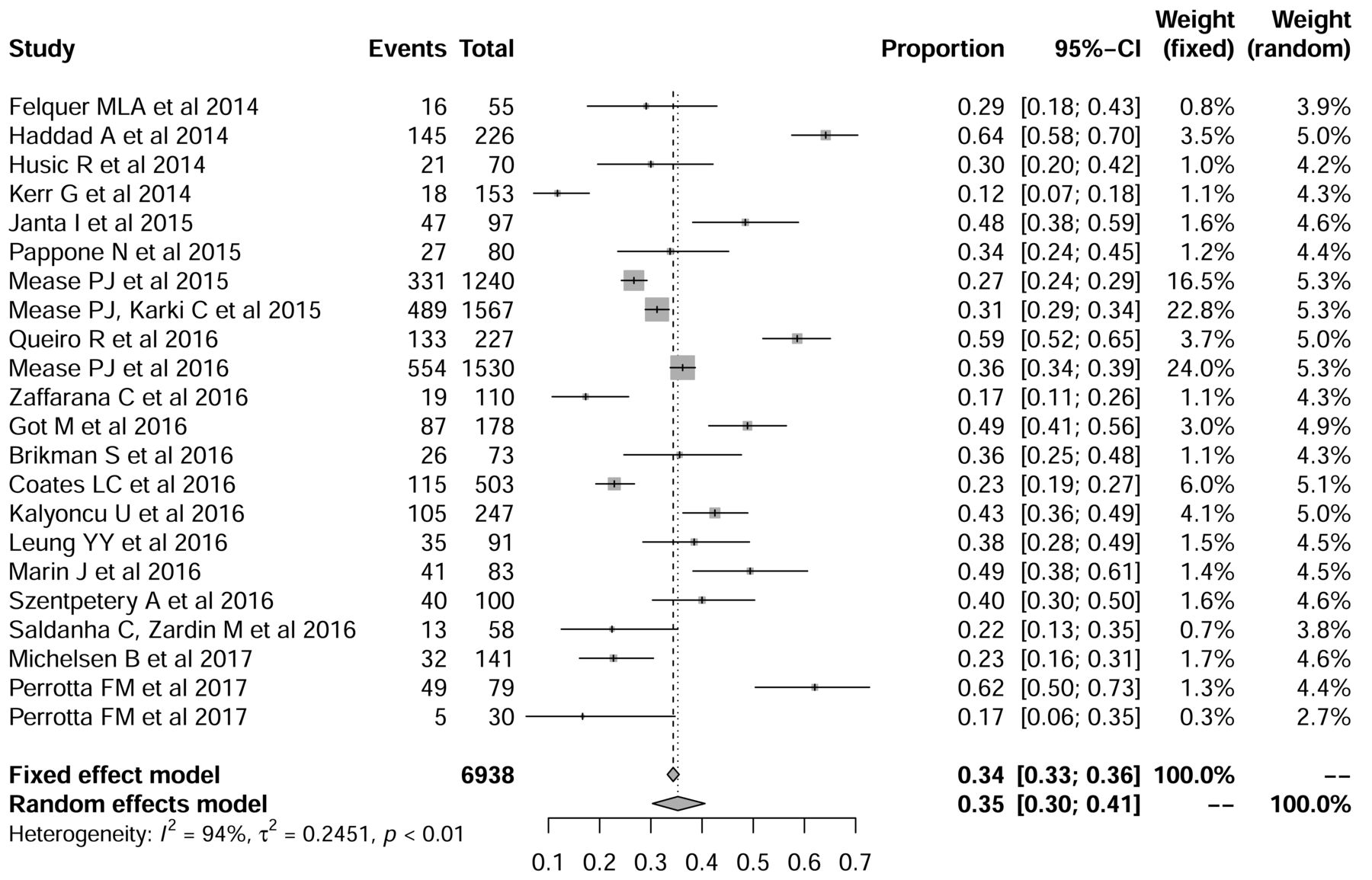
The overall frequency of minimal disease activity was 35% when cross-sectional studies only were considered (n = 22).
In cohort studies, the frequency of patients with MDA increased with longer followup time, varying from 25% (95% CI 15%–40%, I2 = 87%) when MDA was evaluated at 3–4 months, to 30% (95% CI 21%–42%, I2 = 94%) at 6–8 months, 42% (95% CI 39%–46%, I2 = 68%) at 12–13 months, and 42% (95% CI 38%–45%, I2 = 64%) in studies with ≥ 24 months followup (Supplementary Figure 1, available from the authors on request). When patients treated with biological drugs in cohort studies were compared to those treated with bDMARD in RCT, the frequency of MDA was similar at 6 months’ followup: 30% (95% CI 21%–41%, I2 = 85%) versus 32% (95% CI 26%–39%, I2 = 79%), respectively (Supplementary Figure 3).
Frequency of MDA in RCT
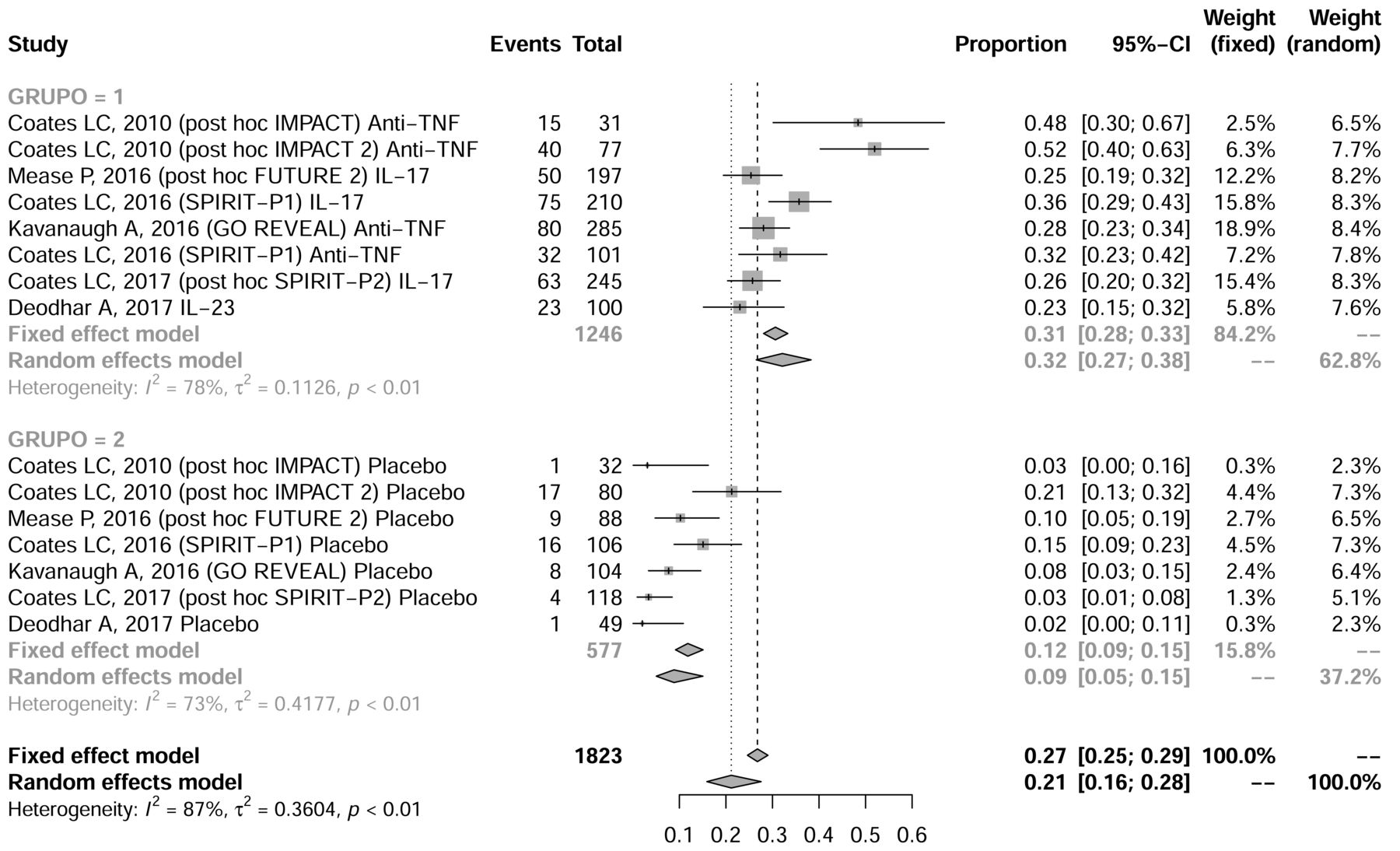
The 6 titles included in the analysis evaluated 7 RCT (1 report described the results of 2 RCT) and all were trials evaluating biological therapy. When all biological therapies (anti-TNF, anti-IL-17, and anti-IL-12/23) were grouped, the prevalence of PsA patients with MDA status was 32% (95% CI 27%–38%, I2 = 78%) in the biological therapy arm, compared with only 9% of patients with MDA in the placebo group (95% CI 5%–15%, I2 = 78%) at roughly 6 months’ followup (Figure 3). The prevalence of MDA was similar across studies of bDMARD therapy: 30% (95% CI 27%–51%, I2 = 83%) in studies evaluating anti-TNF therapy, 29% (95% CI 23%–36%, I2 = 72%) in those evaluating anti-interleukin (IL) 17 drugs, and 23% (95% CI 16%–32%, I2 not applicable) in the sole study evaluating anti–IL-12/23 therapy included in the analysis (Supplementary Figure 2, available from the authors on request).

When all biological therapies (anti-TNF, anti-IL-17, and anti–IL-12/23) were grouped, the prevalence of PsA patients with minimal disease activity (MDA) status was 32% in the biological therapy arm, compared to only 9% of patients with MDA in the placebo group at 6 months of followup. TNF: tumor necrosis factor; IL: interleukin; PsA: psoriatic arthritis.
DISCUSSION
To our knowledge, this is the first systematic literature review with a metaanalysis to compare performance of MDA in RCT and observational studies of patients with PsA. Knowing how MDA performs in RCT and real-life scenarios may contribute to improving its feasibility. Our work showed that about one-third of patients with PsA evaluated in cross-sectional studies were in a state of MDA, with this value varying from 17% (95% CI 7%–34%) with the use of sDMARD to 57% (95% CI 41%–71%) with bDMARD. In addition, the longer the followup time in real-world studies, the higher the prevalence of patients achieving MDA. Patients receiving bDMARD had similar prevalence of MDA status at 6 months’ followup in RCT and observational studies.
The initial hypothesis predicted a higher frequency of MDA in RCT due to better adherence to therapy, because barriers to acquisition of medication and cost of therapy can be problems in daily life. However, even in RCT, adherence rates can range from 43% to 78% among patients receiving treatment for chronic diseases. The factors that are related to lower adherence in RCT and real-world studies include psychiatric comorbidities, cognitive impairment, inadequate followup, adverse effects of medication, poor physician-patient relationship, missed appointments, and treatment complexity9.
Patients included in RCT usually have higher levels of disease activity than those in real-world studies55, and this may limit the final outcomes of the studies8, preventing patients from achieving MDA.
On the other hand, in real-world studies we expect lower response rates because of lower adherence, but in this case, most of the patients have milder disease. Thus we expect lower response rates because of lower adherence to therapy but higher response because disease is milder and treatment is open-label.
In our investigation, RCT and real-world studies had similar frequencies of MDA probably because the selected observational studies were carried out mainly in university hospitals located in developed countries, where patients with PsA have adequate education levels, receive a high standard of care, and have easy access to DMARD. In underdeveloped countries, in contrast, restricted access to DMARD and low education levels leading to poor understanding of medication instructions were barriers to achieving MDA in the real-world context10.
Our results were similar to those from a study12 that described the frequency of MDA in RCT varying from 24% to 52% in patients receiving anti-TNF therapy, and from 23% to 28% in those receiving secukinumab (at 16 weeks). In observational studies, the frequency of MDA was 44%–64% at 12 months, and 40% at the 5-year followup7. Another study described that the frequency of MDA in real-life studies ranged from 15% to 64%49.
Limitations of our report are the great heterogeneity regarding characteristics of patients, current therapies, and followup times in the studies we investigated. There was greater amplitude in effect sizes among observational studies compared to RCT, suggesting that the groups included in the real-life studies were more heterogeneous. In addition, the majority of real-life studies did not specify the current treatment of patients or describe the MDA in the different treatment subgroups. Further, in many studies assessment of MDA was not the primary outcome and its prevalence was described only in posthoc analysis.
A priori observational studies are expected to have greater heterogeneity owing to the role of uncontrolled factors influencing achievement of MDA. The lack of a standardized treatment protocol within the same study and across various scenarios is a key factor explaining the different results. Also, in cohort and case-control studies, missing data may significantly affect the outcomes and no imputation is usually reported.
We acknowledge that in this case clinical heterogeneity should be considered a limitation in the lack of statistical homogeneity. Variances in inclusion criteria could affect achievement of MDA, even with similar treatment strategy protocols. This is particularly relevant in RCT. For example, in the IMPACT trial, 5 or more swollen/tender joints were considered as inclusion criteria, whereas in the FUTURE-2 and SPIRIT-P1 studies, 3 or more tender/swollen joints were required for inclusion. As well, previous treatments differed among studies. For instance, in FUTURE-2, participants could have failed NSAID, synthetic DMARD, or TNF inhibitors, whereas in SPIRIT-P1, subjects were required to be TNF inhibitor–naive, and in SPIRIT-P2 they were included only after an inadequate response to TNF inhibitor therapy.
We observed that patients with PsA included in real-world studies reported recently had similar prevalence of MDA compared to those participating in controlled clinical trials. This finding suggests that MDA is a useful treatment target for PsA in a real-world context.
Footnotes
Supported by Fundo de Incentivo à Pesquisa e Eventos do Hospital de Clínicas de Porto Alegre.
- Accepted for publication September 18, 2019.








{kind=link}
{kind=link}
{kind=link}