

Abstract
Objective. To use ultrasonography to study whether the duration of psoriatic dactylitis was associated with different patterns of extracapsular and synovial-based involvement.
Methods. One hundred cases of hand dactylitis from 85 patients with psoriatic arthritis (PsA) were consecutively enrolled in a multicenter cross-sectional study and divided into 2 groups according to dactylitis duration (shorter or longer than the median: 20 weeks). All dactylitis fingers were investigated using high-frequency ultrasound both in greyscale (GS) and power Doppler (PD), evaluating the presence of flexor tenosynovitis, soft tissue edema, subcutaneous PD signal (PDS), extensor tendon involvement, and joint synovitis.
Results. Cases with a shorter dactylitis duration (< 20 weeks) had a significantly higher prevalence of GS flexor tenosynovitis of grade > 2, PD flexor tenosynovitis, soft tissue edema, and subcutaneous PDS (p = 0.001, p < 0.001, p < 0.05, and p = 0.001, respectively). However, the presence of synovitis in GS and PD mode (in both cases at proximal interphalangeal level) was more frequent in patients with longer dactylitis duration (p < 0.001). When detected in the chronic form, flexor tenosynovitis was grade 2 or lower.
Conclusion. In a large cohort of PsA hand dactylitis, we found a predominant extracapsular inflammation (flexor tenosynovitis and soft tissue edema) in early cases and a high prevalence of joint synovitis at proximal interphalangeal level in the chronic form. However, longitudinal imaging studies are needed to clarify these aspects.
Dactylitis is a common feature of psoriatic arthritis (PsA), occurring in 16% to 49% of patients with PsA, mostly in early disease1,2,3. As the most specific PsA manifestation it has been included in the ClASsification for Psoriatic ARthritis (CASPAR) criteria4,5, although it has been observed in all forms of spondyloarthritis6, including the enteropathic form7. Dactylitis is defined as diffuse and uniform swelling of the entire digit and it is considered a clinical marker of disease severity8,9. Clinically, it can present as a tender, painful, warm, and erythematous digit (acute form). It can also present as a swollen paucisymptomatic digit, not associated with inflammatory modifications (chronic form)10, which remains poorly understood11,12.
Dactylitis was long considered to be the result of the association of the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints with flexor tenosynovitis13,14. In the 1990s, early ultrasound (US) studies reported a predominant flexor tenosynovitis, while the frequency of coexisting joint synovitis varied from 16% to 62%15,16,17, and these data were confirmed by subsequent magnetic resonance imaging (MRI) studies18,19,20. These results led the authors to conclude that flexor tenosynovitis was a major contributor to the clinical appearance of dactylitis, and joint synovitis was a variable coexisting feature. Fournié, et al21 used US to show diffuse digital soft tissue inflammation in dactylitic patients (reported as subcutaneous and extratendinous) and termed this lesion pseudotenosynovitis. A recent study independently reported that this lesion was useful in the differentiation of PsA from rheumatoid arthritis22.
Only a recent US study of 48 cases of PsA dactylitis evaluated the correlation between sonographic features and duration of dactylitis. That study highlighted a significantly higher prevalence of flexor tenosynovitis and peritendinous soft tissue edema in acute form (< 24 weeks) and joint synovitis in the chronic form (> 24 weeks)23. We tested the hypothesis that earlier disease may be associated with a greater degree of extracapsular pathology, in line with prominent accessory pulley involvement in early disease. This multicenter observational cross-sectional study was designed to confirm in a greater number of patients the association between US patterns of disease compartmentalization in dactylitis and its duration.
MATERIALS AND METHODS
Patients
We performed a cross-sectional multicenter study on consecutively enrolled PsA patients with finger dactylitis who were in 3 Italian rheumatology centers (Naples, Reggio Emilia, and Negrar) with a recognized expertise in PsA and US imaging, between August 2017 and September 2018. The study was approved by the local ethics committees of the participating centers and was conducted in conformity with The Declaration of Helsinki (Ethical committee approval number: 5/12). Written informed consent was obtained from all participants.
The inclusion criteria were the fulfillment of CASPAR criteria in patients older than 18 years1 having an acute or chronic dactylitis2 with a duration of more than a month. The exclusion criteria were the following: (1) current engagement in heavy manual work, (2) recent history of hand trauma, (3) treatment with biologic synthetic disease-modifying antirheumatic drugs (DMARD), and (4) a previous corticosteroid injection in the involved finger.
Before US examination, a clinical assessment was performed by clinicians (AM, CS, RS) with longstanding expertise in the field of PsA who diagnosed the dactylitis using the dactylometer and the Leeds Dactylitis Index (LDI)24. The LDI measures the ratio of the circumference of the involved digit to the circumference of the contralateral digit; a minimum difference of 10% is necessary to define a dactylitic digit. The ratio of circumference is multiplied by a tenderness score (0 = no tenderness, 1 = tender, 2 = tender and winces, 3 = tender and withdraws).
The rheumatologic evaluation included tenderness of the involved finger, tender joint count (TJC), and swollen joint count (SJC). Erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and rheumatoid factor were collected. The duration of dactylitis was defined from the onset of reported diffuse digital swelling and pain.
For the purposes of analysis, we divided all cases of dactylitis into 2 groups according to its duration (shorter or longer than the median: 20 weeks). Moreover, all the cases were split into quartiles based on dactylitis duration.
US protocol
US examination of the dactylitis finger was performed by 3 rheumatologists (NG, PM, IT), expert in musculoskeletal US examination and blinded to clinical and laboratory data. All US scans were performed using a MyLab 70XVG machine equipped with a 6–18 MHz linear transducer (Esaote SpA). The US greyscale (GS) imaging measurements were optimized for maximal image resolution. Power Doppler (PD) settings were standardized at the following values: 500 Hz for pulse repetition frequency, 3 for wall filter, 4 for persistence, and color gain 45–55%. The window of the color box was restricted to the areas studied.
Flexor and extensor tendons, MCP, PIP, and DIP joints of the affected fingers were assessed by GS and PD US evaluation in longitudinal and transverse scanning views, in accordance with current guidelines and publications25,26. Joints were examined from both dorsal and volar sides. The following dactylitis-related sonographic lesions were investigated: flexor tenosynovitis (both in GS and in PD mode), soft tissue edema, subcutaneous PD signal (PDS), extensor tendon involvement (including paratenonitis and enthesitis of extensor tendon at proximal-interphalangeal joint), and synovitis (both in GS and in PD mode).
Tenosynovitis was defined in GS according to the Outcome Measures in Rheumatology (OMERACT) definitions27. Soft tissue edema was defined as a diffuse hypo/isoechoic thickening of the extratendinous soft tissues around the flexor tendon (pseudotenosynovitis) with positive PDS in the subcutaneous tissue, in long axis view21. We defined paratenonitis as a hypoechoic area surrounding a tendon without synovial sheath, with or without peritendinous PDS28,29. Enthesitis of extensor tendon at PIP joint was defined by the presence of hypoechoic and increased thickness of the tendon insertion into the bone, as compared to the body of the tendon and to the contralateral30,31.
Synovitis was defined according to the recent European League Against Rheumatism–OMERACT definition as hypoechoic synovial hypertrophy regardless of the presence of effusion and any grade of PD signal32. Tenosynovitis was assessed using the 4-grade semiquantitative scoring scale in GS and Doppler mode, as proposed by the OMERACT US group27. Synovitis was scored using a semiquantitative score (0–3) both for GS and Doppler mode, according to studies32,33.
Statistical analysis
The statistical analysis was performed using SPSS, version 23. All quantitative variables were expressed as mean ± SD or median and range in case of strong violation of normality, while qualitative variables were expressed as percentages.
Intraobserver and interobserver reliabilities were obtained in 2 measurements (basal and at 3 months from the first US evaluation) using 20 static images of 20 patients. We used the Cohen’s κ coefficient for each sonographic lesion, and values > 0.8 were considered excellent. Continuous variables were compared using T test or nonparametric tests when appropriate. Noncontinuous variables were compared using chi-square test. Statistical tests were performed at a significance level of α = 0.05.
RESULTS
Clinical features of the 2 dactylitis groups
The main demographic, clinical, and laboratory characteristics of the 2 groups (shorter or longer than 20 weeks) are reported in Table 1. Both groups were not significantly different for body mass index, PsA duration, TJC, SJC, ESR, CRP, and therapies. However, patients with longer dactylitis duration were predominantly male (p < 0.05) and older (p = 0.01). The patients of the 2 groups were significantly different for the frequency of tenderness (p < 0.001). Moreover, the mean values of LDI score and patient pain visual analog scale (VAS) score were significantly higher in cases with shorter dactylitis duration (p < 0.001).
Clinical and laboratory features according to dactylitis duration (shorter or longer than the median: 20 weeks).
Sonographic intraobserver reliability
For the 3 sonographers (NG, PM, IT), the intraobserver reliability was excellent for all variables (κ > 0.8). The interobserver reliability depicted by κ coefficient was 0.87 (95% CI 0.81–0.93) for GS flexor tenosynovitis, 0.83 (95% CI 0.75–0.90) for PD flexor tenosynovitis, 0.89 (95% CI 0.85–0.93) for soft tissue edema, 0.86 (95% CI 0.74–0.97) for subcutaneous PDS, 0.88 (95% CI 0.84–0.92) for extensor tendon involvement, 0.84 (95% CI 0.76–0.93) for GS synovitis, and 0.91 (95% CI 0.85–0.96) for PD synovitis.
Sonographic findings
At least 1 US abnormality was found in all patients. Flexor tenosynovitis was seen in 88% of dactylitis (grade > 2 in 46% of cases), while related PD flexor tenosynovitis was observed in 72% of cases (grade > 2 in 57% of cases). Soft tissue edema was present in 91% of dactylitis and subcutaneous PDS was present in 85% of cases. Extensor tendon involvement was evident in 12% of dactylitic fingers (with associated PDS in 10% of cases). GS synovitis involving at least 1 joint was observed in 40% of cases; it was present more frequently at PIP level (28% of cases), while it was present at MCP and DIP level in 15% and 9% of cases, respectively. PD synovitis involving at least 1 joint was evident in 21% of cases; it was more frequently detected at PIP level (17% of cases) and it was seen at the MCP and DIP levels in 7% and 4% of cases, respectively. Simultaneous synovitis of MCP, PIP, and DIP joints was not found in any patient.
Flexor tenosynovitis plus soft tissue edema were present in 79% of cases, while flexor tenosynovitis plus joint synovitis involving at least 1 joint were observed in 31% of cases. Soft tissue edema plus joint synovitis involving at least 1 joint were evident in 12% of dactylitic fingers.
Table 2 shows the frequency of US abnormalities in the 2 groups of patients. Cases with shorter dactylitis duration (< 20 weeks) had a significantly higher prevalence of GS flexor tenosynovitis of grade > 2 and PD flexor tenosynovitis (any grade; p = 0.001 and p < 0.001, respectively). Extracapsular soft tissue edema was more common in the shorter disease duration group (p < 0.05; Figure 1 and Figure 2). Likewise, subcutaneous PDS was more common in the shorter disease duration group (p = 0.001). On the other hand, the presence of synovitis in GS and PD mode (in both cases at PIP level) was more frequent in patients with a dactylitis duration ≥ 20 weeks (p < 0.001 and p = 0.02, respectively). Figure 3 reports the prevalence of selected US abnormalities after splitting cases into quartiles based on dactylitis duration.

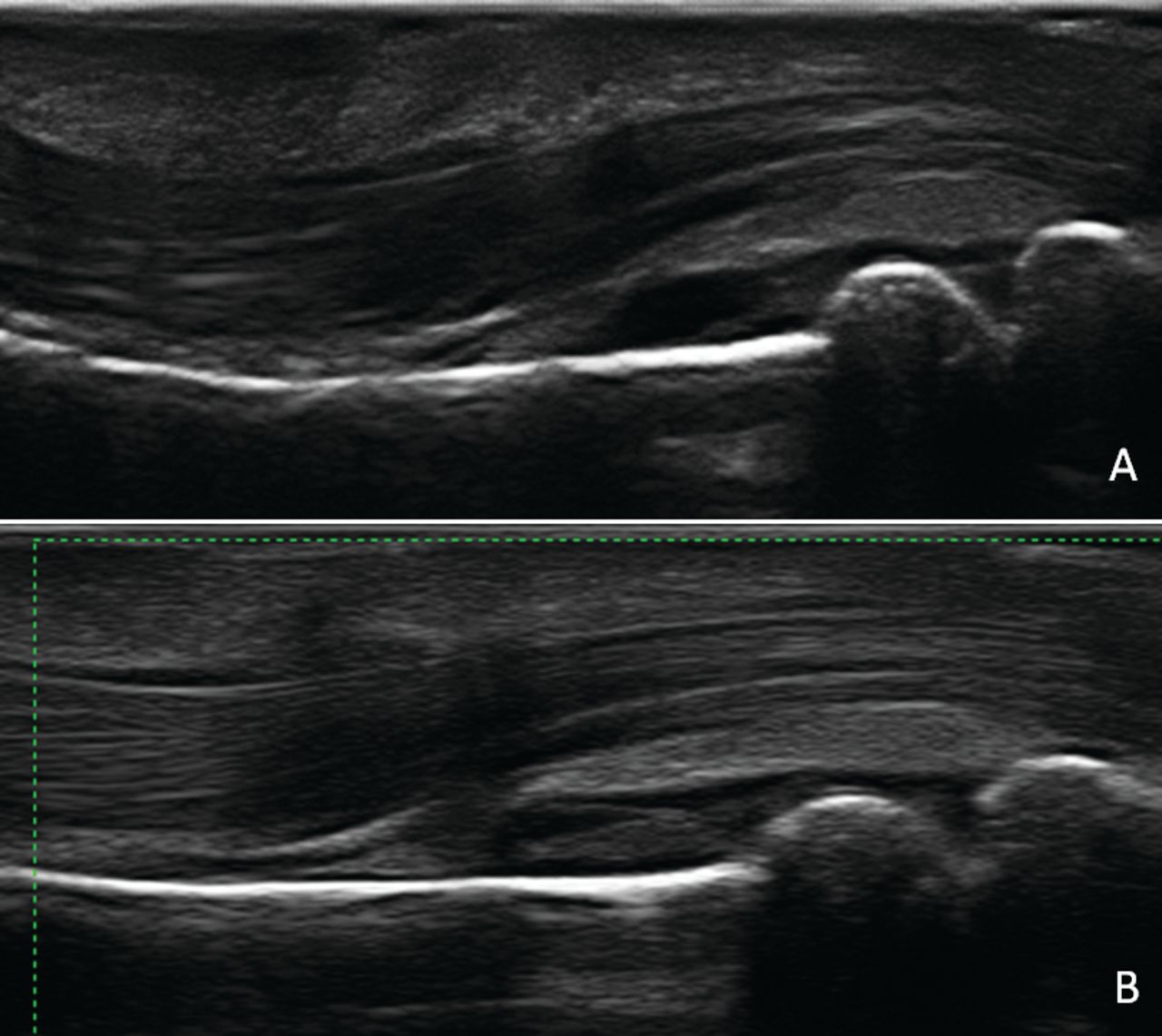
Longitudinal views of dactylitis belonging to the first group (dactylitis duration shorter than 20 weeks). A. Ultrasound shows flexor tenosynovitis of grade 2 with soft tissue edema (white arrowheads), whereas joint synovitis is absent. B. Power Doppler signal (PDS) is present around the tendon fibers and in subdermal tissue; intrarticular PDS is absent.
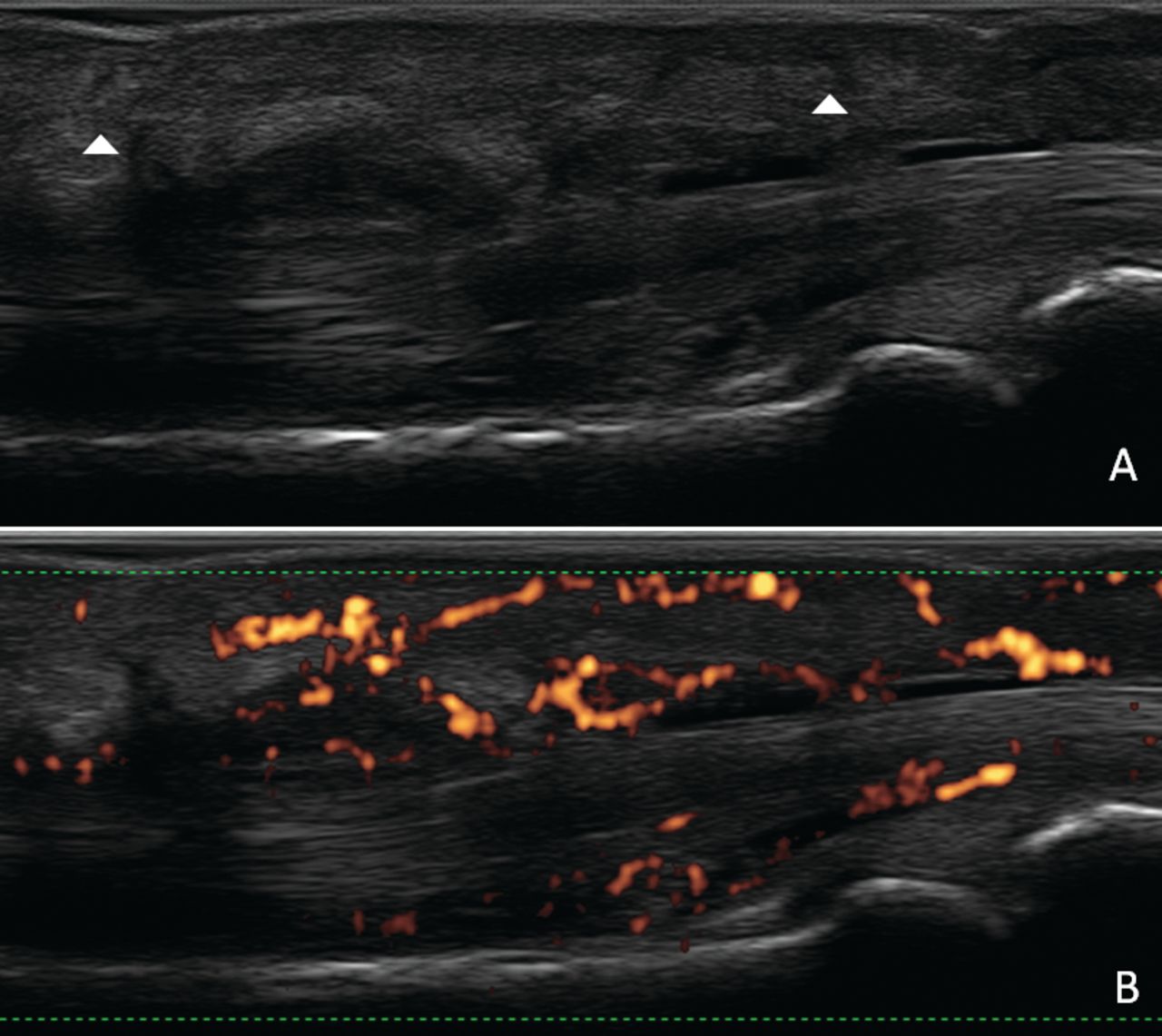
Longitudinal views of dactylitis belonging to the second group (dactylitis duration longer than 20 weeks). A. Ultrasound shows no peritendinous edema, distension of the flexor tendon sheath (grade 1), and of the capsule (grade 3) at proximal interphalangeal joint level. B. Power Doppler signal is absent in the articular, peritendinous, and subcutaneous areas.
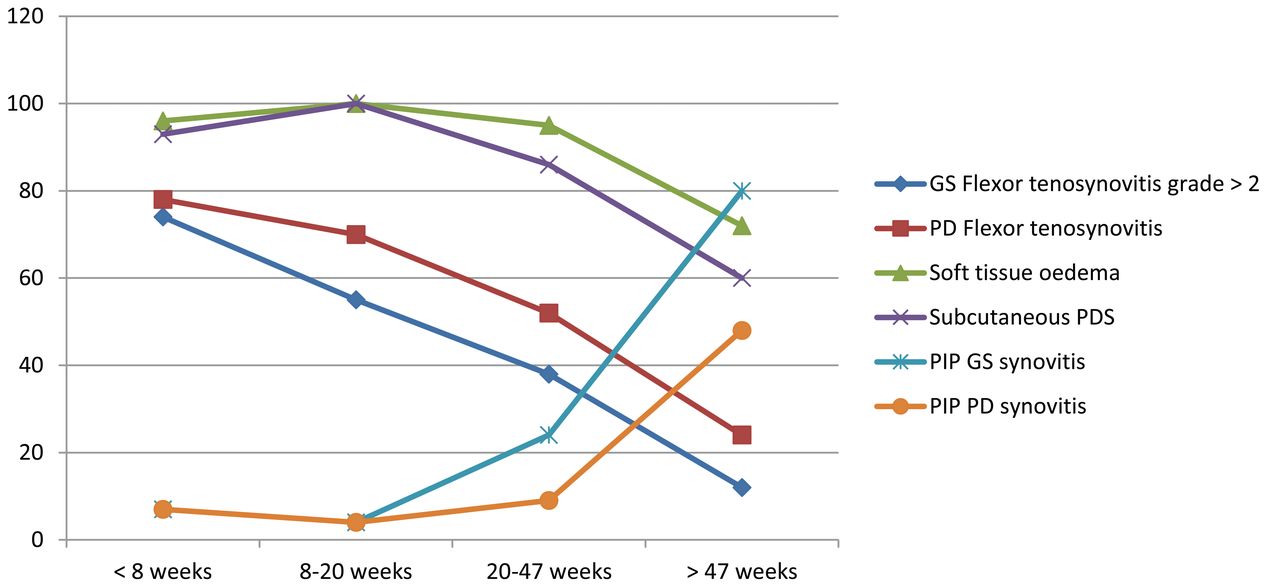
Prevalence of selected US abnormalities after splitting cases into quartiles based on dactylitis duration. US: ultrasound; GS: greyscale; PD: power Doppler; PDS: subcutaneous PD signal; PIP: proximal interphalangeal.
Prevalence of ultrasonographic abnormalities according to dactylitis duration (shorter or longer than the median: 20 weeks).
We found no differences in the prevalence of the US abnormalities (in particular flexor tenosynovitis, soft tissue edema, and joint synovitis) comparing subjects treated versus not treated with conventional synthetic DMARD either in the general population or in the subgroups with dactylitis duration less than and > 20 weeks (Table 3).
Prevalence of ultrasonographic abnormalities according to therapy.
DISCUSSION
This is the first multicenter study, to our knowledge, to evaluate the relationship between US lesions and dactylitis duration in a large PsA hand dactylitis cohort using high-frequency US. Our findings revealed that the prevalence of GS flexor tenosynovitis of grade > 2, PD flexor tenosynovitis, soft tissue edema, and subcutaneous PDS are higher in patients with shorter dactylitis duration. Moreover, the mean values of LDI score were significantly higher in cases with shorter dactylitis duration.
On the other hand, the presence of GS synovitis and intraarticular PDS at PIP level was more frequently observed in patients with longer dactylitis duration. However, flexor tenosynovitis was also present in the chronic form but was of a lesser magnitude. These results confirm the association between US patterns of disease compartmentalization in dactylitis and its duration, as already shown in a previous study with a smaller sample of patients23.
At present, the natural clinical course of dactylitis remains largely unknown and longitudinal studies on soft tissue changes in dactylitis have never been done. Previous US15,16,17 and MRI18,20,34 studies have demonstrated that dactylitis is characterized by the variable association of inflammatory involvement of flexor tendons (tenosynovitis), adjacent soft tissue thickening/edema, and synovitis of MCP, PIP, and DIP joints. The main limits of previous US studies were the very small samples of patients (usually < 30 dactylitic digits), the low frequency of the probe used (7.5 or 10 MHz), and the absence of PD examination15,16,17. In accord with our data, an MRI study by Olivieri, et al of dactylitic toes with a dactylitis duration shorter than 7 weeks showed flexor tenosynovitis and peritendinous soft tissue edema in all patients and a low prevalence of joint synovitis19.
In our study, patients were enrolled in a consecutive manner and they were not selected according to treatment. Although we cannot exclude an influence of treatment on presence and severity of US abnormalities, the comparison of the prevalence of any US alterations did not differ between the treated and the untreated patient groups.
Our present study has several limitations. The main one is its cross-sectional nature. The duration of symptoms is therefore obtained only through medical history. Another limitation of our study is the artificial definition of acute or chronic dactylitis based on the median of the duration of symptoms in the patients of our group. In addition, we cannot exclude that patients with dactylitis duration > 20 weeks could have had a less severe form of dactylitis; only longitudinal studies can clarify these aspects. Moreover, we have used a very general definition of edema because there is currently no agreement on a definition of soft tissue thickening/edema. However, the high intra- and interobserver reliability of US abnormalities supported the validity of this definition. For a more correct evaluation of soft tissue changes in relation to dactylitis duration, it would be useful to use a semiquantitative score. Similarly, there is no precise definition and grading for the subcutaneous PDS. Another possible limitation is that we have enrolled patients with different drug treatments. Currently there are no data about modification induced by treatment of US characteristics of dactylitis. Moreover, no significant differences were present comparing treatment in the 2 groups of patients. Further, we did not evaluate lesions of volar plate, pulley, and extensor tendons at distal phalanx insertion because of limitations of the US machine we used. The study of these structures should be performed with a higher frequency probe (22–24 MHz).
This is the first multicenter study, to our knowledge, that evaluated the relationship between US lesions and dactylitis duration in a large PsA hand dactylitis cohort. Despite limitations of our study, we found a predominance of flexor tenosynovitis, soft tissue edema, and subcutaneous PDS in early cases and a high prevalence of joint synovitis at PIP level in the chronic form. Our findings could suggest a possible change from a predominant extracapsular pattern in the early phase to an intrasynovial pattern in the chronic evolution. However, longitudinal imaging studies are needed to clarify these aspects.
Acknowledgment
The authors thank Prof. Stefano Galletti for his suggestions.
- Accepted for publication April 24, 2019.








{kind=link}
{kind=link}
{kind=link}