

Abstract
Objective. Reactive arthritis (ReA) is a spondyloarthritis triggered by a bacterial infection. In cases where nonsteroidal antiinflammatory drugs and conventional synthetic disease-modifying antirheumatic drugs have failed, biologics such as tumor necrosis factor inhibitors (TNFi) have been used. However, limited evidence exists of the efficacy and safety of these drugs in ReA. We report on Icelandic patients with ReA who have been treated with TNFi, their characteristics, outcomes, and safety.
Methods. We conducted an observational cohort study using the Icelandic nationwide database of biologic therapy (ICEBIO) supplemented with a retrospective study of electronic health record (EHR) data. Drug efficacy was assessed using disease activity scores and standardized questionnaires within ICEBIO; safety was assessed using ICEBIO and EHR data.
Results. Thirty-eight patients with ReA were registered in the database. Eight were given TNFi within 1 year of symptom onset. At 6 and 18 months, there was a significant reduction in C-reactive protein (CRP), tender and swollen joints, visual analog scale for pain and fatigue, 28-joint count Disease Activity Score 28 based on CRP, Clinical Disease Activity Index, and Health Assessment Questionnaire scores. Seventy-one to 90% of patients were considered treatment responders. Two patients were able to stop biologics owing to remission. During the 303 patient-years (mean 8, range 1–15) biologics were given, 6 hospital admissions for infections were noted.
Conclusion. TNFi are safe and effective in ReA, but treatment tends to be prolonged. Further clinical trials are urgently needed in ReA.
Reactive arthritis (ReA) is an inflammatory disease arising 1 to 4 weeks following a bacterial infection, most commonly of the genitourinary or gastrointestinal tracts. It is classified with the HLA-B27–associated spondyloarthritides (SpA) along with axial SpA (axSpA), psoriatic arthritis (PsA), and inflammatory bowel disease–associated arthritis. ReA commonly causes oligo- or polyarthritis, mainly of the lower limbs but also extraarticular disease, such as enthesitis, conjunctivitis, and uveitis, as well as symptoms of inflammatory back pain that may result in SpA1,2. The term reactive arthritis represents a spectrum of postinfectious arthritis. Thus, this classic triad of arthritis, conjunctivitis, and urethritis (formerly known as Reiter syndrome) is present only in a subset of patients3. While ReA is often perceived as mild and self-limiting, a substantial percentage of patients develops chronic inflammatory disease. Indeed, ReA follows a chronic course in up to one-third of patients4,5.
Although treating the acute infection with antibiotics seems to lower the likelihood of developing ReA6, once the disease is established, there generally is no further role for antibiotic treatment7,8,9, with the possible exception of Chlamydia-induced ReA10,11. The first-line treatment of ReA is with nonsteroidal antiinflammatory drugs (NSAID) and local intraarticular steroid injections. Glucocorticoids and conventional synthetic disease-modifying antirheumatic drugs (csDMARD), such as sulfasalazine (SSZ) and methotrexate, are used in severe or resistant cases12. SSZ has been shown to induce remission when started within 3 months13 and is effective in chronic ReA14. High levels of tumor necrosis factor (TNF)-α in the circulation and the affected joints of patients with ReA have prompted the use of anti-TNF agents in disease unresponsive to standard treatment15. Because of the theoretical risk of reactivating the triggering infection, Flagg, et al16 examined synovial biopsies and clinical response in 10 ReA patients treated with the TNF inhibitor (TNFi) etanercept (ETN). Of note, even those with PCR evidence of bacterial organisms on biopsy before treatment showed clinical improvement.
Few studies have been published on the outcome of patients with ReA receiving TNFi. Meyer, et al17 and Flagg, et al16 each reported 10 patients with ReA receiving TNFi. In both trials, 9 patients responded well to therapy. All 15 ReA patients reported by Brinster, et al18 showed clinical improvement on TNFi and one-third were able to discontinue the medication within a few months. Finally, Courcoul, et al19 found that 3 out of 11 patients who had received TNFi for chronic ReA could discontinue the treatment.
The purpose of the present study is to add to the scant evidence of TNFi efficacy and safety in patients with ReA in a larger cohort than earlier reports have presented.
MATERIALS AND METHODS
Data for ReA patients treated with biologic DMARD (bDMARD) were extracted from the ICEBIO registry. ICEBIO is a nationwide registry of Icelandic rheumatologic patients treated with bDMARD that currently includes 98% of this patient group. The registry contains detailed patient characteristics and long-term disease activity scores. The registry was launched in 2007; patients who started biologics earlier were retrospectively entered into the database. ICEBIO is based on the same information technology platform as the Danish Registry DANBIO. ICEBIO has been described in more detail elsewhere20.
Standard demographic data were obtained from the ICEBIO registry at baseline (start of TNFi therapy) as well as information on the type and dosage of TNFi and the dates of symptom onset, diagnosis, and TNFi administration. The following disease activity markers were collected for each office visit: C-reactive protein (CRP), swollen joint count in 28 joints (SJC), tender joint count in 28 joints (TJC), visual analog scale (VAS) for pain and fatigue, 28-joint count Disease Activity Score based on CRP (DAS28-CRP), Clinical Disease Activity Index (CDAI), and Health Assessment Questionnaire (HAQ). Three office visits for assessment of disease activity were chosen: baseline (last visit before starting TNFi), 6 months [closest visit to 180 days (90–210)], and 18 months [closest visit to 540 days (211–660)]. Information on HLA-B27 status was gathered from the National University Hospital’s Blood Bank, the only laboratory that performs HLA typing in Iceland.
A retrospective study of electronic health record (EHR) data was used to gather additional information on the patients found in the ICEBIO registry. This included data on the triggering infection, use of antibiotics, clinical symptoms, antirheumatic treatment before the initiation of TNFi therapy, recurrence of index infection, and serious adverse events during the TNFi treatment period, which were defined as admissions for infections and death. Further safety data were extracted from the EHR if the patients’ ICEBIO data indicated that they stopped or switched biologic agents because of adverse events.
Patients were considered responders if all 3 of the VAS pain, SJC, and TJC decreased by 30% or more (response criteria adapted from Meyer, et al17), or if the DAS28-CRP score decreased by 1 or more disease activity categories: remission < 2.6, low activity ≤ 3.2, moderate activity ≤ 5.1, and high activity > 5.2.
Statistical analysis
All data were anonymized before analysis. Microsoft Excel for Mac version 16.29.1 was used for descriptive analysis. Statistical analysis was performed using R version 3.6.1 in a Linux environment (R Foundation for Statistical Computing). The Kruskal–Wallis test was used to compare variables collected at baseline, 6-month, and 18-month visits. The significance threshold was set at 0.05. Drug survival was demonstrated using a Kaplan–Meier curve.
The study protocol was approved by the Landspitali University Hospital Bioethics Committee (nr 11/2019).
RESULTS
The total number of patients registered with ReA, as the indication for TNFi treatment in the ICEBIO database, was 40. Two of these were excluded because their registry data did not apply to the first biologic medication given for their ReA. Thus, 38 patients remained for data analysis. Twenty-six (68%) were male, and the mean age at the start of bDMARD treatment was 39 years. Thirty-four patients had failed conventional treatment with NSAID and csDMARD prior to initiation of TNFi (data missing for 2 patients; Table 1). The first patient was started on TNFi in 2005 and the last patient in 2018.
Baseline characteristics of 38 patients with reactive arthritis who received treatment with TNF inhibitors and were registered in the ICEBIO database.
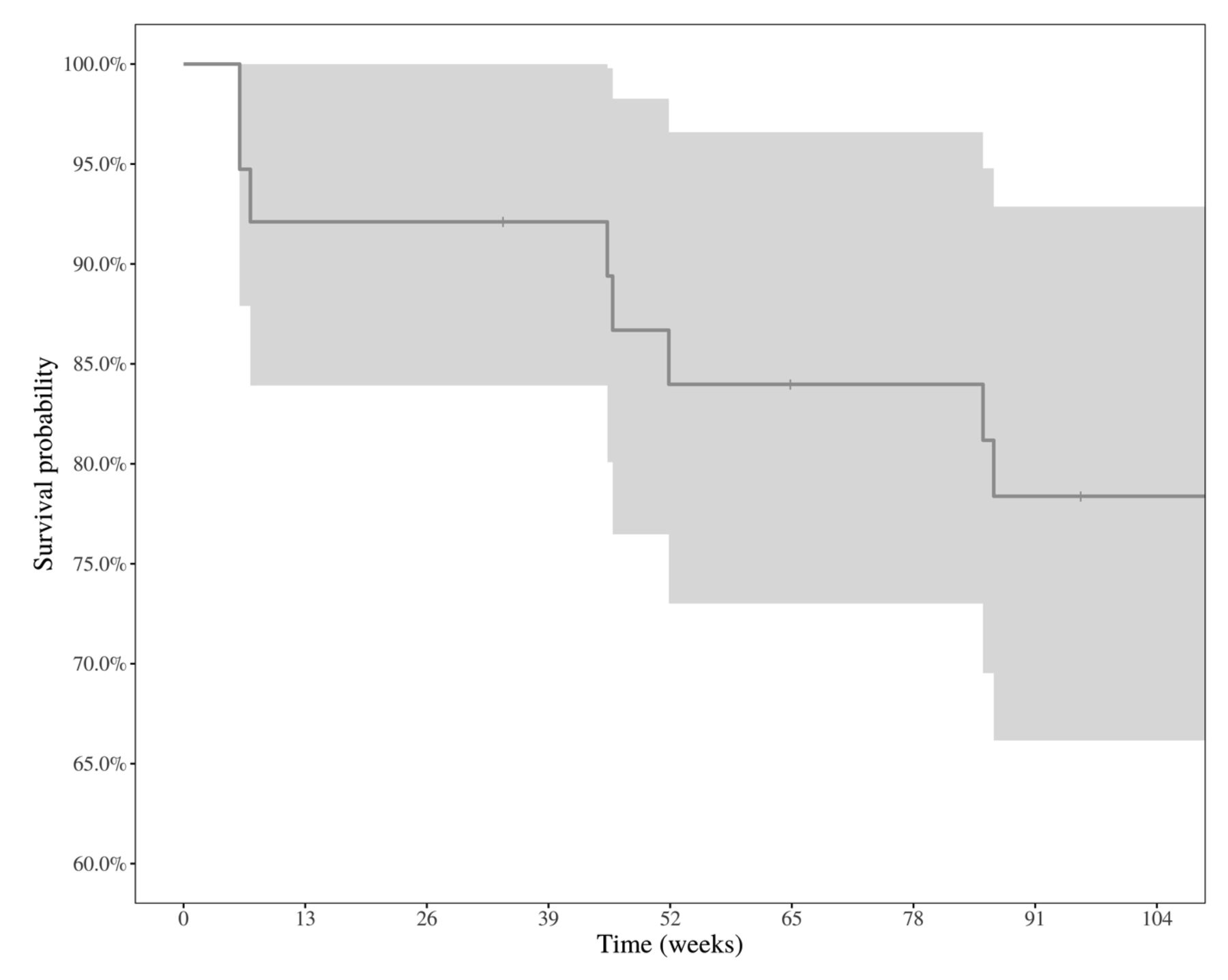
Thirty patients were treated with infliximab (IFX; 79%), 6 with ETN (16%), 1 with adalimumab (ADA), and 1 with golimumab (GOL). The starting dose of IFX was 200 mg in all but 1 instance, where it was 300 mg, followed by infusions on Week 2 and Week 6 and then on 8-week intervals. The starting dose of ETN was 25 mg twice a week in 3 cases, 50 mg once a week in 2 cases, and an unknown dose in 1 case. The ADA dose was 40 mg every other week, and the GOL dose was 50 mg monthly. The mean number of days (25%; 75% quartiles) from the start of biologic therapy to the 6-month visit was 160 days (146; 180) and 441 days (326; 575) to the 18-month visit. Drug survival at 24 months was 78% (Figure 1).

Kaplan–Meier plot for survival of first tumor necrosis factor inhibitor in 38 patients with reactive arthritis.
A triggering organism was found in 45% of patients. Salmonella was the most common bacteria identified (comprising 41% of cases with a known infectious agent). Campylobacter, Chlamydia, and group A Streptococcus were also found (Table 1). Seventy-four percent of patients presented with oligoarthritis and 24% of patients presented with polyarthritis. Enthesitis was present in 26%, and the same percentage of patients had other extraarticular manifestations (Table 2). Of 8 patients tested for HLA-B27 status, 6 were positive.
Clinical features of 38 patients with reactive arthritis who received treatment with TNF inhibitors and were registered in the ICEBIO database.
Ten patients met Braun criteria for ReA and a further 16 were deemed “very likely ReA.” Four patients did not meet these criteria, and data were missing for the remaining 8. However, the patients’ practicing rheumatologists assumed that these patients had ReA.
Functional status markers (CRP level, SJC, TJC, VAS pain, VAS fatigue, DAS28-CRP, CDAI, and HAQ) improved at 6 and 18 months compared to baseline (Table 3). Seventy-one percent of patients (15 of 21 with full data available) were good responders to the treatment; they had a 30% or more reduction of SJC, TJC, and VAS pain, at both 6- and 18-month visits. Joint count information was available for 23 patients at 6 months; 18 had no swollen joints and 15 had no tender joints. Of 22 patients with data available at 18 months, 18 had no swollen joints and 16 had no tender joints. Using the DAS28-CRP scores entered at baseline and at the follow-up visits, 18 (90%) were considered responders at the 6-month visit, and 17 (85%) were considered responders at the 18-month visit (i.e., patients with a decrease by 1 or more disease activity categories of the DAS28-CRP). At 6 and 18 months, 68% and 77% were in DAS28-CRP–defined remission, respectively.
Disease activity of 38 patients with reactive arthritis treated with TNF inhibitors at baseline and the 6-month and 18-month visits, according to data from ICEBIO.
Of the 38 patients who received TNFi, 8 were treated within 1 year of symptom onset and 5 were treated within 6 months. The mean VAS pain score at 18 months for the group of patients treated with TNFi within 6 months of symptom onset was 15, within 1 year was 22, and after 1 year was 23. Responders defined by a 30% reduction in VAS pain, SJC, and TJC at 18 months were 4 out of 4 (with data available) for those who started TNFi within 6 months of symptom onset, 4 out of 5 who started within 1 year, and 11 out of 16 who started after 1 year (Table 4).
Clinical outcomes at the 18-month follow-up visit of 38 patients with reactive arthritis regarding time from symptom onset to the start of TNF inhibitor therapy.
At the time of data acquisition, biologic therapy had lasted on average 8 years (range 1–15). Of the 38 patients, 32 were still receiving biologic therapy. One patient stopped treatment owing to a cancer diagnosis and 1 because of side effects (not requiring hospital admission). Only 2 were able to stop biologic therapy because of remission. They had started treatment with ETN and IFX at 11 and 12 months from symptom onset, respectively, and biologic treatment lasted 1.7 and 12 years, respectively. Data on the current treatment of the remaining 2 patients were missing. Nineteen patients were still receiving the same initial TNFi. Sixteen patients had switched to another biologic medication; 8 because of inefficacy and 4 owing to adverse events. These events were 2 instances of allergic reactions, 1 instance of viral meningitis, and 1 unknown event. These 4 patients had all been treated with IFX.
The 38 patients with ReA received biologics for a total of 303 years. No patient died while receiving biologic therapy. Six patients had infections requiring hospital admission during their TNFi treatment period. Of the 6, there were 3 cases of appendicitis, of which 1 was complicated by appendiceal rupture. The other causes for hospital admission were viral meningitis, human metapneumovirus pneumonia, and pyelonephritis. One patient developed metastatic prostate cancer during biologic therapy, which was subsequently stopped. His ReA was originally triggered soon after surgery for prostate cancer.
DISCUSSION
In this nationwide registry study, we report our experience of outcomes and safety of TNFi in a group of patients with ReA. To our knowledge, this is the largest cohort of ReA patients treated with TNFi, reflecting more than 300 patient-years. The ICEBIO registry has been used in clinical practice in Iceland since 2007. Treating rheumatologists are required to enter disease information into ICEBIO before applying for a bDMARD treatment license and reimbursement by the Icelandic Health Insurance. Standard follow-up data are then registered annually on clinic visits, irrespective of whether the patient is followed up in a hospital outpatient ward or a private rheumatologist’s office21. This gives us a unique opportunity to examine nationwide data on the treatment of various patient groups with different rheumatic conditions.
In our present study, we focus on ReA that has been clinically diagnosed by the treating physician, in most cases an experienced rheumatologist. It is important to note that there is no international consensus on the classification or diagnostic criteria for ReA, or treatment for the disease, as there are for rheumatoid arthritis (RA)22, PsA23, and axSpA24. However, some attempts have been made in this field and studies on ReA have used the Braun criteria19,25. According to these criteria, a diagnosis of ReA is established if both major criteria and 1 minor criterion are met; it is considered a very likely diagnosis if both major criteria or 1 major and 1 minor criterion are met. The major criteria are first, an arthritis typical of ReA and second, preceding enteritis or urethritis. The minor criteria are microbial evidence of Chlamydia in the urogenital tract or positive stool culture for bacteria associated with ReA. Of the 30 patients with data available, only 4 did not meet these criteria. Reflective of the lack of validated criteria, our study focuses on real-world prescribing for a presumed diagnosis of ReA.
Our main finding is that the large majority of patients experienced low disease activity or remission, according to DAS28-CRP, or achieved good response on various patient-reported outcome measures a few months after starting treatment with TNFi. These findings are in accordance with previously discussed studies17,18 that have reported favorable outcomes of TNFi treatment in ReA. Further, safety was acceptable, with 6 hospital admissions due to infections and no deaths during the 303 patient-years of biologic treatment, and no documented reactivation of the triggering infection. Two patients had to switch to another biologic after an allergic reaction. Drug survival was good and similar to drug survival reported in other SpA26.
To our surprise, only 2 patients (5%) were able to stop the TNFi therapy on the basis of remission. This is lower than previous studies have suggested. Meyer, et al17 reported that 3 out of 10 could discontinue TNFi without relapse, and in the Brinster, et al18 study, 5 patients of 15 could stop the medication. It is likely that our cohort had a lower rate of treatment stop owing to remission because it had a larger percentage of chronic ReA patients with a more established SpA (79% treated after 1 year from symptom onset). As a result, there were fewer patients who would have achieved remission irrespective of treatment as a natural course of their disease.
It has been hypothesized that there might be an advantage to giving TNFi within a few months of symptom onset; a “window of opportunity” to avert a chronic course of disease. Although data are limited, the literature does not seem to support this notion. In the Courcoul, et al study, only 1 out of 5 early-treated patients (< 3 mos) was able to stop treatment19. Our study adds 2 cases. Both patients treated within 3 months of symptom onset were unable to discontinue treatment and were still receiving a TNFi at the time of data acquisition, 3.5 and 4.5 years later. Thus, the available data do not support the idea that early treatment of ReA with TNFi halts progression to SpA. Although our sample size is small, our data do seem to suggest that treating soon after symptom onset might result in lower disease activity. Indeed, all 4 patients with available data treated within 6 months were considered treatment responders.
The strength of our present study is first, that it is an unselected population of patients with ReA who were treated with TNFi and the largest to date. Second, it describes treatment efficacy in a group with relatively long symptom duration and established disease. Finally, it reports detailed outcome measures not previously published in ReA. In addition to the common limitations of observational registry studies, such as missing data entries, and retrospective study of medical records, a drawback to this report is that a number of the outcome measures are not validated for use in ReA. Of note, the SJC and TJC in 28 joints are not ideal in ReA because they omit the foot and ankle joints, which are commonly affected in the disease. The 28-joint index was used in this study because it is by far the most used in the ICEBIO database. Thus, the Disease Activity Index for Reactive Arthritis, proposed by Eberl, et al in 200027, could not be used because it relies on the total joint count. The HAQ, CDAI, and DAS28 were developed and validated for RA28 but are commonly used in randomized clinical trials of SpA such as PsA29. It is therefore reasonable to assume that these measures could be reliable in ReA. It should be mentioned that while a significant proportion of the patients had back pain and extraarticular manifestations, there was no way of specifically quantifying their response to treatment other than what surrogate markers, such as VAS pain, could provide.
Three of the included patients in our study were treated with TNFi for post-Streptococcal ReA (PSRA), which is generally regarded as a separate entity from urogenital and enteric ReA30. Indeed, these patients had an upper limb oligoarthritis, an equal upper and lower limb oligoarthritis, and a polyarthritis, respectively. The only extraarticular manifestation noted was erythema nodosum in 1 patient. The patients had all been treated with antibiotics for their pharyngitis. All 3 received IFX, and 2 were treated within 1 year from symptom onset. Only 1 of the 3 patients with PSRA was considered a responder at the 18-month visit. There was no recorded reactivation of Streptococcus or other severe infections during biologic therapy. To our knowledge, these are the first reported cases of PSRA treated with TNFi in the literature.
We have demonstrated in our group of 38 patients with ReA that TNFi are safe and effective. The data also seem to suggest that lower disease activity might be achieved if the active antiinflammatory treatment with TNFi is initiated as soon as traditional treatment options do not result in remission. However, as in other SpA, biologic therapy in ReA tends to be prolonged.
Acknowledgment
The authors thank the patients who recorded their symptoms in ICEBIO and all rheumatologists in Iceland who are part of the ICEBIO group. We also thank Elinborg Stefansdottir, RN, for practical help, and Thorarinn Jonmundsson at the University of Iceland for help with statistical analysis.
- Accepted for publication January 23, 2020.








{kind=link}