

Abstract
Objective. To summarize patients’ preferences for disease-modifying antirheumatic drug (DMARD) therapy in rheumatoid arthritis (RA).
Methods. We conducted a systematic review to identify English-language studies of adult patients with RA that measured patients’ preferences for DMARD or health states and treatment outcomes relevant to DMARD decisions. Study quality was assessed using a published quality assessment tool. Data on the importance of treatment attributes and associations with patient characteristics were summarized across studies.
Results. From 7951 abstracts, we included 36 studies from a variety of countries. Most studies were in patients with established RA and were rated as medium- (n = 19) or high-quality (n = 12). The methods to elicit preferences varied, with the most common being discrete choice experiment (DCE; n = 13). Despite the heterogeneity of attributes in DCE studies, treatment benefits (disease improvement) were usually more important than both non-serious (6 of 8 studies) and serious adverse events (5 of 8), and route of administration (7 of 9). Among the non-DCE studies, some found that patients placed high importance on treatment benefits, while others (in patients with established RA) found that patients were quite risk averse. Subcutaneous therapy was often but not always preferred over intravenous therapy. Patient preferences were variable and commonly associated with the sociodemographic characteristics.
Conclusion. Overall, the results showed that many patients place a high value on treatment benefits over other treatment attributes, including serious or minor side effects, cost, or route of administration. The variability in patient preferences highlights the need to individualize treatment choices in RA.
Expanding treatment options for rheumatoid arthritis (RA) has led to increased choices for patients and physicians. These choices come with tradeoffs in risks and benefits, and there is growing recognition of the importance of including patient preferences in treatment decision making. With individual patients, shared decision making is regarded as the preferred approach to achieving evidence-informed decisions consistent with a patient’s values1. Within clinical practice guidelines, understanding patient preferences for key tradeoffs is a necessary step in the evidence-to-decision process2. Under the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach, strong recommendations are reserved for situations in which most patients would choose a treatment based on the balance of benefits and harms3. Summarizing the existing literature on patient preferences is a critical step in developing patient-centered guidelines.
Evidence on patient preferences can come from a variety of sources4. Researchers may record patients’ choices when presented with an informed choice, typically with a patient decision aid. Alternatively, the importance of outcomes or health states can be assessed either individually in absolute terms (unidimensional) or relative to each other (multidimensional)5. The absolute importance of a health state is usually expressed on a 0 (equivalent to death) to 100 (full health) scale. This can be derived through a simple visual analog scale (VAS) or utility elicitation techniques, where patients are asked to choose between continued existence in a given health state, or a return to full health but with a small chance of immediate death [standard gamble (SG)] or shortened life expectancy [time tradeoff (TTO)]6.
Alternatively, the relative importance of health states can be elicited through multidimensional methods such as a discrete choice experiment (DCE) that ask patients to rate, rank, or choose between treatment alternatives4. In a DCE, patients complete a series of choice tasks, in which they are presented with a choice of 2 or more treatments that differ in their attributes (e.g., characteristics such as dosing, cost, side effects, route of administration)7. The value patients place on each attribute is then estimated using statistical models, assuming that patients chose the treatment with the highest overall value.
The primary objective of our systematic review was to summarize the available quantitative evidence regarding the preferences of patients with RA for DMARD therapy. The secondary objective was to identify any associations between patient characteristics and preferences. The aim was to provide knowledge that can help inform treatment recommendations and clinical decision making for RA. By aligning treatment recommendations and decisions with patient preferences, patient adherence to DMARD therapy may increase8,9.
MATERIALS AND METHODS
Study design and inclusion criteria
We performed a systematic review to identify English-language studies in adults (age > 18) with a diagnosis of RA that assessed patients’ preferences for different DMARD, or treatment attributes relevant to a choice between DMARD. DMARD included any conventional synthetic DMARD (e.g., methotrexate), biologic originator or biosimilar DMARD (e.g., adalimumab), targeted synthetic DMARD (e.g., tofacitinib), or corticosteroids. We included any study that provided a quantitative assessment of patient preferences, which was defined according to the MeSH definition in the National Library of Medicine as an “individual’s expression of desirability or value of one course of action, outcome, or selection in contrast to others”10. This included studies that (1) examined the choices patients made when presented with a decision aid for alternate DMARD and (2) measured patient preferences for alternative treatment options or attributes relevant to a choice between DMARD.
We excluded studies reporting health-related quality of life (HRQOL) because HRQOL measures the value a patient places on their current health state and not their preference for potential treatment outcomes or attributes. We also excluded studies with mixed rheumatic disease populations, unless the data for patients with RA were reported separately. Because we were interested in information regarding patients’ preferences for attributes relevant to DMARD therapy, we excluded studies that measured patient preferences for an unrealistic outcome such as a complete cure. Finally, we also excluded studies that measured preferences for components of a single attribute (e.g., relative importance of questions within a functional status outcome, or specific mechanisms of an auto-injector); these tradeoffs were felt to be less relevant to treatment decision making in clinic or within guidelines. The study protocol was registered with Prospero (PROSPERO 2015 CRD42015027528).
Search strategy and data sources
We conducted a database search for studies on or before January 2018 in the following databases: Medline In Process and Other Non-indexed Citations, CENTRAL (Cochrane Central Registry of Controlled Trials), EMBASE (Excerta Medica Database), Psychinfo, and HealthStar. The MEDLINE search strategy is included in Supplementary Table 1 (available with the online version of this article). Briefly, the search combined keywords and subject headings for RA with terms for patient preferences or methods used to assess patient preferences. The MEDLINE and EMBASE RA filters were derived from Cochrane reviews and adapted for the other databases11. The patient preference filter was informed by a published systematic review of patient preferences12. We also reviewed the reference lists of all eligible studies.
Study selection
Two reviewers independently screened articles. Any article included by either reviewer in the title or abstract screen proceeded to full-text review, where disagreements were resolved by consensus or with a third reviewer if necessary.
Assessment of study quality
To assess for study quality and to identify potential biases, 2 reviewers used a methodological assessment tool previously developed by other investigators13. The checklist includes 31 questions to assess for potential biases across 5 domains: (1) external validity (i.e., is the studied population representative of the target population?); (2) quality of construct representation (i.e., are the health states considered appropriate, comprehensive, and meaningful?); (3) construct-irrelevant variance (i.e., were there factors outside of the measurement, such as task complexity, that may have affected responses?); (4) quality of reporting and analyses (i.e., were the data complete and analyzed appropriately?); and (5) other aspects that strengthen or weaken the study. After each of the 5 domains were evaluated, an overall quality rating (high/medium/low) was assigned to the study. The overall quality rating included a judgment across all domains for that outcome, although not all domains were equally weighted13. The quality rating was done by 2 independent reviewers, with disagreements resolved by consensus.
Data extraction and analysis
For each included study, 2 reviewers extracted the study method and considered attributes, the setting in which the study took place, number of patients involved, patient characteristics, treatment(s) of interest, and funding sources into a standardized form. The results of the studies were not combined into a metaanalysis because of the heterogeneity of the methodologies, patient populations, and treatment options evaluated. Instead, we summarized data into tables based on the type of study method used and highlighted overall themes across the body of evidence. For DCE, we summarized results across studies in a table of pairwise comparisons of attribute importance, as described below. Results for the association between patient characteristics and preferences were summarized descriptively.
For DCE studies, we calculated the proportion of times an attribute was preferred out of the total number of comparisons. For example, if remission and route of administration were both included as attributes in 3 different studies, and remission was more important in all 3, this would be presented as 3/3, favoring remission. If the number of studies in which each of the 2 attributes was favored was the same, then the word “neither” was placed above the ratio to reflect the fact that there was no overall direction of the preference. For these comparisons, we grouped similar attributes into 9 categories representing treatment benefits (remission/low disease activity, symptom/functional improvement, avoiding joint damage), adverse events (AE; serious and non-serious), dosing (onset/duration, route, frequency), and cost. If a study included more than 1 attribute in a given category (e.g., multiple AE), we considered the attribute category to be more important in that study if it was favored in the majority of pairwise comparisons. When drawing conclusions from these analyses, we were careful to consider that the attributes and levels varied considerably across studies. Thus, as a secondary summary, we also presented the utility values for each attribute and level, without summarizing across the studies. These were scaled so that they summed to 100 within each study.
RESULTS
Search results and study characteristics
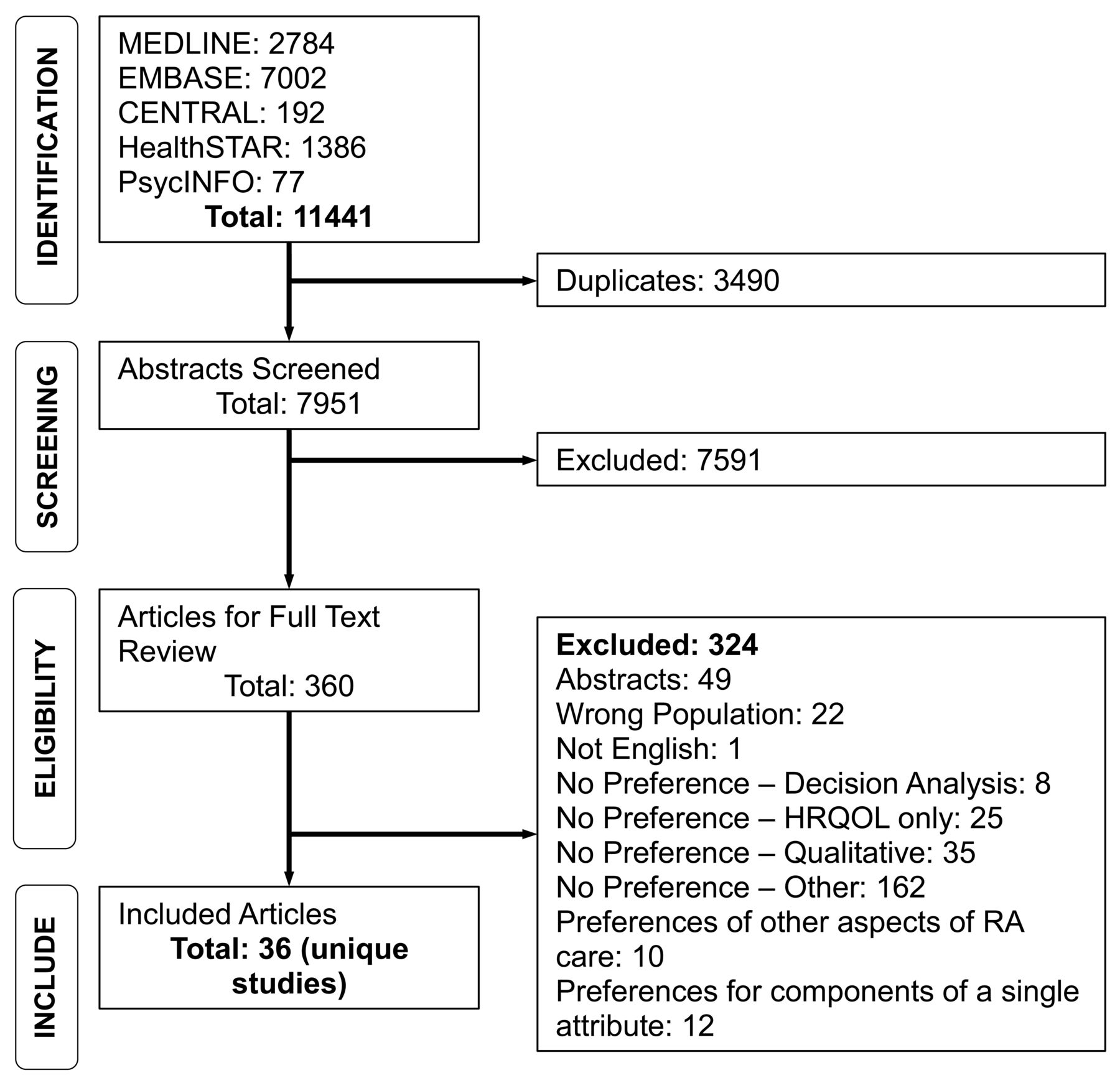
From 7951 records, we included 36 unique studies (Figure 1). The included studies were published between 1990 and 2018, across multiple countries, and had sample sizes ranging from 10 to 1588 (Table 1)14–20,23–42,52–59,60–65. Most studies included patients with established RA (mean disease duration 7–17 yrs), except 2 that examined the preferences of patients with early RA14,15. Most (n = 22) were focused on health states relevant to advanced therapeutics (biologic or targeted synthetic therapy), and in most studies, patients had previously or were currently taking 1 or more of the treatments that the study was focused on. Fifteen of the studies were funded partially or entirely by industry. The methods used to elicit preferences included DCE (n = 13); SG, TTO, or VAS (n = 3); willingness to pay (WTP; n = 2); and willingness to accept risk (n = 5; Table 1). Fourteen other studies used various rating or ranking tasks to evaluate patient preferences for different routes of delivery (n = 5), different treatment outcomes (n = 6), or different treatment options (n = 3; Table 1 with full details in Table 4)15,31–38,60,61,62,63,64. The attributes considered in each study varied considerably.

Flowchart of literature search results. HRQOL: health-related quality of life; RA: rheumatoid arthritis.
Characteristics of included studies.
Quality assessment of included studies
Overall, 12 studies were rated as high quality, 19 were medium, and 5 were low quality (Supplementary Table 2, available with the online version of this article). Low-quality studies typically had poor external validity with small sample sizes that did not reflect typical rheumatology patients with RA, and/or had complex surveys without adequate pretesting or piloting to ensure comprehension, leading to low ratings for the construct-irrelevant variance domain (i.e., understanding of the task). Most studies were rated as medium or high quality for construct representation and quality of reporting and analysis. Ratings of overall study quality were similar between DCE (4 high, 8 medium, 1 low) and non-DCE studies (8 high, 11 medium, 4 low).
Discrete choice experiments
The summary of pairwise comparisons of attribute importance across DCE studies is presented in Table 214,16,17,40,41,52–54,56–59, with additional details and calculated relative importance of attributes in Supplementary Table 3 (available with the online version of this article). For each pairwise comparison in Table 2, the attribute that was preferred most often is listed in each cell, along with the ratio of the number of times it was preferred over the total number of times those 2 attributes were compared across all studies. While the DCE studies were heterogeneous in their attributes and levels, some overall trends can be observed. Treatment benefits were often more important than both serious and non-serious AE across the ranges of levels considered in the studies. In particular, symptom/functional improvement was rated as more important than serious but rare AE in 5 of 8 studies (Table 2). Serious but rare AE were more important than more common but less serious “nuisance” side effects in 5 of 6 studies (2 ties). Cancer in particular, even when described as a “theoretical risk,” was often the most important AE14,16,17. In a study in patients with early RA, treatment benefits were the most important attribute14.
Relative importance of treatment attributes across discrete choice experiment studies.
Dosing and administration considerations were typically less important than benefits, but again this varied across studies (Table 2 and Supplementary Table 3, available with the online version of this article). The route and frequency were often more important than AE, both serious and non-serious. Most studies that included cost found that patients would be willing to pay at least US$100/month for the most desirable treatment attributes, including treatment benefits or avoiding side effects.
Standard gamble, time tradeoff, and VAS
Three studies measured the absolute importance of health states on a 0 (death) to 1 (full health) scale using a SG, TTO, or VAS (Table 3)18,19,20,23–29. Chiou, et al found that the American College of Rheumatology (ACR) 50 and ACR70 responses were similar in importance and considerably higher than the ACR20 response, which would support the use of the former in outcome evaluation in RA trials18. The greatest distinction in side effects was between “severe” and “moderate” with relatively little difference between moderate and mild (Table 3). Ferraz, et al found that patients were risk-tolerant and valued the described benefits of 15 mg prednisone (well-controlled disease but a high risk of side effects) considerably more than treatments with no prednisone (severe disease but no risk of side effects)19. Suarez-Almazor and Conner-Spady found that mild arthritis had relatively little loss in use compared to severe arthritis20. From a measurement perspective, both Ferraz, et al’s study and Suarez-Almazor and Conner-Spady’s study had considerably lower values when using a VAS versus other utility-based methods20,21, which is consistent with the broader literature22.
Summary of unidimensional studies assessing the absolute importance of health states and outcomes.
Willingness to pay
Two studies valued various health states directly using the WTP approach (Table 3). Slothuus, et al found that patients were willing to pay about 3× their current monthly drug expenditure for a treatment with antitumor necrosis factor properties (maximal improvement and small risk of mild infection)23,24. Tuominen, et al found that the severity of AM stiffness (which is not commonly measured in trials) was about 1.5× more important than its duration25.
Willingness to accept risk
Three studies that measured patient’s willingness to accept risk used very different approaches and had quite different findings (Table 3). Fraenkel, et al found that many patients with established RA were completely unwilling to accept even very rare (1/1000 or 1/100,000) risks associated with DMARD therapy for a beneficial treatment26,27. Similarly, Ho, et al found that patients were very unwilling to accept even a small risk of death for improvement in arthritis symptoms28. In contrast, O’Brien, et al found that patients were willing to accept a considerable risk of death for specific health benefits, which was highest for relief of pain29. The quality of these later 2 studies was, however, rated as low (Supplementary Table 2, available with the online version of this article).
Other studies
The remainder of studies used other rating or ranking methods to assess patient preferences for different modes of administration, treatment outcomes, or treatment options (Table 4). In 3 of the 5 studies examining patients’ preferred route of delivery, more patients preferred subcutaneous (SC) over intravenous (IV) therapy, although 2 of these found that 22% and 21% of patients expressed no preference30,31. The final study found preferences to be split (50%) between SC and IV32.
Other studies.
In the studies that evaluated the importance of treatment outcomes, reduction in pain and improvement in function (particularly hand/finger function and walking) and fatigue were consistently identified as highly important33,34,35. An additional study identified “being dependent on others” as the worst-case scenario for patients36. In the RA-Patient Priorities for Pharmacologic Intervention questionnaire, developed through an iterative process, the 6 most important outcomes to evaluate when assessing treatment efficacy were pain, activities of daily living, joint damage, mobility, life enjoyment, independence, fatigue, and valued activities35.
Finally, 2 studies assessed patient preferences for different treatment options in the context of guidelines37 or a randomized trial15. Fraenkel, et al trained a patient panel in the GRADE approach for developing recommendations37. In 3/16 recommendations, the patient panel recommended a different treatment from the traditional physician-dominated panel because of differences in how patients valued treatment attribute tradeoffs. Patients were generally more willing to prefer the treatment with the highest chance of benefit. Similarly, in a posthoc study of patients with early RA from the BeST trial, more patients expressed a preference to be randomized to the methotrexate and infliximab arm (with the higher perceived chance of benefit) than the other trial arms. Patients also expressed a preference not to be randomized to the arm with corticosteroids15. Finally, van Overbeeke, et al found that most patients (60%) expressed no preference and trusted their physician for the decision whether to start a biosimilar or originator biologic DMARD38.
Associations between patient characteristics and treatment preferences
The observed associations between patient characteristics and preferences across studies are summarized in Supplementary Table 4 (available with the online version of this article). Overall, sociodemographic variables including age, education, ethnicity, and income were found to be associated with preferences more frequently than variables related to RA disease severity or treatment history. Two studies found that younger patients with RA placed higher importance on treatment benefits39,40 and 3 studies found that more educated patients with RA were more risk tolerant and preferred more intense treatments14,41,42. In 2 of 3 studies that examined an association between income and preferences, higher incomes were associated with greater risk tolerance14,41,42. Both studies that analyzed an association between ethnicity and risk tolerance found greater risk aversion in black patients compared to non-black patients41 and black patients compared to white patients42.
DISCUSSION
Our systematic review identified 36 studies that used various methods to investigate patient preferences for RA therapy and treatment outcomes. Among studies that compared treatment attributes, the benefits of treatment were generally more important than most risks. However, some studies found patients to be quite risk averse and there was important variability in preferences. Taken together, these results support current intensive treatment strategies, but highlight the critical need to individualize treatment decision making. For guideline developers, it suggests that many decisions may be preference sensitive. Under the GRADE approach, this would mean that for these treatment decisions, a conditional rather than a strong recommendation may be more appropriate3. Decision tools linked to these recommendations would then be encouraged to support shared decision making, which has been shown to improve decision-making quality43, and may also improve adherence44.
When grading the strength of treatment recommendations, guideline developers require an understanding of the relative importance of treatment outcomes and other attributes. With this in mind, we believe there are some general statements that are supported by the evidence:
Treatment benefits were usually more important than AE, but not always. In particular, some studies in patients with established RA found patients to be quite risk averse.
Serious but rare AE, including a hypothetical risk of cancer, were usually more important than more common but less serious AE.
Dosing regimens and monitoring requirements with therapy were generally less important than the benefits of treatment.
Patient preferences were variable and frequently associated with sociodemographic characteristics.
RA treatment approaches have moved toward a treat-to-target paradigm, with treatment escalation recommended until patients are in remission, or if not possible, low disease activity45,46,47. Implicit in this recommendation is that patients generally value the benefits of improved disease control more than any risks or undesirable aspects of treatment escalation. Overall, our findings support this, but with some caveats. Several studies showed that patients with established RA place a high importance of avoiding rare but serious AE. These patients may prefer to maintain their current treatment rather than escalate therapy in the setting of active disease that is well tolerated. This is recognized in guidelines, which support a less intensive treatment target, such as low disease activity, for some patients with established disease45,46,47. It is critical, however, that patients adequately understand both the risks of treatment and the risks of active disease. A reluctance to escalate treatment may be related to a misunderstanding of risks, particularly rare AE, which are difficult for patients to understand48. Although the evidence was not robust, 3 studies suggested that patients with early RA are relatively risk tolerant and would prefer early intensive treatment approaches with the greatest chance of benefit45,46,47. This may suggest that patients’ preferences change over time as patients adapt to their condition, which is supported by qualitative research49. It is also possible that patients with early RA in the studies were less well informed of the risks and benefits of treatment. Longitudinal studies could help clarify this.
In drawing the above conclusions, we must keep in mind the limitations of the available evidence. Several studies were judged to be of low or moderate quality, and the majority of the studies were of patients with established RA. The studies were often conducted in academic centers. Patients without access to these centers, including marginalized patient populations, may therefore be underrepresented. The majority of the studies were also industry-funded, which may have introduced bias. Most of the studies included patients currently receiving RA treatment and are therefore not reflective of the preferences of people who refuse or discontinue DMARD therapy.
Strengths of our review include the registered protocol, comprehensive search terms, and quality assessment, although the later 2 are also sources of potential limitations. Systematic reviews of patient preferences are quite new. We were over-inclusive with our search terms, but it is possible we missed relevant studies. A search filter for patient preference studies has been proposed and is in the process of being validated50. Similarly, the quality assessment of patient preference studies is not as well standardized as with other types of evidence. A systematic review identified 6 different quality rating systems, including the one we used51. Summarizing findings across studies is also challenging, given the study heterogeneity. We were careful in considering the study context in the interpretation of our findings, but it is possible others may have a somewhat different interpretation of the same evidence. Qualitative studies were also excluded; they may provide a better understanding of patient preferences but are even more challenging to summarize.
To the best of our knowledge, this is the first systematic review of patient preferences for DMARD treatment in RA. The results highlight the variability in preferences between patients, providing further rationale for efforts to promote shared decision making. For guideline developers, our review provides evidence to inform the risk/benefit tradeoffs that are required when developing and grading treatment recommendations. Guideline developers using our findings should judge whether the available evidence on patient preferences is sufficient to understand the balance of benefits and harms for their target patient population. If not, further research should be prioritized. It is hoped that our work can help inform the risk benefit tradeoffs required when deciding between RA treatments.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
The work was supported in part by a Canadian Initiative for Outcomes in Rheumatology Care grant and a Canadian Institute of Health Research (CIHR) grant (MOP - 142441). Dr. Hazlewood is supported by a CIHR New Investigator Salary Award and The Arthritis Society Young Investigator Salary Award. Dr. Marshall is supported by a CIHR Canada Research Chair in Health Services and Systems Research and the Arthur J.E. Child Chair of Rheumatology Outcomes Research.
- Accepted for publication April 1, 2019.








{kind=link}