

Abstract
Objective To describe the features of large-vessel vasculitis (LVV) as it affects the aorta and its branches in patients with relapsing polychondritis (RP).
Methods Retrospective data and systematic literature review.
Results Twenty-one patients were identified. LVV diagnosis was subsequent to RP and associated with extrachondral involvement in the majority of patients. Supraaortic vessels were more frequently involved (82%). Fourteen patients (67%) were treated with a conventional synthetic disease-modifying antirheumatic drug (csDMARD) and 7 (33%) with a biological DMARD (bDMARD). Vascular interventional procedures were performed in 10 patients (48%). Premature death due to cardiovascular complications was reported in 3 cases (14%).
Conclusion Extraaortic LVV is a serious and overlooked RP manifestation. All patients with RP should be investigated for LVV.
Relapsing polychondritis (RP) is a rare autoimmune disease characterized by recurrent inflammation of cartilaginous structures. All connective tissue can be involved, including that of the eye, heart, and inner ear1. Cardiovascular involvement occurs in 24–52% of patients2. It is more common in men and is associated with significant morbidity and mortality2. A single study reported an incidence of 6.4% for aortic involvement in patients with RP3. No data are available on patients with large-vessel vasculitis (LVV) affecting the aorta and its branches.
We studied the diagnostic investigations and therapy of 4 patients with RP and LVV followed in our center, and systematically reviewed available evidence to characterize this overlooked clinical entity.
MATERIALS AND METHODS
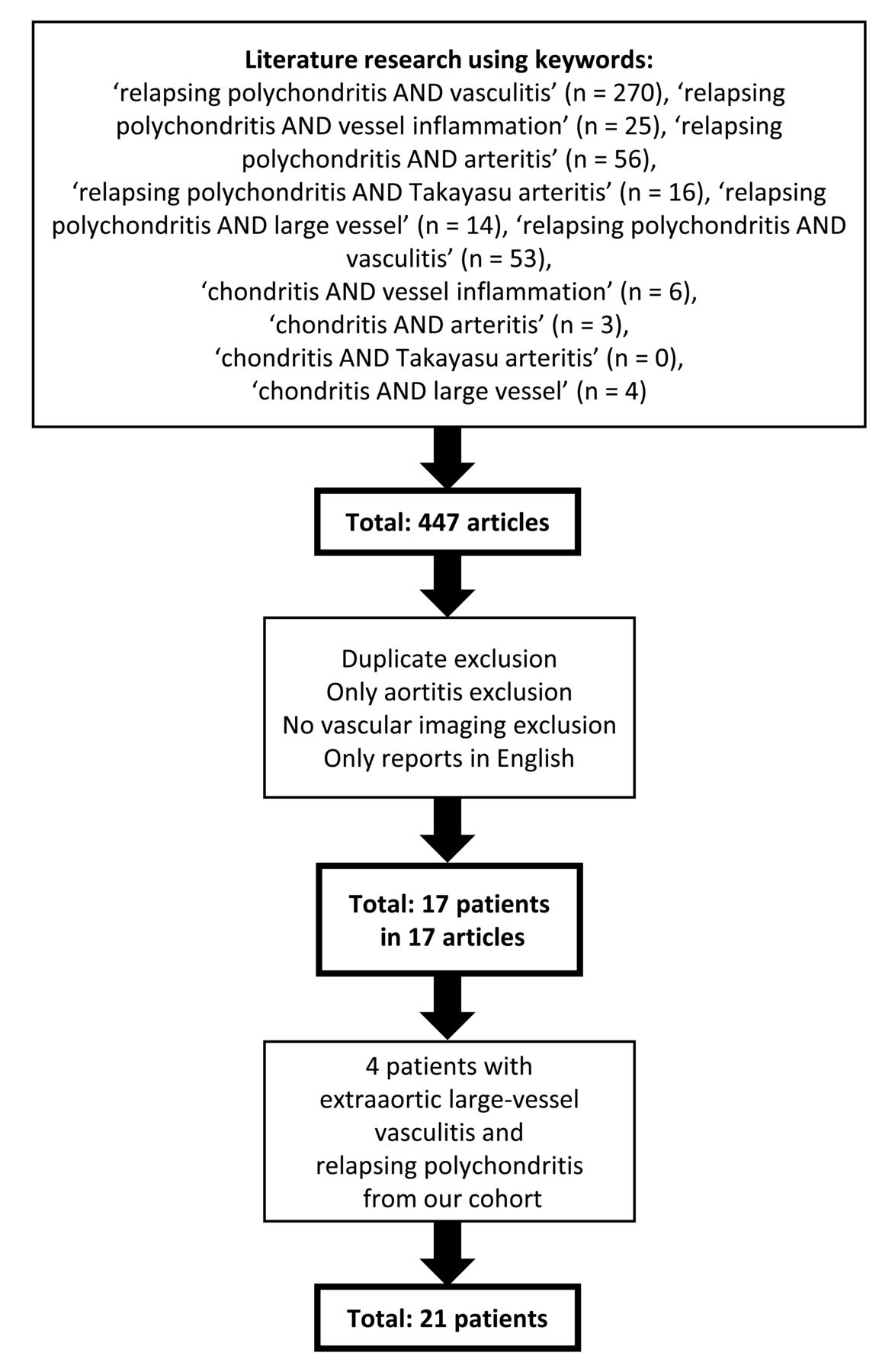
We performed a retrospective analysis of patients with RP diagnosed according to Michet criteria1 and followed at our center. We identified patients with LVV affecting the aorta and its branches. The Ethical Committee approved the study (approval number DSAN854-A-OS/1). Patients’ written informed consent was obtained. We made a systematic literature review with the following terms: “relapsing polychondritis,” “chondritis,” “vasculitis,” “vessel inflammation,” “Takayasu,” “arteritis,” and “large vessel.” We included only patients with unequivocal signs of extraaortic large-vessel inflammation: circumferential thickening, aneurysms, and stenoses, disclosed by magnetic resonance angiography (MRA), computed tomography angiography (CTA), CT/positron emission tomography (PET), arterial doppler ultrasonography (US), conventional angiography (CA), or documented postmortem. We excluded patients with vascular involvement restricted to the aorta (Figure 1).
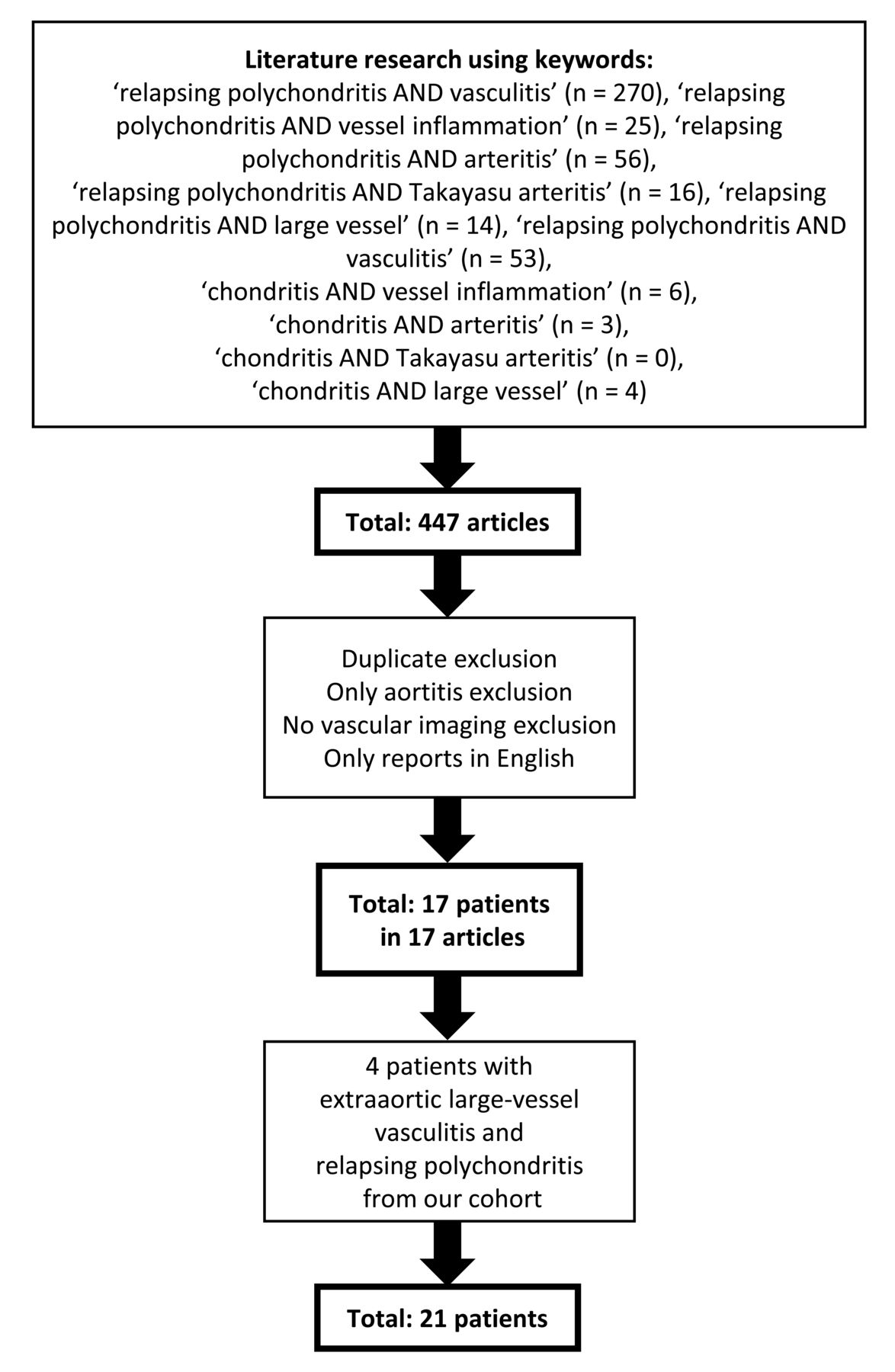
Flow diagram of the study selection process.
RESULTS
In our cohort of 41 patients with RP, we identified 4 (9.7%) with LVV affecting the aorta and its branches.
Case reports
Patient 1 was a 25-year-old woman who developed limb claudication and acute-phase reactant elevation. Abdominal bruits and absence of dorsalis pedis pulses were noted. MRA showed diffuse inflammatory thickening of the abdominal aorta, bilateral iliac arteries, superior mesenteric artery, and celiac trunk with stenosis of the infrarenal aorta and of the iliac arteries. CT/PET confirmed the presence of active inflammation. A course of steroids was started and golimumab therapy was introduced, but increased inflammatory markers persisted. After 18 months she developed an infrarenal aorta aneurysm (Figure 2A). She underwent abdominal aneurysmectomy with aortobifemoral bypass and was switched to tocilizumab (TCZ). After 12 months, an MRA revealed no vascular progression and a CT/PET showed no signs of inflammation. After 3 years of clinical remission, TCZ was discontinued.

Balanced turbo field-echo sequence magnetic resonance angiography (MRA) showing infrarenal abdominal aorta dilation in Patient 1 (panel A). High-resolution 3-D volumetric contrast-enhanced MRA showing wall thickening of brachiocephalic trunk and aortic arch in Patient 2 (panel B). 18F-fluorodeoxyglucose positron emission tomography showing radiotracer uptake in ascending aorta and arch of aorta in Patient 4 (panel C).
Patient 2 was a 37-year-old woman who developed dizziness and left upper limb paresthesia. An MRA revealed wall thickening of the ascending aorta, aortic arch, brachiocephalic artery, and left common carotid artery; occlusion of left subclavian artery, and stenosis of the celiac trunk (Figure 2B). Inflammatory markers were not increased. Because the disease was considered inactive, no immunosuppressive treatment was started. The patient then developed recurrent episodes of chondritis, so she was started on steroids and azathioprine (AZA). After 5 years, she was still asymptomatic. An MRA disclosed no vascular progression and a CT/PET showed no inflammation.
Patient 3 was a 20-year-old woman admitted for ascending aorta replacement. On admission, a significant increase of inflammatory markers with severe stenosis of the anterior descending coronary artery and active vasculitis of both common carotid arteries and abdominal aorta was noted. She was treated with steroids and cyclosporine (CSA), and then with methotrexate (MTX). Because of the persistence of systemic inflammation, she was started on cyclophosphamide (CYC). One year later, inflammatory markers were still increased and MRA showed abdominal aorta vasculitis worsening and involvement of the left iliac artery. Steroids were increased and anakinra was added, with initial benefit. After 18 months, she experienced an inflammatory flare. She was treated with pulse steroids and switched to TCZ. After 5 years she remains in good disease control.
Patient 4 was a 36-year-old man who underwent coronary revascularization. A perivascular biopsy revealed lymphoplasmacytic arteritis. CA disclosed involvement of the infrarenal aorta, celiac trunk, superior mesenteric artery, and critical stenosis of the renal arteries. He underwent bilateral renal angioplasty and AZA was introduced. Repeated attempts to titrate corticosteroids resulted in recurrent flares of systemic inflammation, so etanercept (ETN) was added. ETN had only marginal efficacy, as confirmed by a CT/PET that revealed inflammation of the arch and ascending aorta (Figure 2C), so it was substituted with infliximab (IFX), which had to be stopped because of infusion reaction. Over the years, various combinations of immunosuppressors were attempted. Only marginal results were obtained with a combination of TCZ, low-dose steroid, and mycophenolate mofetil (MMF). The patient eventually developed renal amyloidosis.
Literature review
We found 447 publications describing RP patients with vascular involvement. After application of our criteria, 17 reports about 17 patients with RP were included4–20 (Table 1A and Table 1B).
Summary of the cases of relapsing polychondritis (RP) with extraaortic large-vessel vasculitis in our cohort and reported in the literature.
Additional details about cases of relapsing polychondritis with extraaortic large-vessel vasculitis in our cohort and reported in the literature.
Patients were more frequently female (59%), with a median age of 29 ± 14.7 years. The main cartilaginous structures involved were ears (15 patients, 88%) and nose (12 patients, 71%). Tracheal chondritis was documented in 3 patients (19%), and costochondritis and involvement of the larynx in only 1 patient each (6%).
Arthralgia/arthritis and ocular inflammatory complications were present in 7 patients (41%). Two patients developed sensorineural deafness, 2 patients were affected by pyoderma gangrenosum-like lesions, and 1 patient had recurrent oral aphthae.
In 71% of cases, extraaortic LVV was diagnosed after the onset of the chondritis (mean delay, 48 ± 86.8 mos). In 29% of cases, the diagnosis was simultaneous. Involved arteries included subclavian (35%), common carotid (29%), internal carotid (18%), iliac (18%), renal (12%), vertebral (6%), axillary (6%), femoral (6%), inferior mesenteric (6%), and brachiocephalic trunk (12%). Supradiaphragmatic and infradiaphragmatic vessel involvement was present in 3 patients (18%), while the remaining (82%) had exclusive supradiaphragmatic involvement. In 5 patients (29%), vascular disease was limited to the branches originating from the aortic arch. Inflammatory coronary artery disease was present in 7 patients (41%) and it was isolated in 6. Ten patients (59%) had concomitant aortitis, mostly affecting the ascending aorta.
In 11 patients, vascular inflammation was diagnosed by means of CA. Three also underwent CTA, and 1 had both CTA and CT/PET. In 2 patients the imaging technique was MRA, in 2 patients CTA, and in 1 patient ultrasound. In 1 patient vascular involvement was documented postmortem.
All patients were treated with steroids as first-line therapy. In 10 patients (59%), a conventional synthetic disease-modifying antirheumatic drug (csDMARD) was added (CYC, 5; AZA, 4; MTX, 4; CSA, 2; MMF, diaminodiphenylsulfone, and chlorambucil, 1 each). A biological DMARD (bDMARD) was used in 4 patients (24%). In all cases, IFX was the initial bDMARD and in 1 case it was switched to rituximab. In 7 patients (41%), a vascular interventional procedure was required (coronary artery bypass graft, 3; aortic aneurysm repair, 2; aortofemoral bypass and percutaneous transluminal coronary angioplasty, 1). Three patients (18%) died from RP-related cardiovascular complications.
DISCUSSION
In our review we showed that patients with RP can develop LVV involvement of the aorta and its branches and we reported the disease features of this subgroup.
LVV diagnosis was subsequent or simultaneous to RP onset, suggesting that the RP-related systemic inflammation might also affect extraaortic large vessels. Nonetheless, because RP itself can be associated with many auto immune diseases, it is hard to say whether LVV involvement represents a different disease complicating the course of RP or a manifestation included in the clinical spectrum of RP.
Because the presence of LVV involvement in patients with RP is usually not actively investigated, in the majority of cases the diagnosis was made once vascular inflammation became clinically overt. Moreover, once patients are diagnosed with RP, steroid therapy is usually started, with benefits also for underlying vascular inflammation. This might explain why LVV diagnosis is usually made either concomitantly with RP onset (when a full assessment is performed), or with a significant diagnostic delay (when steroid therapy has been tapered).
In this subgroup of patients with RP, we observed a high frequency of auricular and nasal involvement and a low frequency of laryngotracheal manifestations. The majority of patients (81%) had involvement of other extrachondral sites, chiefly ocular inflammation and arthritis, indicating a higher burden of inflammation and a more severe disease phenotype. Moreover, similarly to other LVV, but dissimilarly to previous reports, a slight female preponderance seems associated with extraaortic LVV.
Heterogeneity of studies and clinical phenotypes preclude clear conclusions on the best therapeutic approach. Both csDMARD and bDMARD were used as steroid-sparing agents in refractory cases. Mixed results were obtained with CYC, AZA, and MTX. In one-third of patients, bDMARD were started after csDMARD failure. The experience with bDMARD was mainly restricted to 3 different mechanisms of action [anti-interleukin 1 (IL-1), anti-tumor necrosis factor-α, anti-IL-6r], with TCZ and IFX showing the best results.
Vascular involvement can be extremely severe in patients with RP, as documented by the significant percentage of patients undergoing vascular surgery.
We suggest that LVV involvement be clinically investigated and eventually confirmed in patients with RP both at diagnosis and during followup visits. In these patients, treatment choice should be focused both on RP and LVV manifestations, because LVV involvement can be insidious and can affect patient survival. Recent progress in imaging modalities together with emerging treatment options might open new possibilities for this orphan disease.
- Accepted for publication December 3, 2019.








{kind=link}
{kind=link}