

Abstract
Objective. To assess longterm effectiveness of tumor necrosis factor inhibitors (TNFi) in patients with psoriatic arthritis (PsA) registered in the Rheumatic Diseases Portuguese Register, exposed to at least 1 TNFi, prospectively followed between 2001 and 2017.
Methods. Kaplan-Meier analysis was performed for first-, second-, and third-line TNFi. Responses included European League Against Rheumatism (EULAR) criteria, Disease Activity Index for Psoriatic Arthritis (DAPSA), minimal disease activity (MDA), and Ankylosing Spondylitis Disease Activity Score (ASDAS) at 3 and 6 months. Baseline predictors of discontinuation and response were studied using Cox and multivariable multinomial/logistic regression models.
Results. The 750 patients with PsA showed drug retention of 4.1 ± 3.4 years (followup 5.8 ± 3.8 yrs) for first TNFi. Switching to a second (189 patients) or third (50 patients) TNFi further decreased survival by 1.1 years. Female sex, higher baseline 28-joint count Disease Activity Score, and infliximab were predictors of first TNFi discontinuation. After 6 months of the first TNFi, 48.7% of patients achieved a good EULAR criteria response and 20.9% were in DAPSA remission. There were 11.4% in MDA, and 56.4% had a good ASDAS. Responses to the second TNFi were significantly inferior compared to responses to the first TNFi. Female sex and higher baseline Health Assessment Questionnaire–Disability Index were negatively associated with good EULAR response at 3 months, and obesity decreased the chance of response at 6 months.
Conclusion. In this study, switching to a second or third TNFi was associated with significantly lower drug survival and response rates for patients with axial and peripheral PsA subtypes. More successful therapeutic approaches will require considering the effect of sex and obesity on TNFi effectiveness.
The development of tumor necrosis factor inhibitor (TNFi) therapies has dramatically improved the management of psoriatic arthritis (PsA). Despite the effectiveness of these agents, a significant proportion of patients do not respond and/or are intolerant to TNFi, requiring treatment discontinuation and/or switching to adequately control disease activity1. Several questions regarding sequential therapeutic approaches remain unanswered. Clinical recommendations suggest that switching between TNFi should be considered when one proves ineffective or toxic, although real-world research shows reduced drug retention rates and poorer responses after switching2,3. The analysis of registry data, after many years of followup, provides a fundamental tool to assess the performance of sequential therapeutic options and to support treatment decision algorithms.
The aim of this Exchange PsA study was to assess the longterm effectiveness of TNFi for the treatment of patients with PsA registered in the Rheumatic Diseases Portuguese Register (Reuma.pt) according to drug retention and response rates for first-, second-, and third-line biologic treatment options. The frequency of, and main reasons for, TNFi discontinuation as well as predictors of discontinuation and response were also examined.
MATERIALS AND METHODS
The Exchange PsA study was an observational study of patients with PsA, including all Moll and Wright classification subtypes4. These patients were followed at Reuma.pt, an electronic prospective nationwide rheumatic disease register implemented in 2008 with standardized data collection for patients, including those treated with biologic (b) and conventional synthetic (cs) disease-modifying antirheumatic drugs (DMARD) from all Rheumatology Departments of mainland Portugal, Madeira, and the Azores Islands5,6. Patients with a PsA diagnosis treated with bDMARD are registered in Reuma.pt as per clinical practice according to local recommendations7, and this cohort is therefore considered to be representative of the national PsA population. All patients with PsA who were registered in Reuma.pt between 2001 and 2017 and exposed to at least 1 administration of a TNFi were included in the persistence analysis, and those with at least 12 weeks of therapy with a TNFi were included in the effectiveness analysis. Data from before 2008 were prospectively recorded in a paper-based followup protocol and retrospectively introduced into Reuma.pt as described8.
Demographics, disease characteristics, concomitant treatments, and type of TNFi were assessed at baseline. At baseline (up to + 15 days) and followup evaluations, these variables were determined: disease activity [tender (68) and swollen joints (66), visual analog scale (VAS) for global disease activity (patient and physician) and for pain (patient), 4-variable 28-joint count Disease Activity Score using erythrocyte sedimentation rate (DAS28-4vESR) for peripheral disease, Bath Ankylosing Spondylitis Disease Activity Index for axial disease and enthesitis], and function [Health Assessment Questionnaire–Disability Index (HAQ-DI) for peripheral disease and Bath Ankylosing Spondylitis Functional Index (BASFI) for axial disease]. Response was measured at 3 months (−30 to +60 days) and 6 months (−30 to +90 days) by composite indices and according to disease phenotype as follows: European League Against Rheumatism (EULAR), Psoriatic Arthritis Response Criteria (PsARC), Disease Activity Index for Psoriatic Arthritis (DAPSA), and minimal disease activity (MDA) for all patients with peripheral disease, and Ankylosing Spondylitis Disease Activity Score (ASDAS) only for those with axial involvement. Functional indices were analyzed as ΔHAQ-DI and ΔBASFI from baseline. Ineffective TNFi included both primary (before 6 mos) and secondary (after 6 mos) therapy failures, according to the treating rheumatologist, based on predefined fields. The LUNDEX method was applied to correct for withdrawals9.
The baseline characteristics were compared between those who continued and discontinued therapy, among those prescribed different TNFi as first-line therapy, and between sexes using the Student t test, proportion test, and chi-square/Fisher’s exact test as appropriate. A similar approach was used to compare treatment responses at 3 and 6 months, between first and second TNFi therapy, and between second and third TNFi therapy.
Drug retention was defined as the time until treatment discontinuation due to adverse events or ineffectiveness and was calculated using the Kaplan-Meier method; this value was later adjusted for the year of starting the TNFi according to a Cox model10. Discontinuation was defined as either the end of treatment (i.e., ≥ 1 yr of continuous interruption of the treatment without the introduction of another TNFi) or as a switch in treatment to any other biologic. Patients who discontinued treatment for other reasons than adverse events or ineffectiveness were censored. Equality of the survival curves was assessed by the Wilcox (Breslow) method.
To determine predictors of discontinuation of the first TNFi, we used a Cox model that evaluated discontinuation independently of the indication and a multinomial multivariable logistic regression for analyzing predictors according to the reason of discontinuation. To obtain a predictor model for response for peripheral PsA, we used a multivariable logistic regression that considered good EULAR response criteria at 3 and 6 months. All variables considered clinically relevant were assessed by univariable logistic regression, and those with p < 0.20 were considered (except for sex, age at first TNFi, phenotype, and year of starting a TNFi that were forced into the model) and selected by stepwise selection method.
Missing data were interpreted as random, and a complete case analysis was performed using Stata software IC version 12 (StataCorp.) with the significance level set at p ≤ 0.05.
This study was conducted according to the Declaration of Helsinki and the International Guidelines for Ethical Review of Epidemiological Studies and approved by the Ethics Committee of Centro Académico de Medicina de Lisboa (98/17). Reuma.pt was approved by the Portuguese Data Protection Authority, and all patients provided written informed consent for anonymized data collection and publication.
RESULTS
A total of 750 patients with a diagnosis of PsA and treatment with at least 1 TNFi were identified in Reuma.pt (Figure 1). The baseline characteristics of the study population at the time of first TNFi prescription are detailed in Table 1 and Supplementary Table 1 (according to TNFi), and Supplementary Table 2 (according to sex; available with the online version of this article). The predominant PsA subtype was polyarthritis followed by the predominantly axial form, but all Moll and Wright subtypes were represented in this population. Baseline peripheral disease activity was moderate as assessed by the mean DAS28-4vESR, high per DAPSA, and very high per ASDAS for those with axial involvement. Etanercept (ETN) was the most frequently prescribed first-line TNFi (44.7%) followed by adalimumab (ADA; 26.7%), golimumab (15.2%), and infliximab (IFX; 13.5%). Methotrexate (MTX) was prescribed for 62.3% of the patients.

Flow diagram of patients with psoriatic arthritis (PsA) registered at Reuma.pt, treated with tumor necrosis inhibitors (TNFi) as first, second, and third therapeutic lines. * Other reasons include patients’ willingness, surgery or pregnancy related, remission, loss to followup, or death. Patients could have registered more than 1 reason for TNFi discontinuation. & Differences between the first- and second-line TNFi for each reason of discontinuation: ineffectiveness (p = 0.139), adverse events (p = 0.938), and other reasons (p = 0.146). ¥ Differences between the second- and third-line TNFi for each reason of discontinuation: ineffectiveness (p = 0.658), adverse events (p = 0.926), and other reasons (p = 0.259). bDMARD: biological disease-modifying antirheumatic drug; csDMARD: conventional synthetic DMARD.
Baseline demographic and disease characteristics of patients with psoriatic arthritis registered at Reuma.pt, treated with a first tumor necrosis factor inhibitor (TNFi), including those who continued and discontinued therapy.
Baseline predictors of TNFi discontinuation
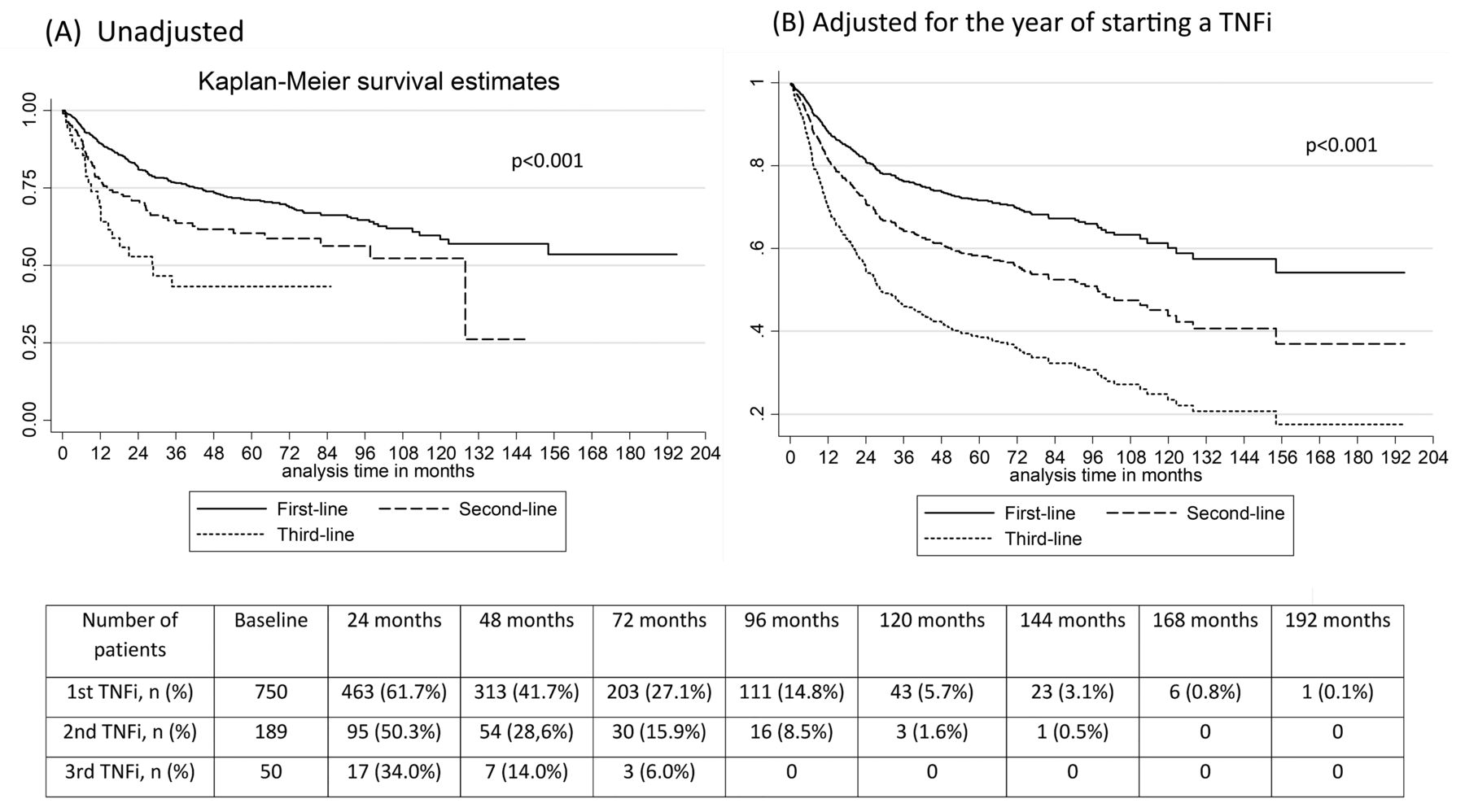
The overall mean TNFi retention for this PsA population was 48.9 ± 40.8 months (min: 0.4; max: 195.0) for treatment with the first TNFi, contrasting with a mean followup of 68.9 ± 45.0 months and corresponding to an exposure of 3063.4 person-years. TNFi retention decreased significantly to 35.5 ± 33.1 months (min: 0.0; max: 146.6) for the second TNFi (p < 0.001) and to 22.7 ± 22.9 months (min: 0.9; max: 85.1) for the third TNFi (p < 0.001; Figure 2). The unadjusted and adjusted survival rates were statistically different between TNFi prescribed as first-line therapy (Supplementary Figure 1, available with the online version of this article), although several baseline features were also distinct among TNFi (Supplementary Table 1).
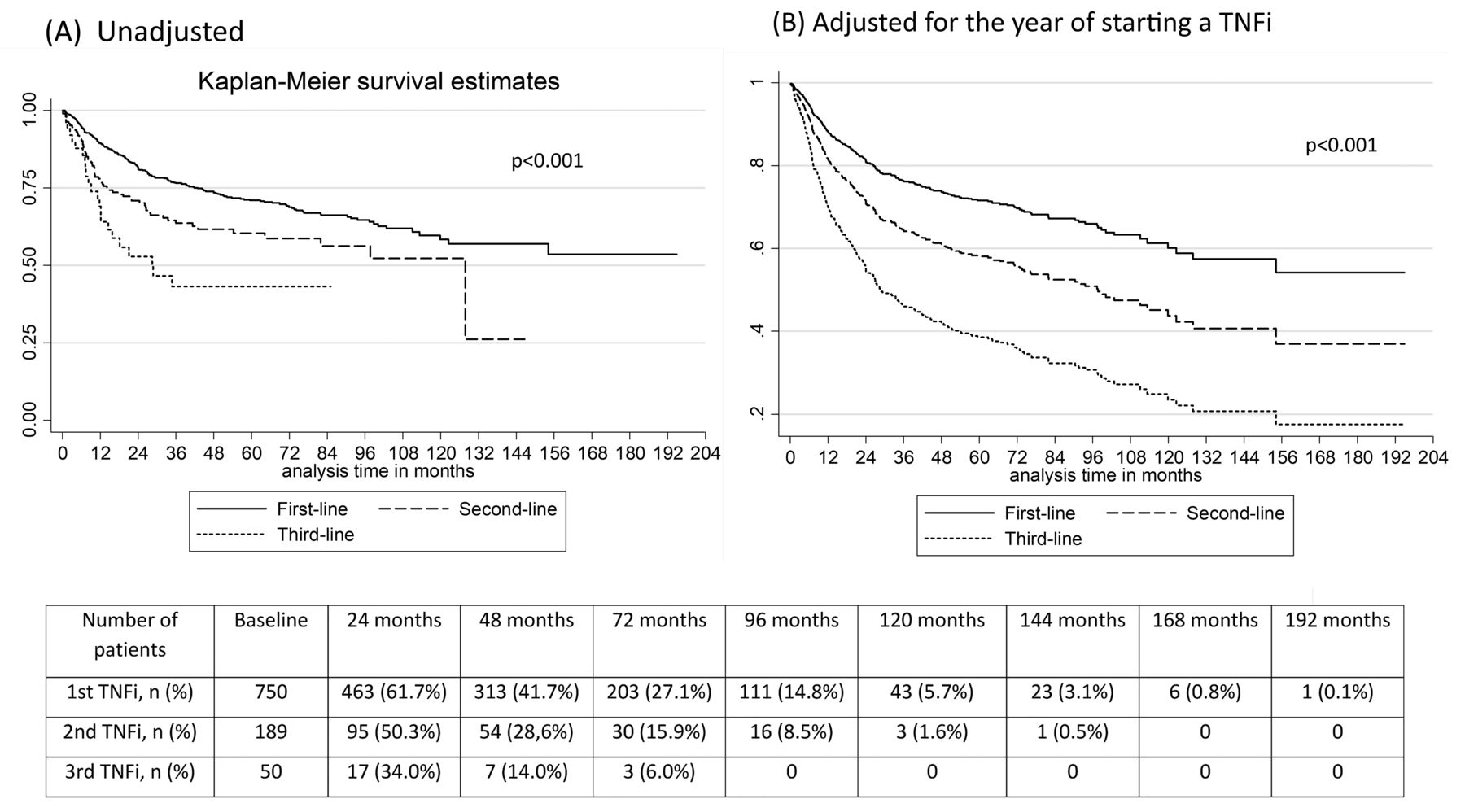
Survival estimates unadjusted (A) and adjusted (B) for the year of starting a tumor necrosis factor inhibitor (TNFi) drug retention, in patients with psoriatic arthritis registered at Reuma.pt and treated with TNFi prescribed as first, second, and third therapeutic lines. P = significance of survival curves of the first TNFi in comparison with the second and third TNFi. TNFi: tumor necrosis factor inhibitor.
From the initial 750 included patients treated with a first TNFi, 35.9% (269) discontinued this therapy primarily because of ineffectiveness (53.9%), whereas adverse events were the indication for discontinuation in 21.9% of patients. The time until discontinuation due to loss of response was 30.6 ± 29.0 months. There were no differences in the proportion of patients discontinuing treatment for each indication when comparing first-, second-, and third-line TNFi (Figure 1). Discontinuations due to inefficacy were mainly caused by secondary failures for the first, second, and third TNFi. We did not observe significant differences in survival for the second TNFi depending on the indication (ineffectiveness vs adverse events) for switching (Supplementary Figure 2, available with the online version of this article). The majority of those who discontinued a first, second, or third TNFi switched to another TNFi, whereas the remaining withdrew from TNFi therapy (Figure 1).
Predictors of discontinuation for the first TNFi were determined using a Cox model (n = 340 observations; Table 2). At baseline, in the univariate analysis, the group that discontinued their first TNFi had a higher proportion of females; higher levels of disease activity as measured by swollen and tender joints, ESR, DAS28-4vESR, and DAPSA; worse functional status (HAQ-DI); and more frequent concomitant corticosteroids (Table 1). Indeed, being female increased the risk of discontinuation of the first TNFi 2.1-fold (HR 2.1, p = 0.003). In addition, each unit increase in DAS28-4vESR at baseline raised the risk of discontinuation by 18% (HR 1.18, p = 0.039). Finally, treatment with IFX as opposed to ETN doubled the risk of discontinuation of the first TNFi therapy (HR 2.0, p = 0.015; global p = 0.036; Table 2). We did not find any influence of HAQ-DI at baseline and of concomitant therapy with csDMARD as a group or with MTX alone on first TNFi survival.
Predictors of discontinuation of a first-line tumor necrosis factor inhibitor (TNFi) using a Cox model of discontinuation considering 2 categories: continued versus discontinued.
Predictors of a good EULAR response to a first-line tumor necrosis factor inhibitor (TNFi), at 3 and 6 months. Univariable and multivariable analysis.
When looking separately at predictors of discontinuation (n = 290 observations) due to ineffectiveness and due to adverse events (Supplementary Table 3, available with the online version of this article), female sex was associated with a 2.18-fold increased risk of discontinuation due to ineffectiveness [relative risk reduction (RRR) 2.18, p = 0.029] and a 3.02-fold increased risk of discontinuation due to adverse events (RRR 3.02, p = 0.027). Each increase of 1 unit in the DAS28-4vESR at baseline was associated with a 52% increase in the chance of discontinuation due to ineffectiveness (RRR 1.52, p = 0.002), but a similar increase was not noted for discontinuation due to adverse events. Of interest, an increase of 1 year in the year of starting the first TNFi decreased the multinomial log-odds of discontinuation due to ineffectiveness and adverse effects by 17% and 15%, respectively.
Baseline predictors of response to TNFi
Response rates and functional improvements for the first and second TNFi are shown in Figure 3. At 3 and 6 months, the EULAR, DAPSA remission, PsARC, and ASDAS responses rates were significantly inferior for the second TNFi compared to the first TNFi. The ∆HAQ-DI was also significantly inferior for the second TNFi at 3 and 6 months and ∆BASFI at 3 months. The study of predictors of response to the first TNFi at 3 months (n = 161) identified female sex to be associated with 64% lower odds of achieving a good EULAR response (OR 0.36, p = 0.005). Further, in this population, an increase of 1 unit in the HAQ-DI at baseline was associated with 56% lower odds of response (p = 0.007). Although not significant, concomitant corticosteroids were negatively associated with response (OR 0.51, p = 0.054). At 6 months (n = 101), obesity was additionally associated with 75% lower odds of achieving a good EULAR response (OR 0.25, p = 0.006), and an increase of 1 year in the year of starting the first TNFi raised the chance of response by 27% (OR 1.27, p = 0.006). In addition, a higher HAQ-DI at baseline remained a predictor of nonresponse at 6 months (OR 0.35, p = 0.021). Finally, we found that concomitant axial involvement and concomitant therapy with csDMARD or MTX alone had no effect on achievement of a good EULAR response to the first TNFi at 3 and 6 months (Table 3).

LUNDEX-corrected response rates and functional improvements at 3 and 6 months of tumor necrosis factor inhibitors (TNFi) prescribed as first and second therapeutic lines. * Comparison between first and second TNFi responses with p value < 0.05. EULAR: European League Against Rheumatism; DAPSA: Disease Activity Index for Psoriatic Arthritis; PsARC: Psoriatic Arthritis Response Criteria: MDA: minimal disease activity; ASDAS: Ankylosing Spondylitis Disease Activity Score; HAQ-DI: Health Assessment Questionnaire–Disability Index; BASFI: Bath Ankylosing Spondylitis Functional Index.
Sex influence on TNFi retention and response
To clarify the effect of sex on TNFi retention and response, we compared the baseline characteristics between female and male patients (Supplementary Table 2, available with the online version of this article). Females were significantly older, more often obese, more frequently exhibited peripheral symmetric polyarticular phenotype, and had a longer delay between diagnosis and the start of the first TNFi. Further, females had significantly higher pain and enthesitis scores but also exhibited more severe peripheral disease activity as assessed by objective measures of disease activity and more frequently required concomitant corticosteroids and csDMARD. The overall TNFi survival rates for females were significantly lower than those for males (Supplementary Figure 3). We found an interaction between sex and patients’ pain VAS; however, sex remained an independent predictor of discontinuation of a first-line TNFi. On the contrary, we did not identify any interaction between sex and the DAS28-4vESR in the discontinuation prediction models (data not shown). In line with these results, females experienced lower response rates as assessed by good EULAR response at 3 and 6 months and by ASDAS at 6 months (data not shown). Examination of the interactions between sex and obesity, and sex and phenotype revealed no effect modification on response.
DISCUSSION
The goal of PsA treatment is to ensure sustained remission or low disease activity, fostering the prevention of damage and the improvement or maintenance of function and quality of life for patients with PsA. To achieve this objective in a real-life setting, both effectiveness and persistence of the response are required. In addition, understanding the effects of approved therapies after switching can help to guide clinicians in their PsA treatment decision algorithms. In this PsA population-based study of TNFi performance with a long followup (16 yrs), all subtypes of PsA were included with the objective of describing disease heterogeneity. Demographic characteristics of this population were similar to those reported by other European and US registries2,3,11,12,13,14. ETN was the most common TNFi used as a first-line therapy in Reuma.pt, similar to that reported by the British Society of Rheumatology Biologics Register (BSRBR)11 and the Norwegian DMARD (NOR-DMARD) register3, and ADA was the preferred second-line TNFi treatment option. This practice is distinct from that reported for the Danish register (DANBIO; (ADA > IFX > ETN) or the National Register for Biologic Treatment in Finland (ADA > ETN > IFX > GOL)12,15, with prescription preferences reflecting sequential regulatory approvals and national practices.
In the Reuma.pt registry, patients with PsA who switched to a second or third TNFi showed significantly lower drug retentions compared to those with a first-line TNFi. Further, significantly lower response rates assessed by a good EULAR, DAPSA remission, and PsARC responses for peripheral disease and by ASDAS response for axial involvement were observed, indicating that patients switching between TNFi do not typically regain the same level of disease activity control obtained with the first TNFi course. The observed worse effectiveness of the second (and third) TNFi in PsA and the inability to regain the same retention rate and response when switching to another TNFi emphasizes the absence of effective personalized treatment strategies in real-life practice and highlights the limitations of cycling between TNFi when aiming to achieve adequate longterm disease control in PsA.
At 1 year, the global survival rate (75%) for patients with a first TNFi was similar to that reported by the DANBIO, the NOR-DMARD, the Consortium of Rheumatology Researchers of North America, and the BSRBR3,11,12,13 but lower than that (87%) described by the Spanish registry (BIOBADASER), although all forms of chronic arthritis [rheumatoid arthritis (RA), PsA, AS, and others] were included in this report14. For the second TNFi, the survival rates at 1 year were consistently inferior to those for the first TNFi: Reuma.pt (60%), NOR-DMARD (57%)3, BSRBR (74%)11, and BIOBADASER (81%)14.
Ineffectiveness was the main reason for discontinuation of the first TNFi in about half of the patients in Reuma.pt, as described for other registries12,16. Despite the initial concerns regarding the safety of TNFi and other bDMARD, registries have demonstrated that adverse events less frequently cause treatment discontinuation or a switch than do treatment failures11,14. Our data indicated that about 20% of discontinuations of the first TNFi occurred because of adverse events, with similar percentages for discontinuation of the second and third TNFi. The variability of the results observed across registers may be dependent on register policies for the reporting of adverse events and prevention strategies in different countries11,14.
The response criteria [e.g., American College of Rheumatology, Clinical Disease Activity Index (CDAI), EULAR] used to assess the effectiveness have been different in the different studies13,15,17,18. In Reuma.pt, the overall response at 6 months to a first TNFi as measured by a good EULAR response was similar to that observed in other registries12,18. Response as measured by DAPSA remission or MDA, however, seems to be a difficult target to reach in clinical practice, as evidenced by the small percentage of patients achieving these outcomes in our register.
We identified female sex as an independent baseline predictor of discontinuation of first TNFi owing to both inefficacy and adverse events, a finding that is consistent with other reports2,12,13,19,20,21. Our results indicate that pain, but not DAS28-4vESR, contributes to modification of the effect of sex on drug retention of the first-line TNFi. Nevertheless, female sex remained an independent predictor of discontinuation. Further, female sex was associated with a lower chance of achieving a good EULAR response at 3 months. These results do not seem strictly dependent on patients’ reported outcomes, because significantly higher baseline objective measures of peripheral disease activity were observed in females and are not modified by obesity and disease phenotype. This supports sex-dependent patterns of response22 as described in our preliminary data from this cohort23. We also found a delay of 1 year between diagnosis and the start of the first TNFi in women compared to men, underscoring that despite having higher levels of disease activity, women receive delayed treatment and are at a higher risk of poor outcomes.
Data from Reuma.pt also reinforced the notion that high disease activity at baseline, as assessed by DAS28-4vESR, is a risk factor for TNFi discontinuation. This association has been previously identified based on the CDAI13 and the physician- and patient-reported global VAS12,19. Interestingly, this effect appears to be related to higher risk of discontinuation due to ineffectiveness but not due to adverse events.
Among different drugs prescribed as first-line TNFi, IFX was associated with shorter drug survival compared to ETN, as in the BIOBADASER reports, in which the findings were independent of IFX as a first- or second-line therapy14. These findings were also applicable to ADA. However, significantly different baseline features were identified in patients who received different TNFi, and the effect of patients starting TNFi in the early years of the biologics era cannot be discounted despite multivariate adjustments.
Higher baseline HAQ, but not high disease activity, was consistently an unfavorable factor for response at 3 and 6 months, indicating that baseline damage precludes optimal therapeutic responses and that consequently, early effective treatment is required to avoid joint damage and favor patients’ outcomes. Obesity was also identified as an independent predictor of a poor EULAR response at 6 months, supporting weight reduction as a co-adjuvant strategy to enable TNFi response in patients with PsA24 and other inflammatory joint diseases such as RA and other spondyloarthropathies25.
Data regarding concomitant medication, in particular MTX, have been contradictory, with some studies suggesting an improvement in survival with IFX and MTX18,26 and others reporting no effect of MTX on survival13,15,19,20,26,27. In our cohort, co-medication with csDMARD or with MTX alone did not affect the global TNFi retention. Further, as in other registries, concomitant treatment with csDMARD or with MTX alone did not lead to the response to a first-line TNFi15.
Moreover, we studied the effect of disease phenotype on first TNFi response and persistence. The presence of concomitant axial disease did not affect EULAR response, and we also failed to observe differences in TNFi survival according to phenotype. Previous studies also reported no differences in TNFi survival between poly- and oligoarticular subtypes20. In general, disease subtypes analysis may lack power to uncover differences among subgroups.
As an observational study based on registry data, the Exchange PsA study is susceptible to selection bias, even though all patients with PsA starting a bDMARD were recommended to be registered. Further, these data cannot be directly extrapolated to other populations. Owing to a lack of consensus regarding imputation methodologies for real-world databases and limitations of different methodologies, we chose to describe complete cases in this analysis. This study was also not powered to assess differences of persistence or response between the approved TNFi. Because of a limited number of patients who received a second (189) or third (50) TNFi, predictors of discontinuation were not determined for switchers, and response rates are not presented for third-line TNFi. In addition, besides obesity, other comorbidities were not consistently recorded. Based on the Exchange PsA results, additional information should be obtained from clinical trials and from registries to determine whether switching to new modes of action [e.g., interleukin (IL)-17, IL-12/23, Janus kinases, and phosphodiesterase E4 inhibitors] will yield additional benefits for treatment persistence and response.
The Exchange PsA study reinforces the concept that despite the remarkable benefits of TNFi for the management of patients with PsA, optimal longterm control of disease activity is difficult to achieve at the populational level. Further, results from this Reuma.pt PsA population validate much of the data about switching between TNFi from previous registers and provide new information on the effects of sex and PsA phenotype on the response and persistence of TNFi. Taken together, these results may inform development of more successful TNFi treatment strategies with attention to sex differences in the decision process and of trials assessing combined weight-reduction programs. In addition, given the lower drug survival after the switch to a second TNFi, understanding the effectiveness of new biologics and of the new inhibitors of intracellular signaling after the failure of a first-line TNFi will be of fundamental importance to support treatment decisions in clinical practice.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
The authors acknowledge Fernando Martins for his work at Reuma.pt. The authors kindly appreciate the contribution of all rheumatogists who included patients at Reuma.pt: Ana Roxo, António Vilar, Augusto Faustino, Carlos Vaz, Cristina Catita, Fernando Martins, Filipa Ramos, Filipe Araújo, Filipe Barcelos, Graça Sequeira, Herberto Jesus, Joaquim Polido Pereira, Jorge Garcia, José Alberto Pereira da Silva, José António Costa, José António Melo Gomes, José António Pereira da Silva, Luís Cunha Miranda, Mário Viana Queiroz, Margarida Cruz, Margarida Oliveira, Maura Couto, Patrícia Pinto, Paula Valente, Raquel Roque, Rui André, and Teresa Nóvoa.
Footnotes
The Exchange study was financially supported by an unrestricted grant from Novartis Produtos Farmacêuticos SA. Novartis had no influence on the data collection, statistical analysis, manuscript preparation, or decision to submit.
- Accepted for publication July 15, 2019.








{kind=link}
{kind=link}
{kind=link}