

Abstract
Objective Determine the relation of symptomatic and structural features of patellofemoral osteoarthritis (PFOA) to psychological characteristics and measures of pain sensitization, in older adults with or at risk of knee osteoarthritis (OA).
Methods This study included 1112 participants from the Multicenter Osteoarthritis Study (713 females, mean age 66.8 ± SD 7.6 yrs, body mass index 29.5 ± 4.8 kg/m2). Participants were grouped based on the presence of PFOA symptoms (anterior knee pain and pain on stairs) and magnetic resonance imaging (MRI) PFOA (full-thickness cartilage lesion with bone marrow lesion): (1) patellofemoral (PF) symptoms with MRI PFOA; (2) PF symptoms without MRI PFOA; (3) MRI PFOA without PF symptoms; and (4) no PF symptoms or MRI PFOA (no PFOA). Relation of PFOA classification to depressive symptoms, catastrophizing, temporal summation (TS) and pressure pain thresholds (PPT) was evaluated using logistic (categorical variables) and linear regression (continuous variables).
Results Compared with no PFOA, those with PF symptoms with or without MRI PFOA had significantly greater odds of depressive symptoms, catastrophizing, and patellar TS (OR range 1.5–2.01), and those with PF symptoms without MRI PFOA had significantly greater odds of wrist TS (OR 1.66). Males with PF symptoms without MRI PFOA had significantly lower pressure PPT at the patella compared with no PFOA and those with MRI PFOA only (no symptoms). There were no significant differences at the wrist for males, or the patella or wrist for females.
Conclusion Persons with PFOA symptoms, regardless of MRI PFOA status, are more likely to demonstrate depressive symptoms, catastrophizing, and TS. Males with PFOA symptoms without MRI PFOA demonstrate local hyperalgesia.
Patellofemoral osteoarthritis (PFOA) is a distinct and important subgroup of knee osteoarthritis (OA), resulting in pain around or behind the patella during weight-bearing activities (e.g., squatting, stair ambulation)1. The patellofemoral (PF) joint is frequently the first knee joint compartment affected by OA, and the presence of isolated symptomatic PFOA increases the risk of an individual developing OA in their tibiofemoral (TF) joint2. Radiographic and magnetic resonance imaging (MRI) features of PFOA have a stronger association with pain and disability than those in the TF joint1. Importantly, PFOA tends to affect younger people more than tibiofemoral osteoarthritis (TFOA). Radiographic evidence of PFOA is present in 24% of adults with PF pain 26–50 years of age3 and 55% with PF pain 40–50 years of age4. Thus, symptomatic PFOA is likely to have substantial effects across occupational tasks, domestic and parenting duties, and physical activity, for a longer proportion of the lifespan.
Preliminary studies suggest that PFOA may be a sequela of PF pain in adolescents and younger adults5. The 2 conditions share similar symptoms, impairments, and biomechanical characteristics6. As the identity and evidence for PFOA has developed, studies have focused on characterizing the biomechanical features of the condition7, and evaluating the effects of biomechanical interventions (e.g., bracing, taping, exercise, manual therapy)8,9. However, findings in similar populations indicate that nonmechanical features may also contribute to PFOA symptoms and function. Younger adults with PF pain demonstrate psychological impairments that are related to pain and function10,11. Similarly, older adults with knee OA have an increased risk of developing depression compared with people without OA12.
Beyond psychological factors, other nonmechanical factors that have been increasingly studied in OA are neurobiological alterations in pain signalling that can influence the pain experience. One such mechanism is pain sensitization, which reflects facilitation in peripheral or central nociceptive signalling (i.e., peripheral and central sensitization, respectively). Measures of pain sensitization [lower pressure pain threshold, presence of mechanical temporal summation (TS)] have been associated with greater pain severity in older adults with knee OA, though whether there are differences between TFOA and PFOA has not been studied to date13,14. Of note, younger adults with PF pain also have lower pressure pain thresholds at local and remote sites compared to pain-free controls, indicating the presence of mechanical hyperalgesia15,16 and likely reflecting peripheral sensitization. Taken together, these findings suggest that people with PFOA may also demonstrate psychological impairments and pain sensitization, which may affect their response to traditional mechanical interventions. Although a recent study found no statistical differences in pressure pain thresholds between people with PFOA and controls17, their small sample size warrants further investigation of pain sensitization measures in this population. Without understanding contributions to PFOA symptoms beyond biomechanical aspects of the disease, a large burden of symptoms may remain unaddressed for those with PFOA.
The aim of this study was to determine whether symptomatic and structural features of PFOA are related to psychological characteristics and measures of pain sensitization in older adults with, or at risk of, knee OA.
MATERIALS AND METHODS
Participants
The Multicenter Osteoarthritis Study (MOST) is a National Institutes of Health–funded longitudinal cohort of 3026 people with, or at risk of, knee OA. The study design has been outlined in detail previously18. Briefly, participants 50–79 years of age (at baseline) were recruited from Iowa City, Iowa, and Birmingham, Alabama (USA), and standardized measures were collected at baseline and at 15, 30, 60, 72, and 84 months. Ethical approval was obtained from the institutional review boards of the University of Iowa (#201511711), University of Alabama at Birmingham (#000329007), University of California San Francisco (#10-00500), and Boston University Medical Center (#H-32956).
This cross-sectional analysis utilized data from the MOST 60-month visit, at which time measures relevant to this study were obtained.
Pain measures
Two measures from the MOST participants were used to define the presence of PF-related symptoms. These were selected based on consensus-based criteria1,7. A knee pain map was used to identify painful areas around the knee. Participants were asked to mark on the map where they experienced their knee pain when it was painful and could select multiple areas if appropriate. Anterior knee pain was defined as present if participants marked the area corresponding to the peripatellar region, regardless of whether other areas were also marked19.
Participants also completed the pain subscale of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)20. We used the item relating to pain during stair climbing (item 2), which was rated on a 5-point Likert scale (none, mild, moderate, severe, extreme). Pain during stairs was deemed to be present if participants rated experiencing pain during stairs that was at least mild in severity19.
Participants were then classified as having PF-related symptoms if they had both the presence of anterior knee pain (knee pain map) and at least mild pain on stairs (WOMAC pain item 2).
MRI
Participants underwent 1.0 T extremity MRI of both knees (OrthOneTM, ONI Medical Systems), using a phased-array knee coil. Fat-suppressed fast spin-echo proton density (PD)–weighted sequences were acquired in 2 planes: (1) sagittal [repetition time (TR) 4800 ms, echo time (TE) 35 ms, 3 mm slice thickness, 0 mm interslice gap, 32 slices, 288 × 192 matrix, 140 mm2 field of view (FOV), echo train length 8]; and (2) axial (TR 4680 ms, TE 13 ms, 3 mm slice thickness, 0 mm interslice gap, 20 slices, 288 × 192 matrix, 140 mm2 FOV, echo train length 8). A short tau inversion recovery sequence was also acquired in the coronal plane (TR 6650 ms, TE 15 ms, TI 100 ms, 3 mm slice thickness, 0 mm interslice gap, 28 slices, 256 × 192 matrix, 140 mm2 FOV, echo train length 8).
For the reading of MRI, 1 knee of each participant was randomly selected. All MRI were scored semiquantitatively by 2 trained and experienced musculoskeletal radiologists (AG and FWR), using the Whole-Organ Magnetic Resonance Imaging Score (WORMS)21. WORMS divides the patella, femur, and tibia into 14 subregions, including 4 PF subregions [medial and lateral patella; medial and lateral trochlea (anterior femur)]. Full-thickness cartilage loss was defined as WORMS scores of 2.5 (full-thickness focal defect < 1 cm in greatest width), 5 (multiple areas of full-thickness loss, of grade 2.5), or 6 [diffuse (≥ 75% of the region) full-thickness loss]22. The presence of a bone marrow lesion (BML) was defined as a WORMS score of ≥ 1 (bone marrow lesion of any size)22. Interrater reliability was adequate for cartilage (weighted κ 0.73) and BML (0.67)23.
Participants were classified as having PFOA on MRI if they had both a full-thickness cartilage lesion and a BML in the PF joint23.
Classification of symptomatic and structural PFOA
Participants were classified into 1 of 4 separate PFOA groups, based on the presence of PF symptoms and MRI PFOA: (1) PF symptoms with MRI PFOA; (2) PF symptoms (no MRI PFOA, as defined above); (3) MRI PFOA (no PF symptoms); and (4) no PFOA (i.e., no PF symptoms or MRI PFOA).
Psychological variables
Participants completed the Center for Epidemiological Studies Depression Scale (CES-D)24 and Coping Strategies Questionnaire (CSQ)25. The CES-D was dichotomized to indicate the presence (≥16) or absence (< 16) of depressive symptoms26. We used a single item (item 3) from the CSQ to represent pain catastrophizing: “When I feel pain I feel it’s terrible and that it’s never going to get any better.” Responses were dichotomized to indicate the presence (≥ 1) or absence (0) of pain catastrophizing.
Quantitative sensory testing
Quantitative sensory testing (QST) comprising mechanical TS and pressure pain threshold (PPT) was performed at the patella and the wrist. Specifically, the stimuli were applied over the midpoint of the patella (bilaterally) and distally over the dorsal aspect of the distal radioulnar joint (right side unless contraindicated). Participants were placed in supine position for measurement of patellar TS and PPT and were seated with their test forearm resting on a flat surface for the wrist TS and PPT measures. QST procedures in the MOST cohort have been detailed previously13.
TS was assessed using a 60 gauge von Frey filament (Aalborg University). Participants were asked to rate the pain experienced during 4 baseline stimulations over the test site to obtain a baseline score (0–10 numerical rating scale; higher scores indicate worse pain). The monofilament stimulus was then applied over the test site for 30 s, at a rate of 1 Hz. Participants rated their pain again immediately after the repeated stimulus, and 15 s after cessation. TS was defined as being present if participants reported increased pain after the test stimulus compared with baseline. Test-retest reliability (14 days) for TS was κ 0.6113.
PPT was measured over each test site using a handheld algometer with a 1 cm2 rubber tip (FDIX25, Wagner Instruments). Pressure was applied at a rate of 0.5 kg/s. Participants were instructed to indicate when the pressure first changed to slight pain. Three repetitions were recorded at each site (kg/cm2). The average of 3 repetitions was calculated for each site for use in further analyses, with lower PPT values indicating greater mechanical pain sensitivity. Test-retest reliability for PPT ranged from 0.85 to 0.90 (intra-class correlation coefficients)13.
Statistical analysis
We evaluated the relation of the 4 PFOA categories (based on PF symptoms and MRI PFOA as defined above) to the outcomes of interest using logistic regression for those outcomes that were dichotomous (presence of depressive symptoms, pain catastrophizing, and TS). The referent group in all analyses was the group with no PF symptoms or MRI PFOA (no PFOA). Because PPT ranges differ among men and women27, the mean PPT for each of the 4 categories was assessed separately for males and females using linear regression. All analyses were adjusted for age, sex (except for PPT analyses), body mass index (BMI), and MRI features of TFOA (presence of full-thickness cartilage lesions, presence of 1 marrow lesion). Sensitivity analyses were performed, where groups were collapsed into those with and without PF pain (irrespective of the presence or absence of MRI features). Analyses were performed using SAS (version 9.4, SAS Institute Inc.).
RESULTS
There were 1112 participants [713 (64%) females] included in the current study (Figure 1). The mean (SD) age was 66.8 (7.6) years, and BMI was 29.5 (4.8) kg/m2. Participant characteristics are presented in Table 1.
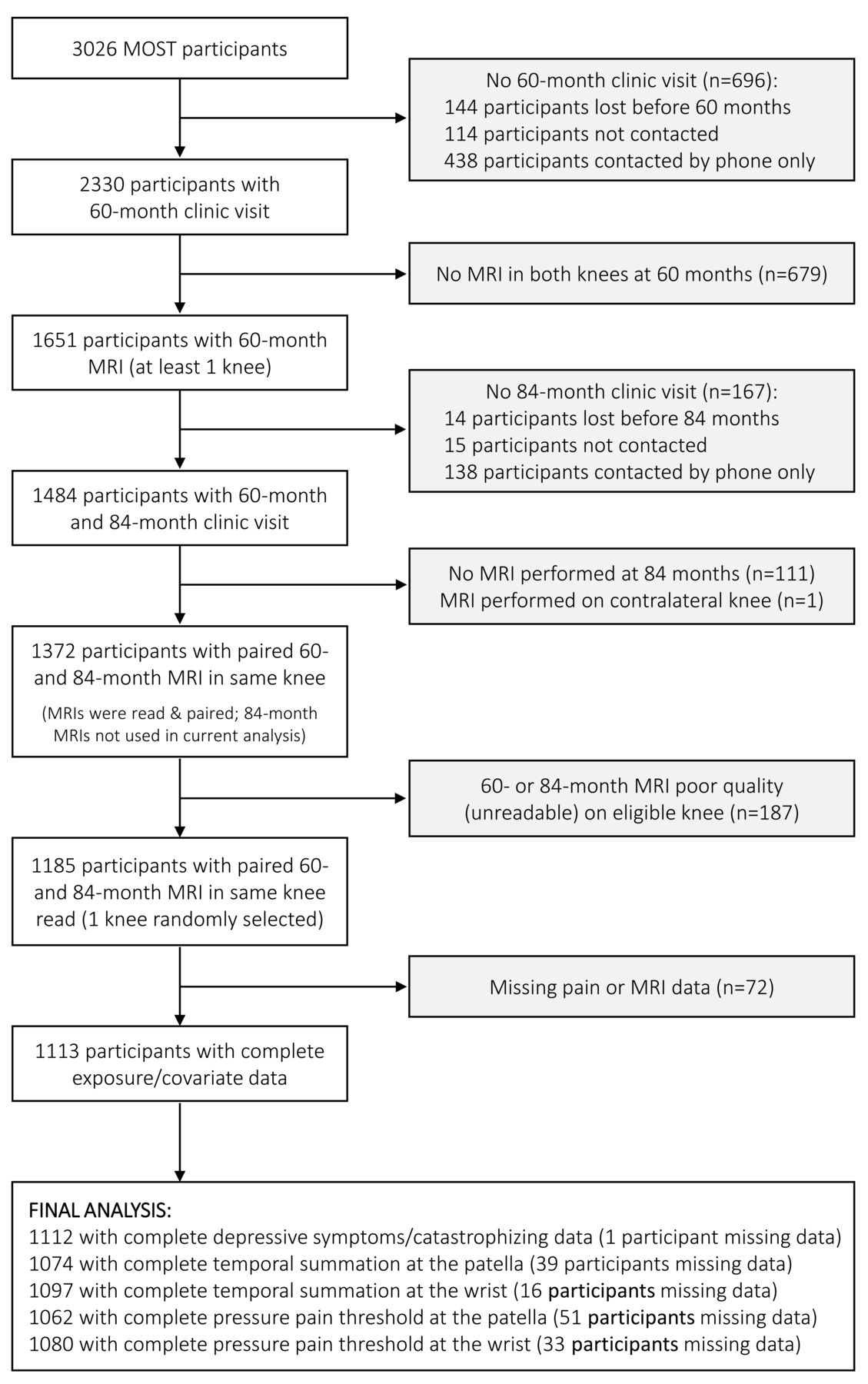
Flow chart of participants included in the analysis. MOST: Multicenter Osteoarthritis Study; MRI: magnetic resonance imaging.
Participant characteristics.
Psychological variables
Compared with the reference group (no PFOA), those with PF symptoms with MRI PFOA had significantly greater odds of having depressive symptoms (OR 2.01, 95% CI 1.13–3.56; Figure 2; Supplementary Table 1, available with the online version of this article). Participants with PF symptoms (no MRI PFOA) also had significantly greater odds of depressive symptoms (OR 1.79, 95% CI 1.04–3.09) compared with the reference group. Participants who had MRI PFOA but no symptoms were not significantly different than the reference group.

Adjusted OR (95% CI) for (A) the CES-Depression Scale (black diamonds) and catastrophizing item of the CSQ (white diamonds); and (B) TS at the patella (black diamonds) and wrist (white diamonds), for each PFOA group (adjusted for age, sex, BMI, tibiofemoral OA; reference group = no pain or MRI OA). CES: Center for Epidemiological Studies; CSQ: Coping Strategies Questionnaire; BMI: body mass index; MRI: magnetic resonance imaging; OA: osteoarthritis; PF: patellofemoral; PFOA: patellofemoral OA; TS: temporal summation.
For pain catastrophizing, those with PF symptoms with MRI PFOA (OR 1.5, 95% CI 1.03–2.19) and those with PF symptoms alone (OR 1.79, 95% CI 1.26–2.54) had significantly greater odds of pain catastrophizing compared with the reference group (Figure 2; Supplementary Table 1, available with the online version of this article). There was no significant difference in odds of pain catastrophizing for participants with MRI PFOA without PF symptoms and the reference group.
QST
Compared with the reference group (no PFOA), participants with PF symptoms with MRI PFOA had significantly greater odds of demonstrating TS over the patella (OR 1.71, 95% CI 1.15–2.53), but not at the wrist (Figure 2; Supplementary Table 1, available with the online version of this article). Participants with PF symptoms only (no MRI PFOA) had significantly greater odds of demonstrating TS at both the patella (OR 1.96, 95% CI 1.37–2.80) and the wrist (OR 1.66, 95% CI 1.16–2.37). There were no significant differences in odds of TS for those with MRI PFOA alone (no PF symptoms).
Group means and 95% CI for PPT at the patella and wrist are presented in Figure 3 and Supplementary Table 2 (available with the online version of this article), stratified by sex. Males with PF symptoms only (no MRI PFOA) had significantly lower PPT at the patella compared to those with MRI PFOA only (mean difference −1.32 kg/cm2, 95% CI −2.43 to −0.22) and those with no PFOA (mean difference −1.37 kg/cm2, 95% CI −2.36 to −0.38). There were no significant differences in PPT at the wrist. For females, there were no significant between-group differences at the patella or wrist.

Adjusted means (95% CI) for PPT at the patella (black diamonds) and wrist (white diamonds), for each PFOA group, stratified by sex (adjusted for age, body mass index, tibiofemoral OA). OA: osteoarthritis; PF patellofemoral: PFOA: patellofemoral OA; PPT: pressure pain threshold.
Sensitivity analyses
Compared to those without PF symptoms (regardless of MRI PFOA status), those with PF symptoms (also regardless of MRI PFOA status) had 2.12 (95% CI 1.38–3.27), 1.55 (1.18–2.03), 1.53 (1.16–2.03), and 1.92 (1.45–2.54) times the odds of having depressive symptoms, catastrophizing, TS at the wrist, and TS at the patella, respectively.
Males with PF symptoms had significantly lower PPT at the patella compared to those without symptoms (mean difference −0.92 kg/cm2, 95% CI −1.52 to −0.31), but differences were not significant at the wrist (mean difference −0.39 kg/cm2, 95% CI −0.8 to 0.03). There were no significant differences between females with and without PF symptoms for PPT at the patella (mean difference −0.21 kg/cm2, 95% CI −0.51 to 0.09) or wrist (mean difference −0.06 kg/cm2, 95% CI −0.24 to 0.12).
DISCUSSION
We found that people with PF symptoms, with or without MRI PFOA, had greater odds of depressive symptoms, pain catastrophizing, and local mechanical TS, compared to people without PF symptoms or MRI PFOA. Those with PF symptoms only (no MRI PFOA) also had greater odds of mechanical TS at the wrist compared to people with no PFOA. We found sex-specific between-group differences for PPT. Males with PF symptoms only (no MRI PFOA) had significantly lower PPT at the patella compared to those with MRI PFOA only, and compared to those with no PFOA, although no differences were found at the wrist. However, no significant between-group differences in PPT were found for females.
Taken together, our findings demonstrate the presence of psychological impairment, local hyperalgesia, and symptom amplification in people with symptomatic features of PFOA, as well as more widespread symptom amplification. This is irrespective of whether structural PFOA (defined as a full-thickness cartilage lesion with BML in the PF joint) is present on MRI, particularly as those with PF symptoms only (without MRI PFOA) demonstrated findings consistent with sensitization. This suggests that it is PF symptoms and not structural changes that are largely associated with the presence of these features. Our findings in PFOA are consistent with those of Neogi, et al13, who evaluated TS and PPT in people with radiographic TFOA (with or without PFOA) in the same MOST cohort. The relevance of imaging features of OA in the knee has been questioned by multiple studies, given the discordance between structural features and symptoms of pain and function28. The literature is characterized by studies that both support and negate a relationship between MRI OA and pain29, while studies also highlight that a large proportion of asymptomatic people have features of knee OA on radiograph and MRI30. Nevertheless, our findings highlight the primary importance of the symptoms of PFOA, as well as their consideration in the assessment and management of patients.
Although depressive symptoms and catastrophizing have not been previously identified in PFOA, our findings regarding these characteristics are consistent with previous studies in similar musculoskeletal populations. Depressive symptoms have been identified in knee OA and PF pain populations10–12. Catastrophizing has been demonstrated in younger adults with PF pain11. While the cross-sectional nature of our study precludes inference of causality, our findings do suggest that psychological impairments are present in people with symptomatic features of PFOA. It is important that health professionals who manage people with PFOA are cognizant of this, and refer for appropriate management as indicated. It is also important for future studies to establish whether there are other psychological characteristics associated with this population, such as anxiety and kinesiophobia10.
Within our cohort, individuals with PF symptoms also demonstrated increased TS at both local and remote sites. While it is logical that local TS would be associated with the presence of pain locally at the knee, particularly a chronic pain condition such as PFOA, increased TS at a remote site (the wrist) may suggest central sensitization, though we did not find differences in hyperalgesia at the wrist. Our findings suggest that TS and PPT provide different information and that TS may be a characteristic of the individual (i.e., trait), rather than a result of the presence of PFOA pain (state), consistent with conclusions of Neogi, et al13.
It is not surprising that local hyperalgesia was present in our cohort, as it is a feature in people with knee OA14 and those with PF pain15,16. What is novel is that we found that this was only the case in males and not females, to our knowledge. Males with PF symptoms only had significantly lower PPT over the patella, even when compared to those with combined PF symptoms and MRI PFOA. The reasons for this are unclear but do reinforce that it is symptoms driving observed differences, rather than structure13. This raises the question that reported between-group differences in PPT observed in prior studies are related to sex, which has not previously been considered separately. This may explain the findings of Bartholomew et al17, who reported no differences in PPT between a mixed-sex cohort of people with PFOA and controls. Because of differences in PPT between sexes27, we considered male and female PPT separately. Sex-specific subgroups of PFOA should be explored further in future studies evaluating pain sensitization.
Our findings provide important preliminary information regarding psychological factors and pain sensitization in older adults with symptoms of PFOA, which might plausibly influence the management of people with PFOA and inform the design of future studies. Most notably, our findings suggest that psychological and pain characteristics should be considered when assessing and managing people with PFOA. Assessment of pain sensitization may help consider further mechanism-based management approaches as more treatments become available. Exploration of how psychological characteristics and pain sensitization are associated with and are predictive of symptoms and function in those with PFOA is warranted to gain prognostic insights and further support for consideration of pain phenotyping. Finally, given our findings that depressive symptoms, pain catastrophizing, and pain sensitization are related to PF symptoms, these factors should be investigated for their ability to predict treatment response.
Inferences from this study should be made, bearing in mind some potential limitations. Although we diagnosed PFOA using consensus-based criteria available in the MOST cohort, diagnosis of PFOA would typically involve additional criteria (e.g., crepitus, physical examination to exclude other sources of knee pain)1,8,9. The MOST cohort consists of older adults with, or at risk of, knee OA, who present with particular characteristics (e.g., high BMI). Thus, the findings of this study may not apply to younger adults with PFOA or those with lower BMI. Further, there were limitations regarding the specific variables available. For example, our evaluation of psychological variables was limited to depressive symptoms and pain catastrophizing. Based on findings in knee OA and younger adults with PF pain, evaluation as to whether other psychological characteristics such as anxiety and fear of movement are also features of PFOA is warranted. We also acknowledge that there are multiple ways in which MRI PFOA can be defined. From systematic review findings highlighting the high prevalence of individual structural features (e.g., cartilage lesions, BML) in asymptomatic people30, we chose to define PFOA as the combination of a full-thickness cartilage lesion with coexisting BML23. This was based on our previous findings in 26- to 50-year-old adults with persistent PF pain, where we found a high prevalence of partial-thickness lesions and osteophytes in pain-free controls, and that PFOA defined as combined full-thickness cartilage lesion with a BML was better able to differentiate PF pain from controls3. However, we acknowledge that other features of PFOA may be related to symptoms (e.g., synovitis, effusion), which should be explored in future studies.
In conclusion, people with PFOA symptoms, with or without structural features of PFOA, are more likely to demonstrate psychological impairments (depressive symptoms, catastrophizing) and pain sensitization (TS), compared with asymptomatic people with no MRI PFOA. Sex-specific differences were observed for PPT. Further exploration of how psychological characteristics and pain sensitization are associated with and are predictive of symptoms and function in those with PFOA is warranted.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
A. Guermazi is the President and shareholder of Boston Imaging Core Lab (BICL), LLC, and consultant to Pfizer, Merck Serono, GE, TissueGene, OrthoTrophix, AstraZeneca, and Sanofi. F. Roemer is a Chief Medical Officer and shareholder of BICL, LLC.
The Multicenter Osteoarthritis Study was funded by the National Institutes of Health (NIH; U01-AG18820, U01-AG18832, U01-AG18947, U01-AG19069, and AR-47785). J. Stefanik was supported by NIH/NIGMS U54-GM104941 and K23-AR070913. T. Neogi was supported by K24-AR070892, P60-AR047785, and R01 AR062506. N. Collins was supported by an Arthritis Queensland Fellowship (2018) and The University of Queensland Postdoctoral Fellowship (2015–17).
- Accepted for publication January 14, 2020.








{kind=link}
{kind=link}
{kind=link}