

Abstract
Objective The aim of this study was to evaluate the prevalence, type of neuropathy, and the relationship between the presence of autoantibodies and neuropathy development in patients with primary Sjögren syndrome (pSS).
Methods Sixty-one patients with pSS underwent a complete neurological and electrophysiological examination as well as immunological tests including rheumatoid factor (RF) and autoantibodies such as antinuclear antibodies (ANA), anti-Ro/SSa, and anti-La/SSB antibodies.
Results The axonal loss or demyelination were found in 39 patients (63.9%). Twenty-nine (47.5%) subjects fulfilled both clinical and electrophysiological criteria of peripheral neuropathy of predominantly axonal type. Seropositivity to both anti-Ro and anti-La antibodies was more frequently found in patients with normal nerve conduction study. Seropositivity to anti-Ro alone was present in the majority of patients with axonal neuropathy (P < 0.05). The presence of RF was associated with several electrodiagnostic signs of demyelination (P < 0.01). The ANA titer showed no independent association with neuropathy.
Conclusion Peripheral neuropathy is a frequent complication in patients with pSS. Seropositivity limited to anti-Ro is associated with increased risk of axonal neuropathy in comparison to seropositivity to both anti-Ro and anti-La antibodies. Seropositivity to RF may contribute to demyelination.
Primary Sjögren syndrome (pSS) is an autoimmune connective tissue disease affecting the exocrine glands, leading to the damage of their structure and impairment of their function. In the course of pSS, internal organs may also be involved, and symptoms associated with every system may occur. Neurological complications account for 8.5–70% of pSS cases1. Peripheral neuropathy, especially the distal sensory or sensorimotor axonal neuropathy, is the most frequent neurological complication of pSS (2–60%)2,3,4,5,6,7. Cranial neuropathy and central nervous system involvement (2–25%) were also reported in the course of pSS8,9,10.
Although the clinical presentation of peripheral neurologic pathologies in pSS were extensively described, the clear underlying pathogenic mechanisms are still not well known. One of the highlighted causes of neuropathy in pSS is vasculitis, which is especially associated with development of mononeuropathy multiplex. The multifocal T cell infiltration in the dorsal root ganglia seems to be responsible for the development of sensory neuronopathy. B cell hyperactivity and the production of autoantibodies have been also considered as candidate contributors to nerve damage owing to their reactivity against nerve tissue antigens11,12,13. Data concerning the immunological profiles of patients with pSS and concomitant neuropathy are sparse and up for debate. One study showed that patients with pSS-associated sensory neuropathy had a higher prevalence of both anti-Ro and anti-La antibodies5,14,15,16. However, in other studies, neuropathies were associated with a negative immunological profile17,18. Moreover, despite many epidemiological studies, there are inconsistencies in the prevalence of neuropathy associated with pSS in different centers. The cause of such discrepancies is linked with different definitions of peripheral neuropathy, and the fact that the definition is not always based on objective clinical and electrophysiological criteria. Some studies relied more on neurological and electrophysiological testing, whereas others depended entirely on symptomatology as reported by patients themselves. Moreover, electrophysiological studies were sometimes limited and insufficient.
The main aim of our study was to evaluate the prevalence and the type of peripheral neuropathy in patients with pSS. The secondary purpose was to assess the relationship between specific immunologic profiles regarding the presence of serologic markers significant for patients with pSS, such as rheumatoid factor (RF), antinuclear antibodies (ANA), anti-Ro, anti-La antibodies, and neuropathy development.
MATERIALS AND METHODS
Patients
Sixty-one patients aged 21–80 yrs (mean 50.82, SD 14.01), including 56 women aged 21–80 years (mean 51.05, SD 14.64) and 5 men aged 35–55 years (mean 48.20, SD 7.73) with pSS diagnosed between September 2014 and June 2016 in the National Institute of Geriatrics, Rheumatology and Rehabilitation (NIGRiR) were enrolled. All patients fulfilled the diagnostic criteria for pSS proposed both by the American-European Consensus Group and by the American College of Rheumatology in 201219.The study was approved by the Ethics Committee of NIGRiR (nr KBT-1/1/15), and signed informed consent forms were obtained from all patients.
We excluded patients with secondary SS and with comorbidities potentially affecting the peripheral nervous system, such as diabetes mellitus, glucose intolerance, renal failure, hyperthyroidism or hypothyroidism, proliferative diseases, amyloidosis, sarcoidosis, hepatitis C and hepatitis B infections, alcohol abuse, vitamin B12 deficiency, and exposure to neurotoxic factors.
Serology
In the course of diagnostics, basic laboratory tests were performed, including RF and autoantibodies (ANA, anti-Ro/SSa, anti-La/SSB). ANA were detected by indirect immunofluorescence using HEp-2 as an antigen. The anti-Ro/SSA and anti-La/SSB antibodies were evaluated using the semiquantitative method (by Euroimmun with EUROblotOne analyzer, EUROIMMUN US Inc.). The RF was measured using nephelometric assay (normal range < 34 IU/mL).
Neurological assessment
All patients underwent a complete neurological examination. Muscle strength was assessed according to the Medical Research Council scale. Examination included the strength of distal and proximal muscles of upper and lower extremities. Patients performed the following movements against resistance: shoulder abduction, elbow flexion and extension, finger flexion and extension, hand grip, hip flexion and extension, knee flexion and extension, as well as foot flexion and extension. Sensory examination was based on assessment of light touch, pinprick, temperature sensations, and deep sensation (joint position sense, presence of sensory ataxia and Romberg sign, vibratory sensation). Vibration was quantified using a Rydel-Seiffer tuning fork bilaterally at the distal interphalangeal joints, medial malleolus, and radial styloids. Cranial nerve function, deep tendon reflexes, and pathological reflexes were also assessed. In patients reporting symptoms suggestive of the carpal tunnel syndrome (CTS), we looked for Tinel sign and we performed Phalen test.
Nerve conduction study
All patients underwent nerve conduction studies, even if their neurological examination was normal. The electrodiagnostic examinations (EDX) were done in the Electromyography Laboratory of NIGRiR using a Neuropack X1 MEB-2300 system (Nihon Kohden). Nerve conduction studies were performed bilaterally using surface electrodes. Standard sites of stimulation and recording response from individual nerves were used, based on commonly adopted methodology20. Motor conduction studies involved the median, ulnar, peroneal, and tibial nerves. Sensory conduction studies were performed in the median, ulnar, superficial peroneal, and sural nerves. Stimulation in multiple sites was done in ulnar neuropathy at the elbow but not in other entrapment neuropathies. For the motor nerve conduction study (NCS), low frequency filter was set to 2 Hz and high frequency filter to 10 kHz. The sweep speed was set at 5 ms, the gain (sensitivity) was set at 2 mV per division for tibial and peroneal nerve, and at 5 mV for median and ulnar nerve. Distal latency, amplitude, conduction velocity, and the F wave latency were measured. For sensory conduction studies, low frequency filter was set to 30 Hz and high frequency filter to 2 kHz; the gain (sensitivity) was set at 10 µV per division, the sweep speed was set at 2 ms. Amplitude of sensory nerve action potential (SNAP) and conduction velocity were measured. The amplitude of both compound muscle action potential (CMAP) and SNAP was measured from the baseline to the negative peak. If the amplitude was low, the sensitivity was increased. Demyelination or axonal loss were diagnosed according to the criteria of the ESTEEM project (European Standardized Telematic tool to Evaluate Electrodiagnostic Methods)21. The presence of conduction block was recognized using guidelines of the American Association of Neuromuscular & Electrodiagnostic Medicine22.
Based on electrophysiologic findings, mononeuropathy, mononeuropathy multiplex, or polyneuropathy were diagnosed. For mononeuropathy multiplex, involvement of at least 2 nerves was required with concomitant pain and subacute onset. For diagnosis of polyneuropathy, the respective electrodiagnostic criteria20 needed to be fulfilled and an additionally chronic, progressive pattern needed to be documented clinically or electrophysiologically. Electrodiagnostic criteria cited above required prolongation of the distal motor latency and/or motor conduction velocity slowing in at least 2 separate nerves and/or decrease in the amplitude of the sensory nerve action potential, or a decrease in sensory conduction velocity in at least 2 separate nerves.
Owing to distinct pathogenic mechanism, entrapment neuropathies were analyzed separately. Symptomatic neuropathy was diagnosed on the basis of abnormalities in both neurological examination and electroneurography. The time interval separating serologic workup and NCS did not exceed several days.
Statistical analysis
IBM SPSS Statistics Software, version 24 (IBM Corp.) was used to perform the whole statistical analysis. To determine distribution of quantitative variables, the Kolmogorov–Smirnov test was used. The relationship between particular variables of nerve conduction to age, titer of particular antibodies, as well as other numeric variables, was analyzed with Pearson correlation coefficient or in case of non-normal data, distribution with the Spearman rank correlation coefficient. For variables of nerve conduction significantly correlating with age, analysis with other variables was controlled for age using partial correlations. Logistic regression analysis, also controlled for age, was used to investigate the influence of RF positivity and concentration, ANA titer, anti-La positivity, and concurrent anti-La positivity in the anti-Ro positive subgroup (independent variables) on clinical signs of neuropathy and nerve conduction study parameters (dependent variables). Data are presented as means and SD. Significance level was set at P < 0.05.
RESULTS
NCS revealed axonal loss or demyelination in 39 out of 61 patients (63.9%). Twenty-nine (47.5%) subjects fulfilled both clinical and electrophysiological criteria of peripheral neuropathy. In the vast majority of patients, neurography showed axonal damage, which was present in 37 subjects (94.8% of all subjects with neuropathy). In 2 patients (5.1% of all subjects with neuropathy), axonal loss was accompanied by demyelination (Table 1). Neuropathy affected predominantly nerves of lower extremities and sensory fibers in 28 subjects (71.8% of all subjects with neuropathy). In 15 cases (38.5% of all subjects with neuropathy), only sensory nerves were affected. Regarding the number of affected fibers, the most frequent diagnosis was polyneuropathy, which was found in 16 patients (41% of all patients with neuropathy); in 10 patients (25.6% of all patients with neuropathy) it was sensorimotor polyneuropathy; and in 6 patients (15.4% of patients with neuropathy) it was sensory polyneuropathy. Fourteen patients (35.9% of all patients with neuropathy) revealed mononeuropathy, most often of the peroneal nerve, and 9 patients (23% of all patients with neuropathy) revealed mononeuropathy multiplex (Table 1). Moreover, in 18 patients (29.5%) a compression neuropathy was found, usually concomitant to axonal peripheral neuropathy. In 12 (19.7%) patients, it was CTS, with 4 (6.5%) as an isolated finding. In 7 patients (11.5%), we found ulnar neuropathy at the elbow, which in 1 (1.6%) was an isolated electrodiagnostic abnormality.
Types of neuropathy according to nerve conduction study.
Seventeen patients reported symptoms typical for neuropathic pain. The most frequent form was burning feet, which was present in 14 patients, suggesting involvement of small fibers. In 4 of these patients the nerve conduction was normal, which indicates the pure small fiber neuropathy; all 4 patients were ANA-positive. In one of them no other seropositivity was found. The second one was also anti-Ro–positive, the third anti-Ro– and anti-La–positive, and the fourth anti-Ro–, anti-La–, and RF-positive. However, the diagnosis of small fiber neuropathy could not be confirmed as the skin biopsy was not performed. Four patients complained about facial pain (1 patient describing symptoms typical for trigeminal neuralgia), and in 5 patients pain was located also in the trunk as well.
Involvement of the cranial nerves assessed by neurological examination was detected in 7 patients (11.5%). The most frequent was a pure sensory trigeminal neuropathy (V nerve); in 5 patients (1 patient with numbness restricted to the trigeminal nerve region, 4 patients with trigeminal neuralgia). The vestibulocochlear nerve (VIII nerve) impairment, revealed by unilateral hearing loss, was found in 2 patients. Cranial neuropathies usually coexisted with other types of neuropathies (most frequently with sensory polyneuropathy). There was only 1 case in which trigeminal neuropathy was found as an isolated abnormality.
Presence of antibodies
RF was found in 27 patients (44.3%). The concentration of RF ranged from 20 to 1515 IU/mL[mean 29.15, interquartile range (IQR) 139.75; mean 134.08, SD 251.11]. ANA antibodies (in titer > 1:160) were detected in 57 patients (93.4%). In a titer of > 1:320, ANA antibodies were found in 51 patients (83.6%). The titer of ANA antibodies ranged from 1:80 to 1:40,960 (mean 1280, IQR 2240; mean 1:2790.82, SD 1:6013.96).
Anti-Ro/SSA–specific antibodies were found in 51 patients with pSS (83.6%) and anti-La/SSB–specific antibodies were found in 23 patients (37.7%). Among 61 patients, 29 (47.5%) had only anti-Ro antibodies (without anti-La antibodies), and 22 (36.1%) had antibodies directed against both Ro and La. Only 1 patient was found to have anti-La antibodies in the absence of anti-Ro antibodies (Figure 1).

Percentage distribution of incidence of anti-Ro and anti-La antibodies in the studied group.
Antibodies and neuropathy
The chi-square test revealed a statistically significant relationship between axonal nerve damage and the presence of anti-Ro/SSA or both anti-Ro/SSA and anti-La/SSB antibodies [chi-square (1) = 4.56, P < 0.05]. Seropositivity to both anti-Ro and anti-La in the same subject was more frequently found in patients with normal NCS (12/22 patients with both anti-Ro and anti-La compared to 7/22 patients with anti-Ro). Seropositivity to anti-Ro alone was present in the majority of patients with axonal neuropathy (21/37 patients with anti-Ro compared to 10/37 patients with both anti-Ro and anti-La; Figure 2).
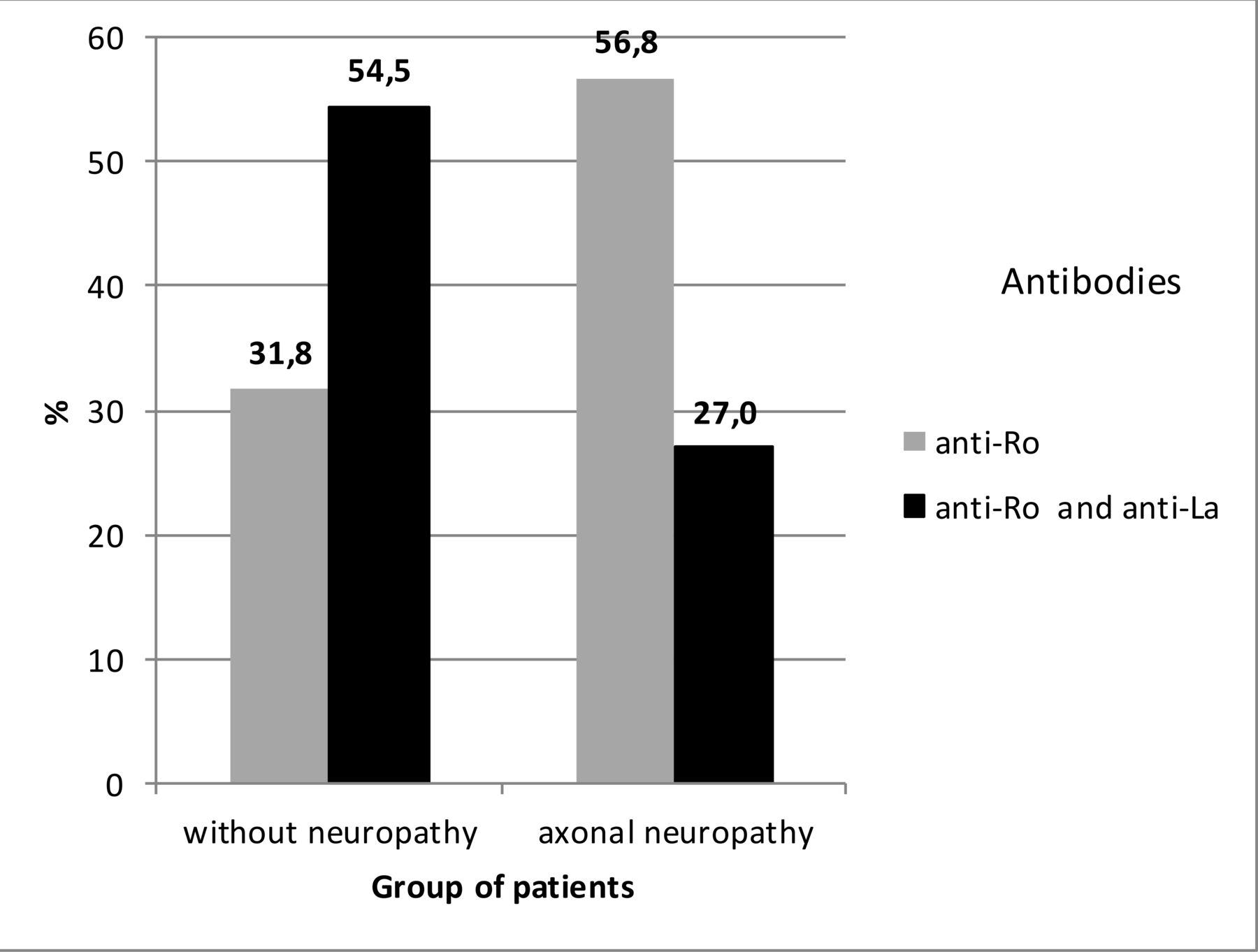
Percentage distribution of incidence. Presence of anti-Ro antibodies and coexistence of anti-Ro and anti-La antibodies in the group of patients without neuropathy and in the group with axonal neuropathy.
Mean ANA titer was higher in patients without neuropathy (P < 0.05) and correlated negatively with age. Using partial correlation analysis under age control, we found that the age is the main risk factor of developing of neuropathy, and ANA titer does not influence nerve conduction independently.
There were 4 patients with clinical signs of peripheral neuropathy and no detectable autoantibodies. One of them showed in NCS sensory axonal polyneuropathy and other 3 sensorimotor axonal polyneuropathy.
We found a significant correlation between age and the NCS. The age correlated with the prolongation of the distal motor and F wave latencies of the median and ulnar nerve, and with the amplitude decrease of CMAP and SNAP of the median nerve and the peroneal nerve, reduced amplitude of the CMAP of the tibial nerve, and reduced amplitude of the SNAP of the ulnar and sural nerve (P < 0.01). The age correlated negatively with the motor conduction velocity of the median, ulnar, peroneal nerve, and sensory conduction velocity of the median, ulnar, sural, and peroneal nerve (P < 0.01 or P < 0.05; Table 2).
Significant correlation between age and nerve conduction.
Using partial correlation analysis under age control, we found that the association of antibodies with the NCS was limited to only a few conduction variables in some nerves. We found statistically significant negative correlation between the presence of RF and ulnar motor conduction velocity at the forearm (r = −0.353, P < 0.01), and statistically significant positive correlation between the presence of RF and F wave latency in the tibial nerve (r = −0.349, P < 0.01). The presence of anti-La antibodies correlated positively with the amplitude of CMAP of the median nerve (r = 0.300, P < 0.05). An inverse correlation was found between co-occurrence of anti-Ro and anti-La antibodies and distal motor latency of the peroneal nerve (r = −0.334, P < 0.05).
DISCUSSION
In the presented cohort, NCS revealed axonal loss or demyelination in many patients with pSS. The prospective character and vast electrophysiological diagnostics used in our investigations yielded a prevalence of neuropathy in pSS comparable to the upper limit of the range of the previously published results (2–60%)2,3,4,5,6,7 and markedly higher than the data for the general population, which varies between 2.4 to 8%23.
In the vast majority of patients, neurography showed axonal damage and affected predominantly nerves of lower extremities and sensory fibers. Delalande, et al17, Pavlakis, et al24, Gono, et al25, Brito-Zerón, et al26, Mori, et al27, and Jamilloux, et al28 also emphasized the predominance of axonal type of neuropathy in patients with pSS.
Described results confirmed that age was negatively associated with the sensory as well as the motor conduction. Previous studies also demonstrated age-related slowing of nerve conduction velocity and reduction in nerve response amplitude in the general population29,30. On the other hand, our current study underlines that the frequency of peripheral neuropathy is significantly higher in patients with pSS compared to the general population, which indicate that neuropathy have to be associated with this disease.
In our present study, ANA antibodies in titers over 1:320 were found in 83% of patients with pSS. Previous studies show that ANA is the antibody most frequently detected in pSS16. Using partial correlation analysis under age control, we found that ANA titer does not influence nerve conduction independently. This result is quite different from the Sène, et al7 study, where patients with nonataxic sensory neuropathies were characterized by a lower prevalence of ANA compared to patients without neuropathy. They did not notice this relationship between the prevalence of ANA and sensorimotor neuropathy. In the same study, patients with nonataxic sensory neuropathy were older compared to the patients without neuropathy. It can be assumed that the relationship between ANA seronegativity and sensory neuropathy described by Sène, et al7 may become insignificant if they had used partial correlation analysis under age control.
We found that the presence of RF correlated positively with F wave latency in the tibial nerve, and inversely with ulnar motor conduction velocity at the forearm. Seropositivity to RF is probably associated with demyelination, but RF concentration does not influence the nerve conduction variables. Indeed, we did not observe any relationship between clinical signs of neuropathy and RF. Our results are consistent with those of Jamilloux, et al28, where the presence of RF did not influence neurological manifestations in patients with pSS. Ramos-Casals, et al16 also did not confirm the association between RF and neuropathy. Similarly, Bharadwaj and Haroon31 reported no relationship between RF and extraarticular manifestations of rheumatoid arthritis (RA). On the other hand, Biswas, et al32 noticed that RF-positive patients with RA had a higher frequency of neuropathy.
The subset of patients with fully normal NCS had the highest prevalence of both anti-Ro and anti-La antibodies, whereas patients with axonal neuropathy were seropositive to only anti-Ro antibodies. This result is consistent with the previous studies about systemic lupus erythematosus, where patients with both anti-Ro and anti-La antibodies have been shown to have a lower risk of nephritis and seizures than those with anti-Ro antibodies alone33. The opposite results regarding a prevalence of anti-Ro and anti-La antibodies in pSS patients were reported by Jamilloux, et al28, Sène, et al7, and Scofield, et al34. Jamilloux, et al28 found that patients with neuropathy, both sensorimotor and sensory, had lower prevalence of anti-Ro antibodies compared to those without neuropathy. Sène, et al7 found that patients with sensory neuropathies were characterized by a lower prevalence of anti-Ro and anti-La antibodies compared to patients without neuropathy. In the same study, patients with sensory neuropathy were older than patients without neuropathy. Sène, et al7 did not use partial correlation analysis under age control, which could show that the age was the highest risk factor of neuropathy. They did not compare patients positive to both anti-Ro and anti-La antibodies to those with only anti-Ro antibodies. Scofield, et al34 found that patients with both anti-Ro and anti-La antibodies were much more likely to have neuropathy than those with anti-Ro antibodies alone. The association of anti-Ro and anti-La antibodies was most robust when these antibodies were determined by double immunodiffusion. Their data suggest that the method of detection can be the reason for different results obtained from previous studies. Different results obtained by Scofield, et al34, could also be a result of limiting the diagnosis of neuropathy to clinical evaluation without electrophysiologic assessment.
The main limitation of this study was the suboptimal EDX approach lacking examination with needle electrode, which could detect coexistent myopathic or subtle neurogenic changes that do not result in abnormalities in the NCS. However, the data from previous studies did not show a significant relation between pSS and myopathy. The neurogenic changes have low specificity, especially in an older population and could be hardly pathophysiologically attributed to pSS when there were no healthy controls. We therefore believe that additional electromyography would not change our results significantly. The second limitation is the lack of skin biopsy, which might reveal neuropathy of small fibers in our patients with otherwise no objective signs of polyneuropathy.
Peripheral neuropathy is a frequent complication in pSS, especially in older patients. Most frequently, an axonal form of neuropathy affecting predominantly lower extremities and sensory fibers is observed. Seropositivity limited to only anti-Ro antibodies is associated with increased risk of axonal neuropathy, whereas seropositivity to both anti-Ro and anti-La antibodies may be associated with lower incidence of neuropathy. The ANA titer probably does not influence nerve conduction independently. Seropositivity to RF may contribute to demyelination, but with a weak effect. Humoral immune response in pSS probably damages peripheral nerves, but this effect is mediated by still-unrecognized mechanisms as the routinely tested antibodies cannot be used as a marker of neuropathy. An extensive NCS is still the most reliable method of detecting early peripheral neuropathy in pSS. We recommend performing electrophysiologic tests in all patients with pSS, even those without clinical signs of neuropathy.
- Accepted for publication February 7, 2020.








{kind=link}
{kind=link}