

Abstract
Objective. Although prednisolone (PSL) and immunosuppressants are key drugs for Takayasu arteritis (TA) treatment, there is limited evidence on the optimal PSL dose. The aim of this study was to investigate the correlation between the initial PSL dose and relapse in TA.
Methods. We enrolled 105 patients with TA who satisfied the criteria of the Japanese Circulation Society and American College of Rheumatology from 1990 to 2015. The clinical characteristics and outcomes of patients with TA were retrospectively evaluated. The relapse-free period was assessed according to the difference in initial treatments.
Results. Relapse was observed in 57 (59.4%) of 96 patients treated with immunosuppressive therapy at diagnosis during a median followup of 56 months. Male sex and younger age of onset were significantly associated with relapse. Although ≤ 30 mg/day PSL monotherapy was preferably prescribed for patients with lower inflammatory markers, compared with > 30 mg/day (87.2% vs 52.6%), a significantly higher relapse rate was observed in the ≤ 30 mg/day group (HR 1.78; p = 0.047). Further, the relapse-free period was longer in patients treated with ≥ 50 mg/day PSL compared with those treated with ≤ 40 mg/day PSL. Combination therapy improved the relapse-free period compared with PSL monotherapy in the short term. The initial PSL dose was not associated with adverse events.
Conclusion. A higher dose of PSL was associated with a significant decrease in the relapse rate. The effect of combination therapy on relapse needs to be further investigated. Lower-dose PSL monotherapy is an undesirable strategy for remission induction in TA, despite low disease activity.
Takayasu arteritis (TA) is a form of large-vessel vasculitis (LVV), characterized by chronic granulomatous inflammation of the aorta and its major branches, resulting in stenosis, obstruction, dilatation, and aneurysm formation1. TA is sometimes complicated by other inflammatory disorders2,3,4,5. Although the precise etiology remains unclear, its association with HLA-B52, HLA-B67, and interleukin (IL)-12B has been demonstrated6. Further, immune cells including macrophages, T and B cells, and antiendothelial autoantibodies have been considered to play critical roles in its pathophysiology7.
Given its immunological nature, corticosteroids such as prednisolone (PSL) are the mainstay treatments for TA. However, patients frequently experience relapse when PSL is tapered8. The European League Against Rheumatism has recommended initiation of high-dose glucocorticoid (1 mg/kg/day) therapy for LVV9. In Japan, the Japanese Circulation Society (JCS) Joint Working Groups have advocated revised guidelines for vasculitis syndrome management, with 0.5–1.0 mg/kg/day PSL being the initial recommended dose10. Previously, the JCS Joint Working Groups had recommended an initial dose of 20–30 mg/day of PSL11. PSL monotherapy based on this dose was reported to be effective in about half of patients with TA12. In this way, the character of optimal initial treatment remains unresolved, because studies focusing on the optimal dose of PSL in TA are limited. Particularly, it remains unclear whether low doses of PSL monotherapy can be an option for TA.
We aimed to investigate the correlation between initial treatments and the relapse-free rate in TA.
MATERIALS AND METHODS
Patients
This study included 105 consecutive patients with TA who visited our department from January 1990 to December 2015. TA diagnosis was based on the criteria of the JCS Guideline for the Management of Vasculitis Syndrome11 and of the American College of Rheumatology13. Patient followup was conducted until April 2018.
Study design
Patients’ medical records were retrospectively assessed for the following information: age at onset, sex, duration until diagnosis, laboratory data at diagnosis [erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP)], vascular involvement, complications, medications, surgical history, followup duration, number of relapses, and period from diagnosis to relapse. Adverse events that were also evaluated included severe infection, bone fractures, osteoporosis, diabetes mellitus, dyslipidemia, cardiovascular diseases, hematological disorders, gastrointestinal (GI) bleeding, and death.
Affected vascular lesions were classified on the basis of angiographic findings14. Disease activity was determined according to US National Institutes of Health (NIH) criteria and included the following 4 components: systemic features, elevated inflammatory markers (ESR or CRP), features of vascular ischemia or inflammation, and typical angiographic features. Relapse was defined as clinical status deterioration satisfying new onset or worsening of at least 2 of 4 components15,16.
Mean dose reduction of PSL (mg/month) was defined as follows: (initial dose of PSL – dose at relapse or at the last reduction) divided by the duration until relapse or the last reduction, according to the previous report17.
We evaluated patients with TA, compared the differences in clinical findings between the relapse and nonrelapse groups, and analyzed the relapse-free rates between the groups classified according to PSL doses and immunosuppressive drug use as initial treatment. The study protocol complied with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Tohoku University Graduate School of Medicine (reference number: 10788). Patients’ written informed consent was not required because of the retrospective observational design of the study.
Statistical analysis
All statistical evaluations were performed using GraphPad Prism 7.03. Mann-Whitney U test or t test was used for continuous data, and chi-square or Fisher’s exact test was used for binary data. Survival and cumulative incidence curves were drawn using the Kaplan-Meier method, and the log-rank test was used to compare relapse-free survival rates between the groups. The mean PSL doses in each month were analyzed using 2-way ANOVA with Sidak’s multiple comparisons test. HR and 95% CI were calculated. P < 0.05 was considered statistically significant.
RESULTS
Baseline characteristics and relapse
Table 1 summarizes the clinical characteristics of patients with TA. Mean age at onset was 35.6 ± 16.9 years, and female sex was predominant (90.4%). Mean CRP and ESR levels were 4.1 ± 4.0 mg/dl and 58.9 ± 35.2 mm/h, respectively. Type V disease was the most frequent (n = 31, 29.5%), followed by type IIa and IIb diseases (n = 25, 23.8%, and n = 20, 19.0%, respectively). Eight patients had inflammatory bowel disease (7.6%). Ninety-six patients (91.4%) fulfilled the NIH criteria for active TA. Fifty-seven patients (59.4%) had relapse during a median of 56 months of followup, and median duration from initial treatments to relapse was 16.5 months. Most patients (n = 36, 63.2%) experienced relapse one time. Multiple relapses were observed as follows: 2 times, 14 patients (24.1%); 3 times, 4 patients (6.9%); and 4, 7, or 9 times, 1 patient (1.7%).
Baseline characteristics of 105 patients with Takayasu arteritis.
Treatment details
The treatment flowchart is shown in Appendix 1, and initial remission induction therapy for patients with active TA (n = 96) is summarized in Table 2. Of the 105 patients, 9 (8.6%) were not treated because of inactive disease status. Mean PSL dose was 38.9 ± 14.5 mg/day (0.72 ± 0.28 mg/kg/day) and mean reduction rate was 2.1 ± 3.3 mg/month. In particular, mean reduction rate of PSL from the initial dose to 30 mg/day, between 30 mg/day and 20 mg/day, and after tapering the dose to 20 mg/day was 3.2 ± 1.4 mg/week, 2.5 ± 0.9 mg/week, and 1.3 ± 1.0 mg/month, respectively. The initial PSL dose was 60 mg/day (1.1 ± 0.23 mg/kg/day) for 14 patients (14.6%), 50 mg/day (0.94 ± 0.15 mg/kg/day) for 13 patients (13.5%), 40 mg/day (0.81 ± 0.13 mg/kg/day) for 27 patients (28.1%), 30 mg/day (0.54 ± 0.10 mg/kg/day) for 21 patients (21.9%), 20 mg/day (0.38 ± 0.09 mg/kg/day) for 15 patients (15.6%), 10 mg/day (0.19 ± 0.05 mg/kg/day) for 3 patients (3.1%), and other doses (0.78 ± 0.23 mg/kg/day) for 3 patients (3.1%). Intravenous methylprednisolone pulse therapy was administered to only 7 patients (7.3%) who experienced relapse. Mean PSL dose at relapse and that required to induce remission was 10.0 ± 5.9 mg/day (0.18 ± 0.11 mg/kg/day) and 36.2 ± 11.1 mg/day (0.69 ± 0.21 mg/kg/day), respectively. Sixty-four patients (66.7%) received PSL monotherapy, whereas 32 (33.3%) received combination therapy with immunosuppressive drugs as initial therapy. The most commonly used immunosuppressant was methotrexate (MTX, n = 24, 75.0%), followed by mizoribine (MZR, n = 3, 9.4%), intravenous cyclophosphamide (IVCYC, n = 2, 6.3%), cyclosporine (CSA, n = 1, 3.1%), azathioprine (AZA, n = 1, 3.1%), and tacrolimus (TAC, n = 1, 3.1%). In the combination therapy group, 17 patients experienced relapse. For control of refractory disease, 7 patients treated with MTX switched to CSA (n = 6) or AZA (n = 1), those with MZR (n = 2) switched to CSA (n = 1) or AZA (n = 1), and 1 patient switched from CSA to MTX. The other patients continued to be treated with similar immunosuppressive drugs (MTX, n = 6; IVCYC, n = 1). Among 21 patients who experienced more than 2 relapses, 5 (23.8%) received combination therapy as initial treatment (MTX, n = 3; CSA, n = 1; MZR, n = 1).
Initial remission induction therapy for patients with active Takayasu arteritis.
Higher relapse rates in patients treated with ≤ 30 mg/day PSL
Although high-dose (1 mg/kg/day) PSL or its equivalent is generally accepted as effective for TA treatment16, it remains unclear whether TA patients with low inflammatory activity can be treated with low-dose PSL. In our cohort, the ≤ 30 mg/day PSL dose (n = 39) administered in patients with low inflammatory markers was compared with > 30 mg/day PSL (n = 57; Figure 1A; mean CRP levels 3.1 ± 3.2 vs 5.3 ± 4.3 mg/dl, respectively; p = 0.005). Combination therapy with immunosuppressants was significantly less common in patients treated with ≤ 30 mg/day PSL than in those treated with > 30 mg/day PSL (Figure 1B; 12.8% vs 47.4%; p = 0.0004). Of note, the Kaplan-Meier curve revealed that the relapse rate was significantly higher in the ≤ 30 mg/day PSL group than in the > 30 mg/day PSL group (Figure 1C; HR 1.78, 95% CI 1.01–3.06; p = 0.047). Median relapse-free duration was 21 months for the ≤ 30 mg/day PSL group and 84 months for the > 30 mg/day PSL group. The relapse-free rates in the ≤ 30- and > 30-mg/day PSL groups were 48.7% and 69.2% at 24 months and 34.6% and 51.7% at 60 months, respectively. To examine whether the initial CRP levels influenced relapse, we analyzed the relationship between frequency and CRP levels. The cumulative frequencies according to CRP levels were comparable between the relapse and nonrelapse groups (Figure 1D). Relapse rates at CRP levels of 0–2, 2–4, 4–8, and 8–20 mg/dl were 56.5%, 60.9%, 57.9%, and 47.1%, respectively. There was no statistical difference in the mean PSL doses at relapse between the ≤ 30 and > 30 mg/day PSL groups (Figure 1E; 8.7 ± 5.6 vs 11.6 ± 6.1 mg/dl; p = 0.068).
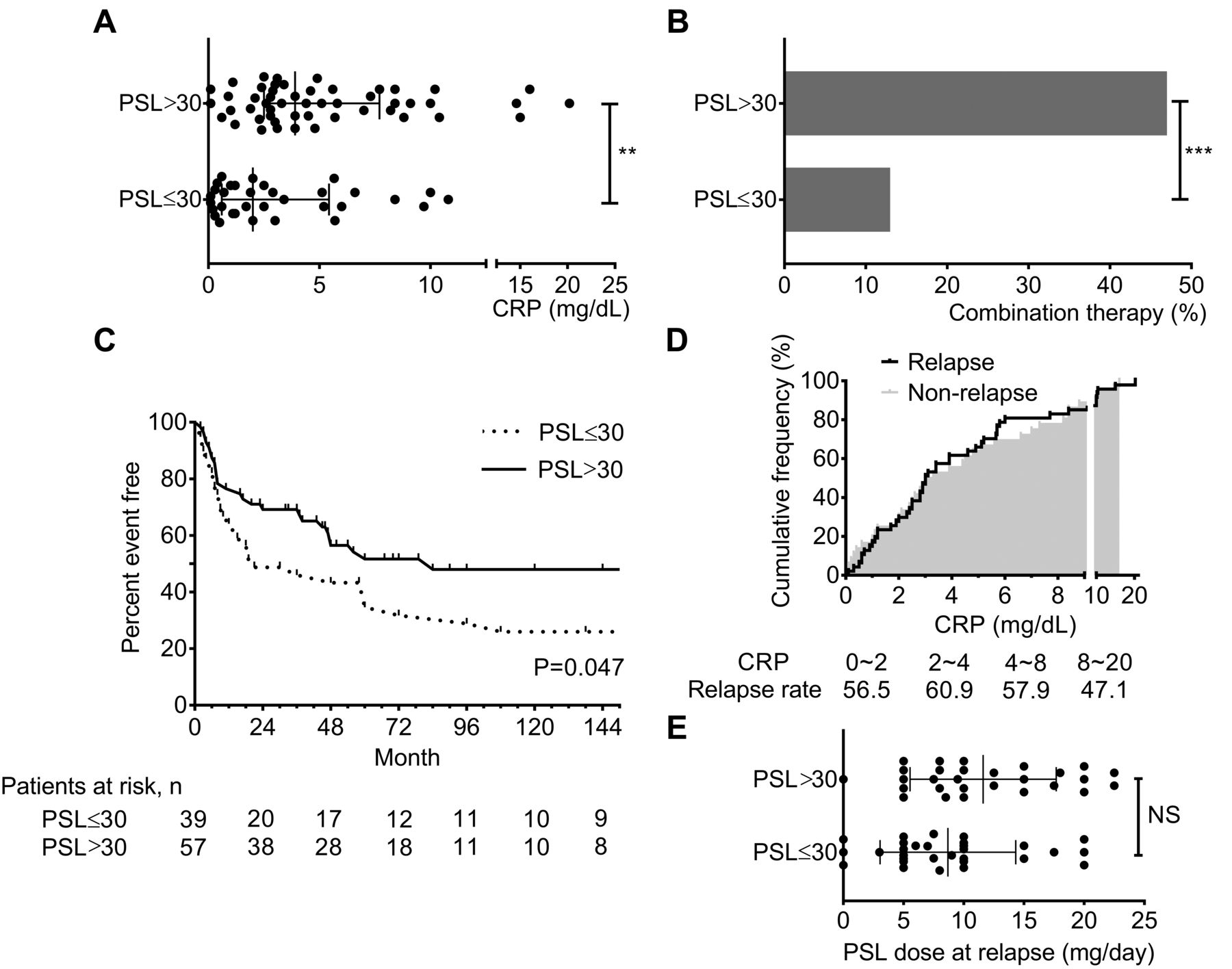
Higher relapse in patients treated with ≤ 30 mg/day PSL. A. CRP levels in patients treated with > 30 (n = 41) or ≤ 30 mg/day PSL (n = 33). B. Prevalence of combination therapy between the > 30 (n = 57) and ≤ 30 mg/day PSL groups (n = 39). C. Kaplan-Meier curves of time to relapse in the > 30 (n = 57) and ≤ 30 mg/day PSL groups (n = 39). D. The cumulative frequency of patients with relapse (n = 47) or nonrelapse (n = 36) according to the CRP levels (mg/dl). E. Doses of PSL (mg/day) at the time of relapse in the > 30 (n = 28) and ≤ 30 mg/day PSL groups (n = 30). Dots represent data for individuals; bars indicate mean ± SD. ** p < 0.01; *** p < 0.001. CRP: C-reactive protein; PSL: prednisolone; NS: not significant.
Delay in time to relapse with combination therapy
Previous analysis included heterogeneous patients receiving both PSL monotherapy and combination therapy. Hence, we evaluated the relapse-free rates in patients who were initially treated with PSL monotherapy (> 30 mg/day, n = 30; ≤ 30 mg/day, n = 34). A Kaplan-Meier curve similar to Figure 1C was observed, but it did not reach statistical significance (HR 1.66, 95% CI 0.87–3.16, p = 0.18; Figure 2A). Interestingly, improvement in the relapse-free period was observed in patients with a higher PSL dose (≥ 50 mg/day; Figure 2B). The relapse-free rates in 40, 50, and 60 mg/day PSL groups (n = 10, 9, and 8, respectively) were 66.7%, 77.8%, and 75.0% at 24 months and 44.4%, 51.9%, and 60.0% at 60 months, respectively.
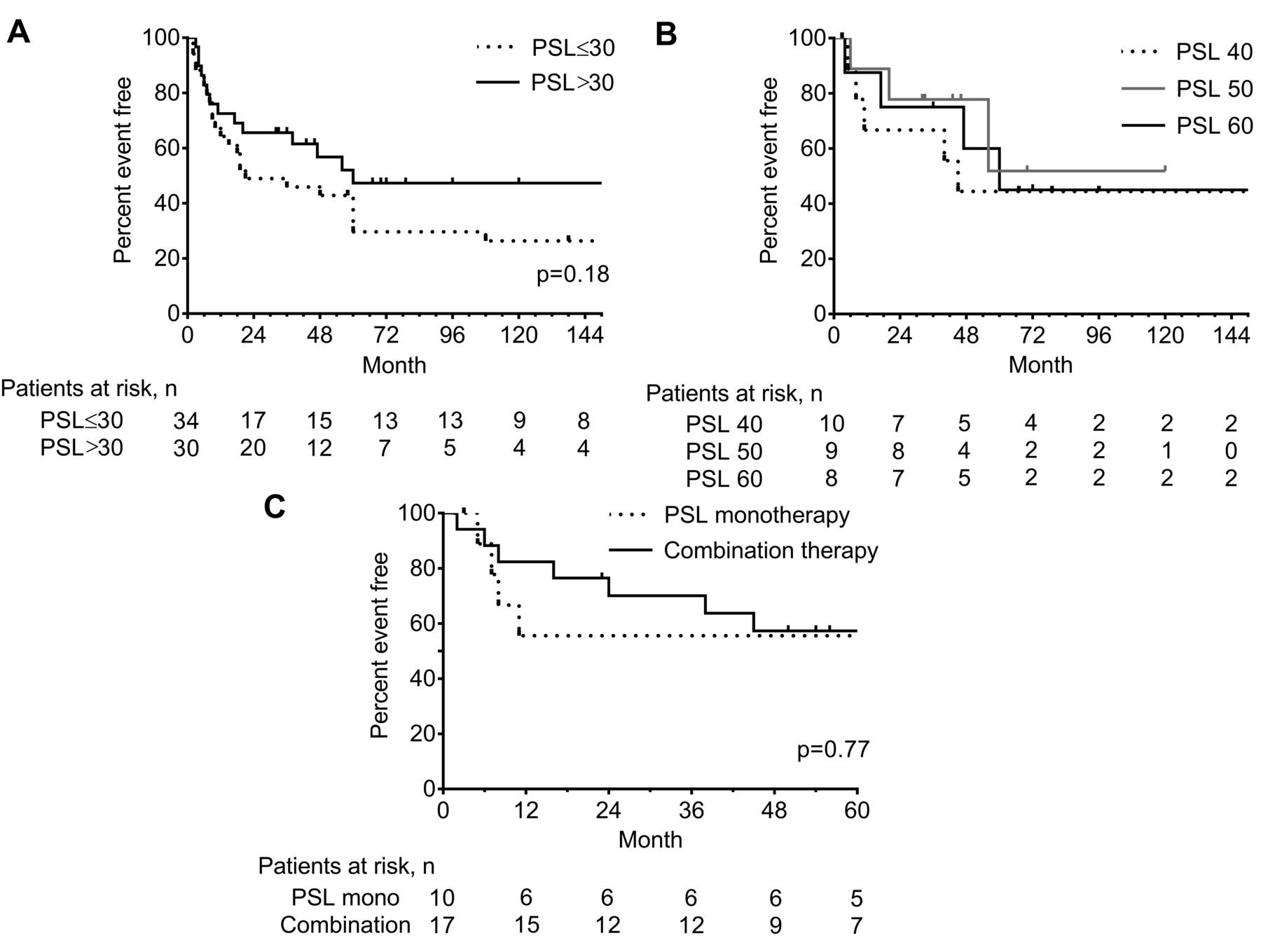
Delay in time to relapse with combination therapy. A. Kaplan-Meier curves showing the relapse-free rates in patients treated with > 30 (n = 30) and ≤ 30 mg/day PSL monotherapy (n = 34). B. Kaplan-Meier curves showing the relapse-free rates in patients treated with 40 (n = 10), 50 (n = 9), and 60 mg/day PSL monotherapy (n = 8). C. Kaplan-Meier curves showing the relapse-free rate in patients treated with PSL 40 mg/day with (n = 17) or without (n = 10) immunosuppressive drugs. PSL: prednisolone.
We assessed whether combination therapy improved the relapse-free period. Because the initial PSL dose was a strong determinant for relapse (Figure 2B), we selected patients with initial PSL dose of 40 mg/day and compared the relapse-free period between patients with PSL monotherapy (n = 10) and combination therapy (n = 17). The immunosuppressive drugs added were MTX (n = 14), TAC (n = 1), AZA (n = 1), and MZR (n = 1). Although statistical difference was not identified among these groups (HR 1.20, 95% CI 0.34–4.24; p = 0.77), the relapse-free rates with PSL monotherapy and combination therapy were 55.6% and 82.4% at 12 months, and 55.6% and 70.1% at 24 months, respectively (Figure 2C).
Comparison between the relapse and nonrelapse groups
We compared the differences in clinical variables between the relapse and nonrelapse groups. Several factors were found to be significantly different by univariate analysis, which included sex, age at onset, initial PSL dose, and mean reduction rate of PSL (Table 1 and Table 2). A significant amount of high-dose methylprednisolone pulse therapy was found in the relapse group (12.3% vs 0%; p = 0.039). Combination therapy was initially prescribed for 17 (29.8%) and 15 (38.5%) patients in the relapse and nonrelapse groups, respectively, which was not statistically different (p = 0.38). The apparent difference of immunosuppressants used was not observed between the 2 groups (Table 2).
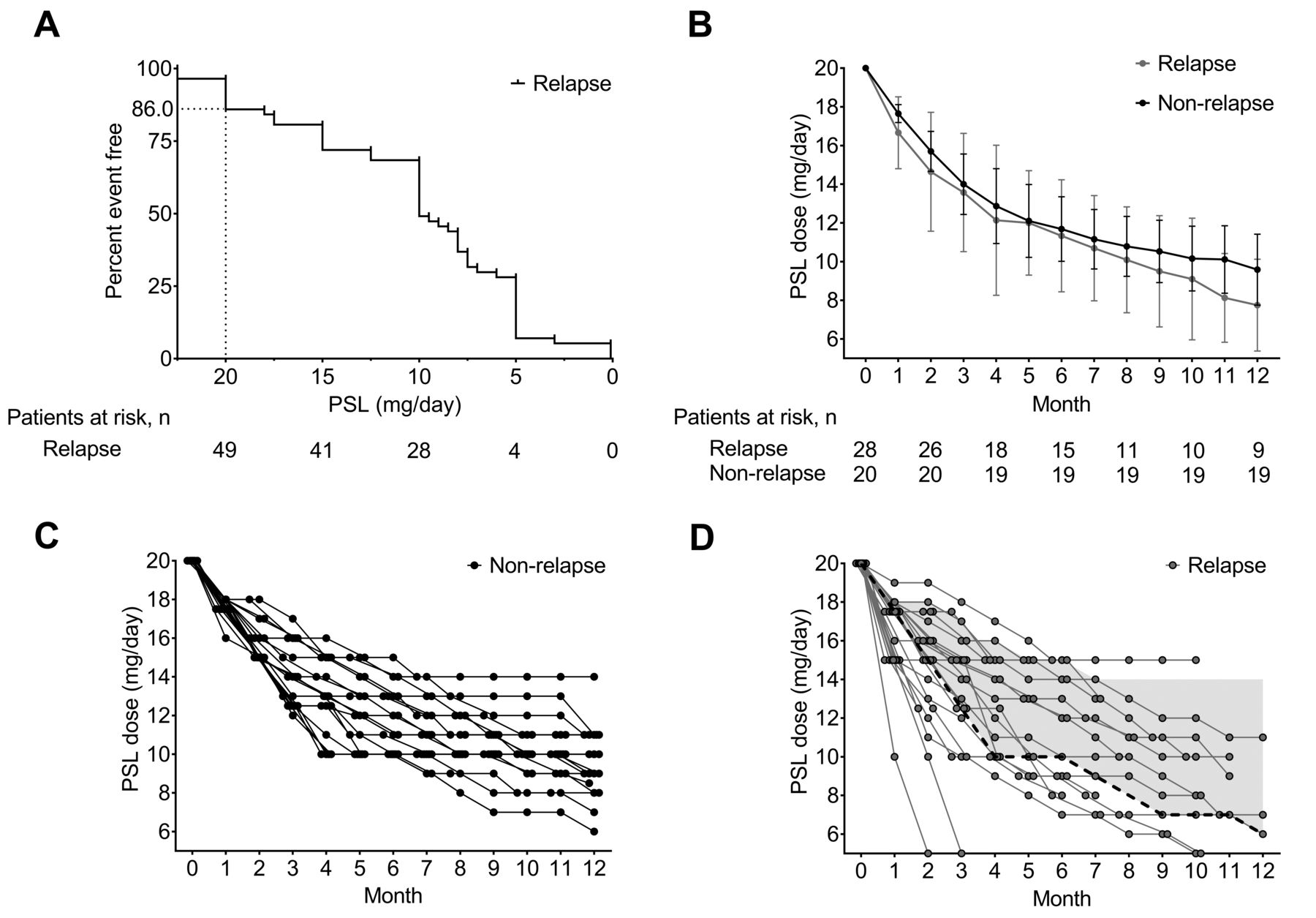
Given that the reduction rate of PSL is another important issue in TA treatment, we analyzed the reduction rate of PSL in the following 3 periods: until the PSL dose reached 30 mg/day, when the dose was between 30 and 20 mg/day, and when it was below 20 mg/day. The reduction rates until the PSL dose reached 30 mg/day, was between 30 and 20 mg/day, and was below 20 mg/day (relapse vs nonrelapse group) were as follows: 3.0 ± 1.1 versus 3.1 ± 0.9 mg/week, p = 0.52; 2.4 ± 1.0 versus 2.7 ± 0.9 mg/week, p = 0.27; and 1.7 ± 1.3 versus 0.8 ± 0.6 mg/month; p = 0.005, respectively (Table 2). However, the followup period until the final PSL reduction was longer in the nonrelapse group than in the relapse group. Thus, we next analyzed individual PSL doses below 20 mg/day because 86.0% of relapses occurred at the dose of PSL < 20 mg/day (Figure 3A). Mean PSL doses for the relapse and nonrelapse groups were indistinguishable (Figure 3B). However, individual PSL doses in the nonrelapse group were relatively close, and the fastest reduction rate was 2.5 mg/month until a PSL dose of 10 mg/day was reached, maintenance of 10 mg/day PSL for 2 months, and then tapering the dose by 1.0 mg/month (Figure 3C). A faster reduction rate of PSL than the method described above resulted in relapse, accounting for 53.6% of relapse (68.4% were > 30 mg/day of PSL and 88.9% were combination therapy; Figure 3D).
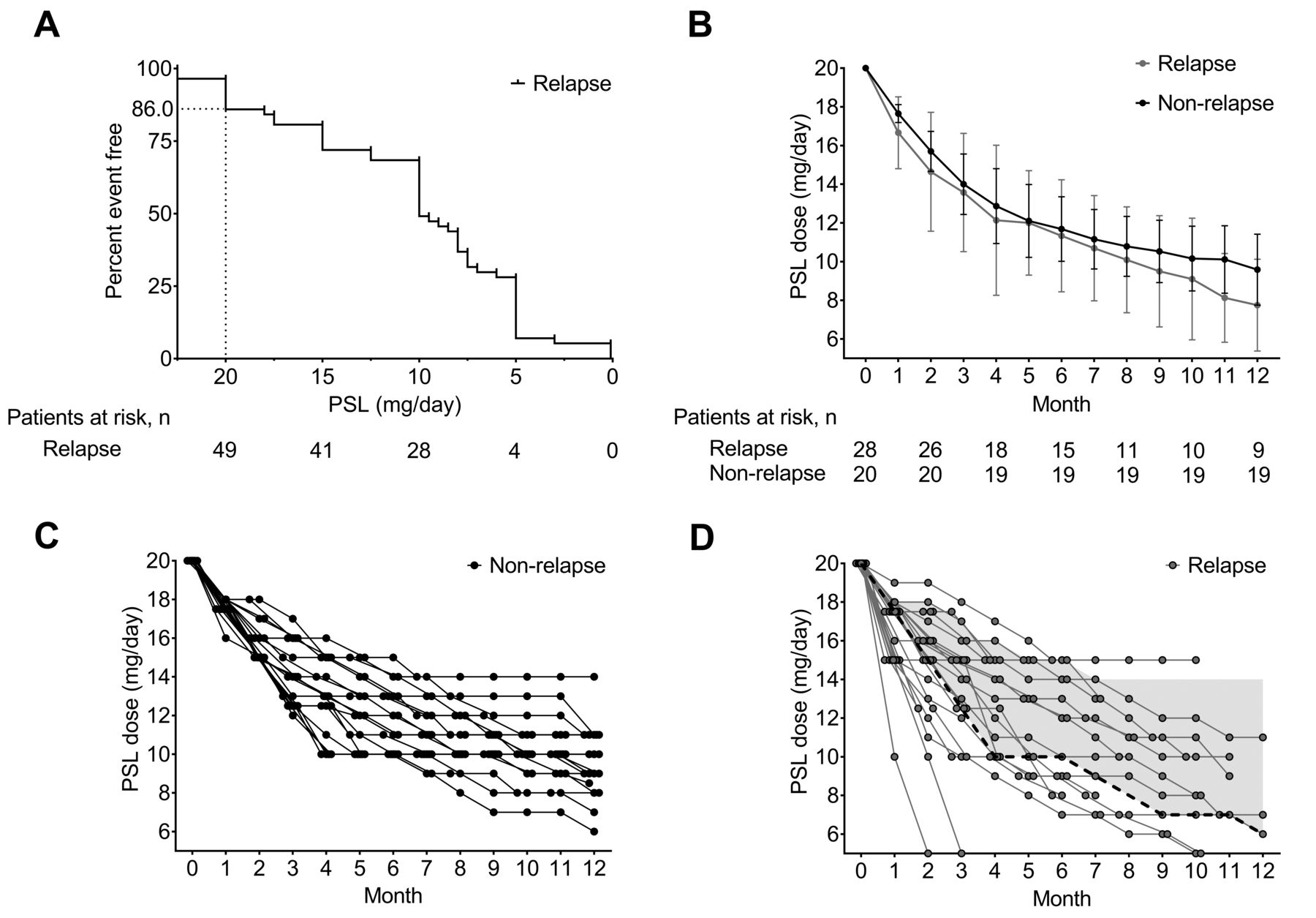
Reduction rate of prednisolone below 20 mg/day. A. The correlation between the relapse-free rate and the PSL doses (mg/day) in the relapse group (n = 57). B. Grey line represents mean doses of PSL (mg/day) in the relapse group (n = 28); black line represents mean doses of PSL in the nonrelapse group (n = 20; mean ± SD). C, D. Circles represent the sequential PSL doses (mg/day) used for individual patients in the nonrelapse group (n = 20; panel C) and the relapse group (n = 28; panel D) over 12 months. The dotted lines and grey area show the fastest reduction rate and the range of the reduction rate of PSL in the nonrelapse group, respectively (panel D). PSL: prednisolone.
Safety
As shown in Table 3, severe infection, bone fractures, osteoporosis, diabetes mellitus, dyslipidemia, cardiovascular diseases, hematological disorders, and GI bleeding, which are major PSL-related adverse events, occurred in 7, 4, 22, 19, 15, 3, 1, and 2 cases, respectively, during a median of 56 months of followup. Five deaths were observed (thrombotic microangiopathy, cerebral infarction, cardiac tamponade, infectious endocarditis, and unknown). To clarify the correlation of initial PSL doses and side effects, adverse events were compared between the ≤ 30 (n = 39) and > 30 mg/day PSL groups (n = 57). Adverse events did not statistically differ between the 2 groups (Table 3).
Adverse events.
DISCUSSION
This large retrospective study describes the longterm outcome of patients with TA and the effect of initial treatment on relapse. High-dose PSL is generally effective, but longterm PSL treatment can be associated with increased risk of adverse events. Therefore, immunosuppressive drugs could be combined with PSL to mitigate this risk. In our cohort, PSL was used in 91.4% of patients, consistent with other studies from India (95.2%)18 and Turkey (93%)19. However, overall use of immunosuppressive drugs was lower in our study (33.3%) than in these previous studies (93.6% and 84%, respectively). In a Japanese study, Ohigashi, et al17 reported that rates of PSL and immunosuppressant use were 79.2% and 18.9%, respectively. Therefore, use of immunosuppressants varies among different countries, institutions, and periods.
The difficulty in treating TA is its high relapse rate during tapering of treatments. In our study, relapse was observed in 59.4% of patients during a median of 56 months of followup. Previous reports showed that the cumulative relapse rate varies from 27% to 96%9,15,17,18,20, due to differences in patients’ clinical background, followup periods, and initial treatment. However, few studies have investigated risk factors for relapse.
In particular, little is known about effects of the initial PSL dose on relapse. Yang, et al21 reported a cohort in which 486 patients (85.9%) received a relatively lower dose of PSL (20–40 mg/day). Immunosuppressive drugs were used in only 23 patients. In that report, the total death rate during about 5 years of followup was 9.6%, which is higher than that in our cohort (4.7%) and other cohorts (0.7%–4.8%)15,17,18,20, indicating that lower-dose PSL monotherapy is insufficient for suppressing vascular inflammation and may harm the longterm outcome of patients with TA. Although the clinical activity and severity between the relapse and nonrelapse groups were comparable, initial PSL doses were significantly different. These data suggested that relapse occurred more frequently in patients treated with low-dose PSL than in those treated with high-dose PSL. Our data further confirmed that the similar relapse rate was observed regardless of the CRP levels (Figure 1D). The important point of our study is that the relapse-free rate with low-dose PSL (≤ 30 mg/day; monotherapy, 87.2%) was significantly lower than that with high-dose PSL (> 30 mg/day; monotherapy, 52.6%), although the former showed lower disease activity (Figure 1A). Of note, regardless of the discrepancy of initial PSL doses, there was no statistical difference in PSL doses at time of relapse between the groups (Figure 1E). In addition, the relapse-free rates tended to be higher in the ≥ 50 mg/day PSL monotherapy group than in the ≤ 40 mg/day monotherapy group (Figure 2A, B), indicating that the initial PSL dose is a strong determinant of relapse, and PSL monotherapy with ≤ 30 mg/day (equivalent to 0.54 mg/kg/day) should be avoided even if the disease activity appears to be low.
Goel, et al18 recently reported that the cumulative hazard for relapse in patients with an initial complete response was not significantly different between those initially treated with 0.5 versus 1 mg/kg/day of PSL. In their study, immunosuppressive drugs were used in 93.6% of patients, which was more frequent than that in our cohort (33.3%). Additionally, the specific immunosuppressants used were also different. They most commonly used mycophenolate mofetil (63.7%), which is not approved for TA in Japan. Alternatively, MTX, CSA, AZA, IVCYC, and TAC have been used for patients with TA. Biologic agents targeting tumor necrosis factor-α, CD20, and IL-6 receptor (IL-6R) have shown promising benefits in patients resistant to conventional therapy22,23,24. A recent randomized, placebo-controlled trial (TAKT study) investigated the efficacy and safety of tocilizumab (TCZ), a biologic agent targeting IL-6R, in patients with refractory TA25. This study showed the favorable effects of TCZ compared with placebo regarding time to relapse and thus has the potential to change the therapeutic strategy in TA. TCZ was administered in 10 patients who relapsed in this cohort. The addition of immunosuppressants tended to improve the relapse-free period in our cohort as well (Figure 2C), suggesting that combination therapy has the potential to delay time to relapse. Therefore, low-dose PSL administration combined with immunosuppressants should be considered.
Glucocorticoids such as PSL are essential in TA management, but their longterm use results in many side effects that are mostly time- and dose-dependent26. We investigated major events related to PSL. The adverse event incidence is comparable between the relapse and nonrelapse groups. Upon relapse of vasculitis, PSL doses are usually increased to control the disease. Further, as shown in Table 3, the difference in adverse events was also assessed between the ≤ 30 and > 30 mg/day groups, which showed no statistical difference. Administration of monotherapy with low-dose PSL is unfavorable because of a strong likelihood of relapse.
Faster reduction of PSL is reportedly associated with relapse17. In our cohort, the mean reduction rate of PSL was faster in the relapse group than in the nonrelapse group. In particular, the mean tapering speeds of PSL after the dose had been tapered to 20 mg/day were significantly faster in the relapse group. However, these numbers do not directly represent the practical tapering doses in each patient because they were affected by the length of the followup periods. Therefore, we compared the actual doses of PSL after the dose had been tapered to 20 mg/day between the relapse and nonrelapse groups. The comparison revealed that the mean PSL doses did not significantly differ between the 2 groups (Figure 3B). Thus, the statistical significance of the reduction rate below 20 mg/day can be explained by the long followup period in the nonrelapse group. The comparison of individual PSL doses between the nonrelapse (Figure 3C) and relapse groups (Figure 3D) revealed important findings regarding the optimal reduction rate of PSL. The fastest reduction rate in the nonrelapse group was 2.5 mg/month until a PSL dose of 10 mg/day was reached, maintenance of 10 mg/day PSL for 2 months, and then tapering the dose by 1.0 mg/month (Figure 3C). A faster rate of PSL dose reduction resulted in relapse (Figure 3D). Such faster reduction was applied for 53.6% of the relapse cases (68.4% were > 30 mg/day of PSL and 88.9% were combination therapy). Therefore, the reduction rate should be slower than the one described in this protocol despite the initial PSL dose and combination therapy. Another point to note is the threshold PSL dose associated with relapse. Relapse was observed in patients with a reduction rate of 2.5 mg/month until a dose of 10 mg/day was reached. PSL was continuously tapered in the relapse group, whereas PSL dose was maintained for 2 months in the nonrelapse group. As shown in Figure 3A, 31.0% of relapses occurred at a PSL dose of 10 mg/day. Given the possibility that 10 mg/day of PSL is the threshold for relapse, careful attention is needed while tapering doses around 10 mg/day.
There are several limitations of our study. First, this was a retrospective study. Although TA is a rare disease, prospective studies would be required to confirm our findings. Second, we evaluated disease activity and relapse according to NIH criteria or CRP levels. TA is well known to deteriorate in some patients without increased CRP levels. The Indian Takayasu Clinical Activity Score has been reported as an alternative evaluation tool of disease activity in TA to standardize the method for assessing the disease activity16. Dagna, et al27 reported that pentraxin 3 (PTX3) is a promising biomarker for monitoring of disease progression. Additionally, Ishihara, et al28 showed that PTX3 increased even without any increase in CRP levels. Third, there are missing data regarding inflammatory marker levels and PSL doses at relapse (Figure 1A, D, E).
In our study, 59.4% of patients experienced relapse, and an initial monotherapy with ≤ 30 mg/day PSL resulted in a higher relapse rate than high-dose PSL, even with low disease activity. The combination therapy group showed a slightly lower relapse rate in the initial 2 years but not at subsequent periods compared with the PSL monotherapy group. These results indicate that initial monotherapy with ≤ 30 mg/day (equivalent to ≤ 0.54 mg/kg/day) of PSL is undesirable because of its potential to increase the relapse rate and lead to further vascular damage in patients with TA.
APPENDIX 1.

Treatment flowchart of 105 patients with Takayasu arteritis. PSL: prednisolone.
Footnotes
This work was partly supported by JSPS KAKENHI (grants 16H06642 and 18K16136 to TS) and research grants from Kanae Foundation and Nanbyo Medical Foundation (to TS).
- Accepted for publication May 3, 2019.








{kind=link}
{kind=link}
{kind=link}
{kind=link}