

Abstract
Objective. The assessment of the cardiovascular (CV) risk is recommended in patients with chronic inflammatory rheumatic diseases. The objectives of this study were to assess the CV risk profile in a cohort of patients with psoriatic arthritis (PsA), to determine the presence of subclinical cardiovascular disease by carotid ultrasound (US), and to study the association of CV disease to PsA characteristics.
Methods. This was a cross-sectional multicentric descriptive study. The clinical CV risk was calculated with Systematic Coronary Risk Evaluation (SCORE) charts. Common carotid US was conducted to evaluate the carotid wall intima-media thickness and the presence of atheroma plaques. Patients were reclassified upon US results. Multivariate analyses were performed to identify associations of US carotid abnormalities with the classical CV risk factors and PsA characteristics.
Results. The study included 176 patients with PsA. The SCORE-estimated CV risk was intermediate in 65.3% of the patients. In the US study, 32% of the patients had abnormalities, and 30.8% of the patients were upgraded and reclassified as very high risk owing to the presence of atheroma. Subclinical CV disease was associated with age and dyslipidemia but not with other risk factors. It was associated with axial disease in the subgroup with intermediate risk, and with C-reactive protein levels in patients with high risk.
Conclusion. Many patients with PsA have clinical estimated intermediate or high risk of a fatal CV event. A carotid US study detects subclinical vascular disease and may be useful to depict the real risk. The presence of atheroma is only partially explained by the classic CV risk factors.
Psoriatic arthritis (PsA) is a chronic inflammatory disease characterized by synovial and entheseal inflammation and psoriasis. As in other chronic rheumatic inflammatory diseases, several cross-sectional and longitudinal studies have found high prevalence of classic cardiovascular (CV) risk factors and CV events and in general, an increased mortality for CV reasons in patients with PsA1,2,3,4,5,6,7.
The European League Against Rheumatism (EULAR) task force recommends the use of local guidelines for CV risk assessment and treatment of patients with inflammatory joint disorders8. The Systematic Coronary Risk Evaluation (SCORE) CV disease risk prediction model should be used if no national guideline is available9. The Fifth Joint Task Force on CV disease prevention in clinical practice recommends the use of the SCORE charts to assess the CV risk in the general population10, but EULAR recommends adapting the CV risk obtained from the SCORE by a 1.5 multiplication factor for patients with rheumatoid arthritis (RA)8. However, no such correcting factor has been proposed for patients with PsA to date. In addition to the classic risk factors, the CV risk may also rely on longer disease duration and higher inflammatory burden in patients with PsA, suggesting that the SCORE might also underestimate the real CV risk in these patients11.
Several studies have described the presence of subclinical atherosclerosis in patients with spondyloarthritis, mostly in ankylosing spondylitis (AS), but also in PsA12,13,14. An ultrasound (US) scan of the common carotid artery wall can identify areas of increased thickness and nonocclusive atherosclerotic plaques, which represent subclinical markers of CV disease15,16. It has been demonstrated that the common carotid intima-media thickness (CIMT) is significantly associated with higher risk for stroke, coronary heart disease, or a combination of these in the general population17,18. In patients with RA, the use of carotid US has been shown to improve the stratification of the CV risk19. In addition, in these patients a CIMT > 0.9 mm yielded a high predictive power for the development of CV events20. However, data comparing clinical CV risk stratification and US results in patients with PsA are scarce21.
The main objectives of the present study were to assess the clinical CV risk profile in a multicentric cohort of patients with PsA; to study the presence of subclinical CV disease by standardized common carotid US procedures; and to investigate whether any specific disease characteristic or CV risk factor was associated with the presence of carotid atheromatosis.
MATERIALS AND METHODS
We performed a multicentric, cross-sectional, descriptive study of patients with PsA, followed in rheumatology units in the southeast area of Spain. Patients were consecutively recruited and included if they were over 18 years, fulfilled ClASsification for Psoriatic ARthritis (CASPAR) criteria22, were actively followed up with at least 1 visit in the last year, and signed an informed consent form for entering the study and publishing the results. The study was approved by the Clinical Research Ethics Committee of the Hospital General Universitario de Elda (approval number RCV-APS-MC/26/02/2016).
Variables analyzed
Clinical characteristics, obtained from the medical records, were age; sex; presence of psoriasis ever; psoriasis and arthritis duration at the time of the study; PsA disease pattern (axial, peripheral, or both – axial disease was defined clinically considering the presence of inflammatory-type back pain and/or substantial impairment of spinal mobility plus radiographic criteria); and in the last 5 years, therapy with nonsteroidal antiinflammatory drugs, disease-modifying antirheumatic drugs (DMARD), biological therapies, or other immunosuppressants. The median C-reactive protein (CRP) levels of the last 5 years were calculated, except in the few patients with a shorter disease duration, in which all CRP determinations since the diagnosis were included.
Recorded in the study visit were the presence of classic CV risk factors, including body mass index (BMI), hypertension (HTN), dyslipidemia, smoking history, diabetes mellitus (DM), and personal and familial CV events. Patients were considered nonsmokers if they had not smoked any cigarette in the previous 2 years. We also registered whether the patient had any specific therapy prescribed for dyslipidemia and hyperuricemia. For the SCORE classification, these were measured: current systolic and diastolic arterial blood pressure (best of 2 measures), weight, height, and abdominal perimeter. The lipid profile, which included total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C) and triglycerides (TG), and uric acid, were recorded if measured in blood samples within the last 3 months.
Then, the probability of fatal atherosclerotic CV events over a 10-year period was calculated using the SCORE chart calibrated for Spain (www.heartscore.org), following the European recommendations23. SCORE was not applicable in patients who had already had CV events, who must be considered at very high risk. It was not applicable to patients with DM, who have to be considered at high risk in the absence of target organ damage, and very high risk if target organ damage is present10.
US study
All the patients underwent a bilateral common carotid US study. The measurements were performed by rheumatologists specifically trained in the vascular US technique; a short consensus period was held ahead of the start of the study. Following the Mannheim consensus24, an all-length cross-sectional plus longitudinal scan of both common carotids was made, including carotid bulb and the origin of external and internal carotids when possible. The CIMT was measured manually, calculating the mean of 3 different measures taken in an area of 1 cm, located 1 cm caudally to the carotid bulb. Both the average CIMT and the presence of atheroma plaques in the walls or in the bulb were assessed in the right and left common carotids.
Plaques were defined, according to the Mannheim consensus, as focal structures encroaching into the arterial lumen of at least 0.5 mm or 50% of the surrounding CIMT value, or a thickness > 1.5 mm as measured from the intima-lumen interface to the media-adventitia interface24. Then, the patient risk was reassessed upon US findings. Thus, if plaques were detected, the patient’s risk was upgraded to very high. The patients with a CIMT > 0.9 mm who had other CV risk factors were also upgraded to the very high risk group. The US results of the patients with an already clinically estimated very high risk were irrelevant regarding risk upgrade and were not considered for the analyses.
Statistical analysis
As in a previous pilot study25, we identified plaque criteria in 26.5% of the patients with PsA, and using this as the expected frequency of plaque, the estimated sample size was 186 patients, for a CI of 95% and a precision of 3%. Descriptive data are shown as percentages or mean ± SD. The characteristics of the patients with plaques were compared to those without plaques by means of univariate analyses; differences between qualitative variables were assessed using Fisher’s exact test and the chi-square test, and quantitative variables using Student t test. For the CIMT associations, the Student t test was applied to analyze differences between means, and Pearson’s correlation coefficient was used for the analysis of continuous variables. The association between the presence of atheroma plaques in the US (independent variable) and PsA-related characteristics was analyzed using multivariable logistic regression, to adjust for classic CV risk factors. Two different models were used. The first considered the presence of plaques according to the Mannheim consensus24, and the second considered “carotid abnormality” as either plaques or a mean CIMT > 0.9 mm. We also estimated receiver-operating characteristic (ROC) curves to evaluate the ability of different variables to predict the presence of plaque. Statistical significance was established as p < 0.05. Data were analyzed with the statistical software SPSS V15.
RESULTS
Clinical characteristics
A total of 176 patients were included. The average age was 55.2 years (SD 11.8), with 16 patients under 40 years old (mean 34.1, SD 3.9). An exclusively peripheral form of PsA was present in 70.5%. Almost all the patients had psoriasis (95.5%), and the rest had a first-degree relative with psoriasis. Demographic and clinical characteristics of the sample are shown in Table 1.
Demographic and clinical characteristics of the patients with PsA included in the study (n = 176).
The frequency of the estimated clinical CV risk of the patients with PsA according to SCORE was low (SCORE < 1) 5.7%; intermediate (SCORE 1–4) 65.3%; high (SCORE 5–9) 12.5%; and very high (SCORE ≥ 10) 1.1%. There were 27 patients with DM, and 4 of them had had previous CV events. These patients were assigned to the groups of high or very high risk, depending on the presence of organ damage or CV events. The final clinical risk classification was low, 10 patients (5.7%); intermediate, 115 patients (65.3%); high, 44 patients (25%); and very high, 7 patients (4%). Among the very high risk patients, 4 had had previous CV events, 2 were very high upon SCORE, and 1 had DM with organ damage.
Ultrasound results
Atheroma plaques (Mannheim criteria) were found in 46 patients (26.3%). Also, 10 additional patients had an average CIMT > 0.9 mm and were considered very high risk because of the presence of other classic CV risk factors19. US results are shown in Table 2.
Ultrasound results of the patients with PsA who were evaluated (n = 176).
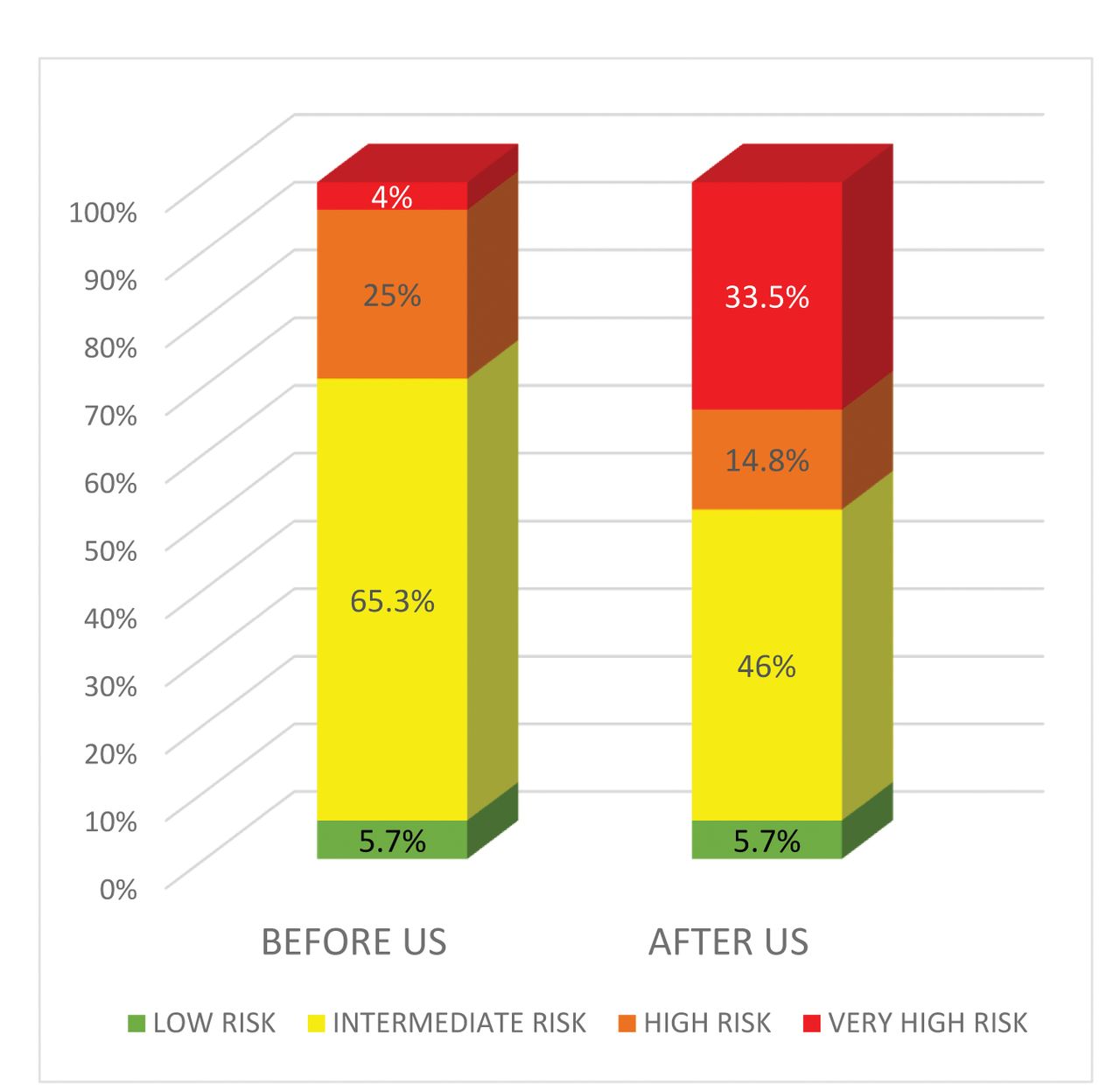
Fifty-three patients (30.8%) were upgraded because of the US results. No patient in the clinical low-risk group showed plaques. In the intermediate-risk group, 33 patients (18.8%) had US abnormalities. In the high-risk group, 20 patients (11.4%) had US abnormalities. Eventually, the classifications based upon the results of the US study were low risk, 10 patients (5.7%); intermediate risk, 81 patients (46%); high risk, 26 patients (14.8%); and very high risk, 59 patients (33.5%). CV risk stratification before and after the US study is shown in Figure 1.

Cardiovascular risk stratification before and after US study. CV: cardiovascular; US: ultrasound.
Univariate analysis
The patients with plaques were older [60.6 (SD 9.9) vs 56.6 (SD 11.7) years; p < 0.001] and showed a tendency to longer cutaneous disease. No differences were observed for sex, PsA disease type, CRP levels, joint disease duration, or treatments.
Patients with plaques had diagnosed dyslipidemia more frequently (43.5% vs 21.7%; OR 2.78, 95% CI 1.4–5.7; p = 0.007). Patients with carotid US abnormalities had HTN more frequently (39.3% vs 23.5%; OR 2.10, 95% CI 1.1–4.2; p = 0.048); higher urate levels (5.4, SD 1.5 vs 4.9, SD 1.5; p = 0.049); and had 3 or more concurrent classic CV risk factors more frequently (30.2% vs 10.2%; OR 2.39, 95% CI 1.20–4.89; p = 0.017). No differences were detected between groups for smoking, DM, BMI, TC, LDL-C, HDL-C, or TG levels.
In the intermediate group, 32 patients (28.1%) had plaque or a CIMT > 0.9 mm. No correlation was found between the median CRP levels and CIMT.
Multivariate analysis
In the multivariate model, the presence of plaques was associated only with age (OR 1.08, 95% CI 1.03–1.13; p < 0.001) and dyslipidemia (OR 2.78, 95% CI 1.05–7.33; p = 0.039). No associations between plaques and disease features were identified. An association close to the edge of significance was found for duration of cutaneous disease (OR 1.003, 95% CI 1.000–1.006; p = 0.042). Uric acid levels performed moderately for the presence of carotid US abnormalities; the area under the ROC curve was 0.63 (95% CI 0.53–0.74; Figure 2). No other disease characteristics or classic CV risk factors were associated with the presence of plaques. We performed a model for the coexistence of 2 or more classic CV risk factors and the presence of plaques, and the area under the ROC curve was 0.73 (95% CI 0.62–0.83; Figure 2).
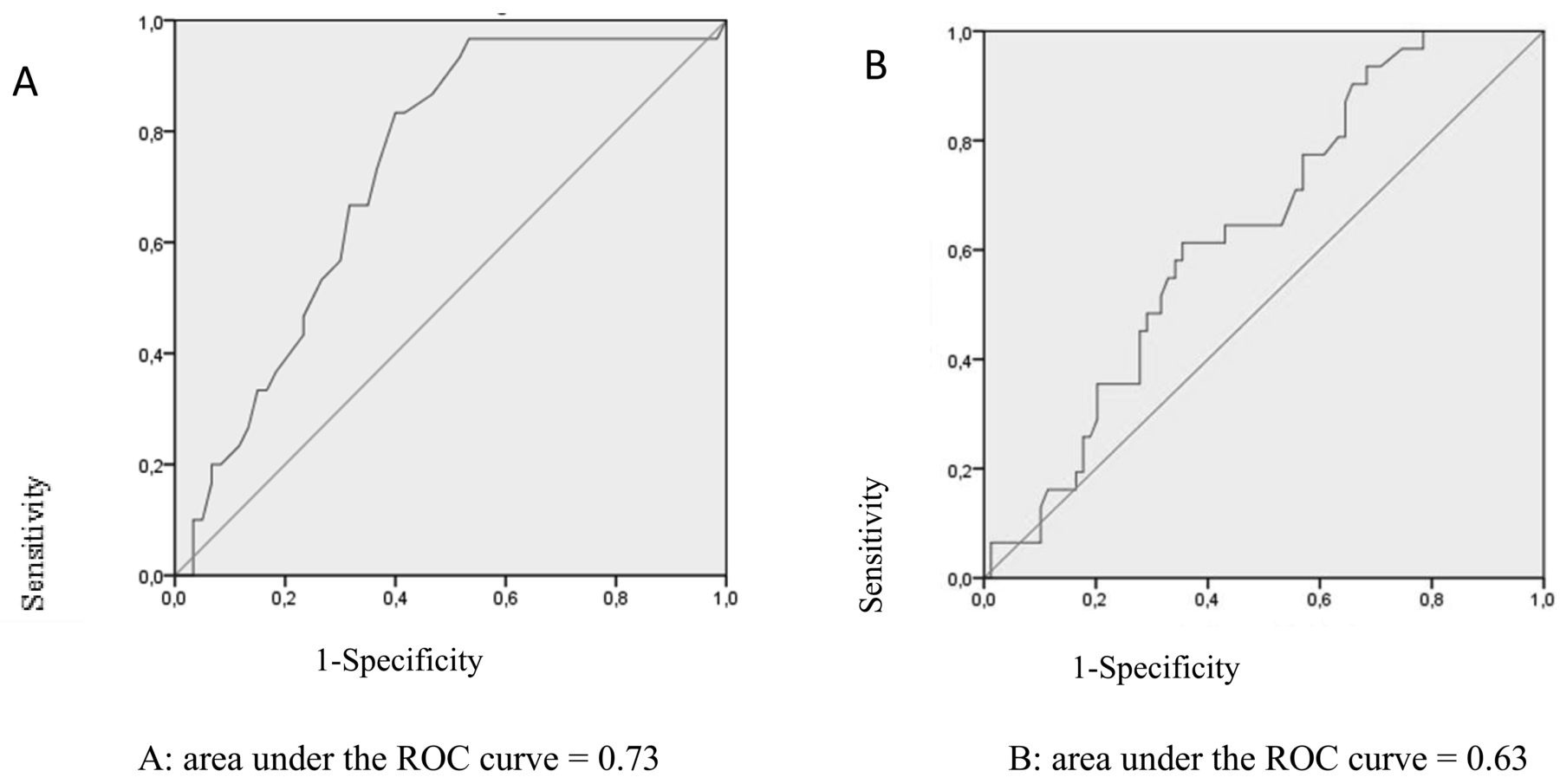
ROC curve for the ability of 2 or more classic CV risk factors to predict the presence of carotid plaques in the whole sample (A), and for the ability of uricemia to predict the presence of carotid US abnormalities in patients with clinical intermediate and high CV risk (B). ROC: receiver-operating characteristic; US: ultrasound; CV: cardiovascular.
In the patients with clinical intermediate risk, the presence of axial disease was associated with carotid abnormalities (OR 4.43, 95% CI 1.15–17.07; p = 0.031). Axial disease (OR 7.05, 95% CI 1.39–35.68; p = 0.018) and higher uricemia (OR 2.05, 95% CI 1.14–3.69; p = 0.016) were associated with being upgraded in the US study.
In the patients with clinical high risk, higher median CRP was associated with being upgraded in the US study (OR 23.18, 95% CI 2.02–266.66; p = 0.012). The patients receiving anti-tumor necrosis factor (TNF)–α therapies had lower probability of being upgraded in the US study, compared with the patients taking only DMARD (OR 0.03, 95% CI 0.001–0.687; p = 0.028).
DISCUSSION
We report the results of a series of patients with PsA and a thorough evaluation regarding CV risk factors and clinical and US estimates of CV disease. The presence of classic CV risk factors was considerable, similar to other series and prospective cohorts26,27,28,29,30,31. Because some prospective cohorts have shown that patients with PsA have more commonly classic CV risk factors and metabolic syndrome than patients with other inflammatory arthritides28, the assessment of the classic, modifiable CV risk factors should be encouraged in all patients with PsA.
EULAR recommends assessing the CV risk of patients with chronic rheumatic inflammatory diseases. It also recommends adapting the CV risk obtained from the SCORE by a 1.5 multiplication factor for patients with RA, because the clinical CV risk prediction tools do not reveal the effect of the inflammatory burden on the global CV risk8,32. There are no similar recommendations for the management of PsA so far. Nevertheless, the risk for CV diseases and mortality in PsA is also known to be increased31,33,34,35,36,37,38. In a recently published metaanalysis of population-based cohorts or case-control studies, the risk for myocardial infarction (MI) was significantly increased in PsA as well as in RA or gout33; the risk for MI was only attenuated when adjusting for traditional risk factors and remained significantly increased. These results suggest that traditional CV risk factors are not responsible for the total number of CV events observed in these patients.
In Europe, SCORE charts are usually recommended to assess the CV risk in the general population10. According to this tool, most patients in our series had a clinical estimated intermediate CV risk level. Nevertheless, SCORE has limitations in patients under 40 years old or with DM. In our series there were 16 young patients; all but 3 of them were considered to have a clinical intermediate CV risk (due to high cholesterol levels, smoking, or high blood pressure), and the US study revealed the presence of plaques in 1 case (a 29-year-old male). There was a young woman with DM who was considered high risk and the remaining 2 patients had low risk. SCORE limitations notwithstanding, it seems advisable that CV risk estimation should be conducted in all patients with PsA, regardless of their age. The carotid US reveals itself as an economical, reliable, and reproducible test to improve clinical risk estimation tools. The majority of abnormalities in the US scan were found in the intermediate group. Among the patients with intermediate or high CV risk, the US study revealed pathologic findings in 32% of the cases. These results suggest that the patients with a clinical intermediate or high risk would benefit the most from research for subclinical atheromatosis. In our series, the CV risk was upgraded because of the presence of subclinical atheromatosis in a substantial proportion of patients, resulting in an increase in the very high risk group.
Compared to other series of patients with PsA, we found a higher prevalence of subclinical CV disease14,39,40. In addition to our previous pilot work25, we have found only 1 study evaluating the CV risk in patients with PsA by both clinical tools and carotid US21. In that study, the Framingham Risk Score was applied in patients with psoriasis and PsA who then underwent carotid ultrasound. The Framingham score correlated only moderately with the presence of plaque and explained only 19% of the variability in the CIMT.
In patients with RA, not only the plaques but also the CIMT > 0.9 mm have shown a high predictive power for the development of CV events20. Along the same lines, a series of RA Spanish patients without CV events were assessed by SCORE, REGICOR, modified SCORE, and modified REGICOR according to the EULAR recommendations. Carotid US was performed, and CIMT > 0.9 mm and/or carotid plaques were used as the gold standard test for severe subclinical atherosclerosis. Both modified charts failed to identify 88% and 91% of US-positive patients32. According to the previous studies, a thinner CIMT could also imply a higher risk for future CV events in PsA. For the purpose of our study, the patients with a CIMT > 0.9 mm who had other CV risk factors were upgraded to very high risk and were placed on a CV risk prevention program along with the rest of the patients who had plaques. Globally, in our series of patients with PsA, SCORE stratification tables proved to be insufficient to reveal the real CV risk because US detected subclinical abnormalities in 32% of them. Eventually, 48.3% of the patients had a final high or very high CV risk. However, we need to regard these results cautiously because we do not yet know the predictive value of CIMT > 0.9 mm for CV events in PsA. In our study, the presence of plaque was associated as expected with age and dyslipidemia. Upgrade due to plaques was associated with higher uricemia only in the intermediate risk group. The reason could be an insufficient sample size, because hyperuricemia has been previously associated with carotid plaques in a large multi-center study41. No associations with other classic CV risk factors were found. In addition, there was a very young man who had plaque in the US test. These findings suggest that there must be other factors influencing the real risk, such as the inflammatory burden, in patients with PsA.
It still remains a challenge today to accurately evaluate the role of the inflammatory burden in atheromatosis. PsA is a phenotypically very variable disease and we are still lacking a consensual validated global activity index. Further, the different available disease activity indices such as the Disease Activity Index for Psoriatic Arthritis indicate the state at a particular moment and not the accumulated inflammatory burden. As a way to estimate the inflammatory burden, we included the CRP determinations of the preceding years and calculated the median CRP to avoid the bias that average CRP could cause by drastic increases during infections. On the other hand, an indirect way of estimating the inflammatory burden of the disease was analyzing the duration of skin and joint disease and the therapies used. Previous works analyzing the association of inflammation with atheromatosis in patients with PsA have yielded different results. A recent study found a mild correlation between the CIMT and the disease duration in patients with PsA, and the CIMT and CRP, although there were no differences between the CIMT in PsA versus healthy controls39. Some authors did not find an association of plaques with inflammatory markers or disease duration14,40. On the contrary, higher erythrocyte sedimentation rates but not higher CRP were associated with more severe atherosclerosis in a Canadian descriptive study42. In our series, the upgrade due to plaques was associated with CRP levels only in the high-risk group. This may occur because CRP, as a unique outcome, is imprecise to express the global inflammatory burden, or because the inflammatory burden might become more relevant for atheromatosis in presence of a certain number of classic CV risk factors. In our sample, the majority of the patients had a medium-term or longterm cutaneous and/or joint disease at the moment of the study. The presence of plaques showed a tendency to longer skin disease duration, but not to longer arthritis; this could be influenced by the sample size. We did not find other associations with disease characteristics, except for axial disease in the intermediate group. The reason could be an insufficient sample size, because in patients with AS a greater IMT than in controls has been described, after adjustment for traditional CV risk factors12. Interestingly, in our series the patients in the high-risk group taking anti–TNF-α therapy had lower probability of plaques, suggesting a potential protective role of these treatments.
The main limitation of our study is its cross-sectional design, making it impossible to draw conclusions about the precise role of US in predicting the real risk for CV events in patients with PsA. On the other hand, the sample size may have been insufficient to detect differences regarding disease type and duration or therapies. Another weakness is that we lack specific articular and cutaneous disease activity indices, and also that the treatment duration was not considered. It is possible that these variables might have yielded different results. Larger cohort studies are needed to better define the relationship between the characteristics of patients with PsA and subclinical CV disease, and prospective studies should be conducted to analyze the role of subclinical CV disease in the development of CV events in this population.
Our results are relevant for clinical practice because there is a high prevalence of traditional CV risk factors among patients with PsA, and hence CV risk should be assessed in all these patients. However, SCORE charts may underestimate the real CV risk, and thus we could be missing the CV risk in a considerable proportion of patients with PsA. A common carotid US scan would be advisable in patients in the intermediate and high-risk groups, especially if dyslipidemia or hyperuricemia are present, or there is axial involvement or a longstanding skin disease.
Footnotes
Supported by institutional funding from the Sociedad Valenciana de Reumatología.
- Accepted for publication May 23, 2019.








{kind=link}
{kind=link}