

Abstract
Objective. Disease activity in large-vessel vasculitis (LVV) is traditionally assessed by clinical and serological variables rather than vascular imaging. This study determined the effect of treatment on 18F-fluorodeoxyglucose positron emission tomography (FDG-PET) vascular activity in relation to clinical- and serologic-based assessments.
Methods. Patients with giant cell arteritis (GCA) or Takayasu arteritis (TA) were prospectively evaluated at 6-month intervals in an observational cohort. Treatment changes were made at least 3 months before the followup visit and categorized as increased, decreased, or unchanged. Imaging (FDG-PET qualitative analysis), clinical, and serologic (erythrocyte sedimentation rate, C-reactive protein) assessments were determined at each visit and compared over interval visits.
Results. Serial assessments were performed in 52 patients with LVV (GCA = 31; TA = 21) over 156 visits. Increased, decreased, or unchanged therapy was recorded for 36-, 23-, and 32-visit intervals, respectively. When treatment was increased, there was significant reduction in disease activity by imaging, clinical, and inflammatory markers (p ≤ 0.01 for each). When treatment was unchanged, all 3 assessments of disease activity remained similarly unchanged over 6-month intervals. When treatment was reduced, PET activity significantly worsened (p = 0.02) but clinical and serologic activity did not significantly change. Treatment of GCA with tocilizumab and of TA with tumor necrosis factor inhibitors resulted in significant improvement in imaging and clinical assessments of disease activity, but only rarely did the assessments both become normal.
Conclusion. In addition to clinical and serologic assessments, vascular imaging has potential to monitor disease activity in LVV and should be tested as an outcome measure in randomized clinical trials.
- LARGE-VESSEL VASCULITIS
- GIANT CELL ARTERITIS
- FLUORODEOXYGLUCOSE
- TAKAYASU ARTERITIS
- POSITRON EMISSION TOMOGRAPHY
- VASCULITIS
Giant cell arteritis (GCA) and Takayasu arteritis (TA), the 2 major forms of large-vessel vasculitis (LVV), are complex diseases that pose significant management challenges1,2,3,4. Clinical assessment and measurements of acute-phase reactants [erythrocyte sedimentation rate (ESR), C-reactive protein (CRP)] are conventionally used to diagnose and monitor disease activity5; however, accurate determination of disease activity status can be difficult6. Clinical features of disease can be nonspecific (e.g., fatigue, headaches) or potentially related to prior vascular damage rather than active vascular inflammation (e.g., limb claudication, vascular examination abnormalities). Acute-phase reactants are often used to guide treatment decisions, yet these markers are not specific for vasculitis7. Clinically active disease can occur with normal laboratory tests, and persistently abnormal serologic tests without associated clinical symptoms pose clinical conundrums8,9. Accurate assessment of vascular disease activity status is critical because untreated inflammation can result in irreversible damage to the large arteries, and treatments for LVV carry potentially life-threatening risks10.
Vascular imaging, in particular 18F-fluorodeoxyglucose positron emission tomography (FDG-PET), may be useful to detect and monitor vascular inflammation2,11. Multiple studies have demonstrated the utility of FDG-PET in diagnosing LVV2,12,13,14. Recent European League Against Rheumatism recommendations for imaging modalities in LVV include FDG-PET to diagnose LVV15. Few studies have described the role of FDG-PET to monitor vasculitis in established cases of LVV2,11,16,17,18. When patients with LVV undergo a prospective imaging-based assessment, a significant burden of ongoing vascular disease activity has been observed on both magnetic resonance (MR) angiography and FDG-PET during clinical remission, highlighting potential discordance between clinical and imaging assessments at later stages of disease19. Whether serial imaging should guide treatment decisions is debatable20, but patients with LVV can develop new arterial lesions on vascular imaging during periods of apparent clinical remission, and PET activity during remission may predict clinical relapse and angiographic progression of disease2,5,21. There is minimal prospective data about the effects of specific treatment on imaging-based assessment of vascular disease activity in comparison to clinical and serologic assessments. These types of data would provide a more nuanced understanding of drug efficacy in LVV. Glucocorticoids, the mainstay of therapy for patients with LVV, typically improve vascular PET abnormalities18,22, but the effect of specific steroid-sparing therapies on vascular disease activity is unknown.
There are no validated outcome measures of disease activity in LVV, which has hampered the conduct of successful clinical trials in these diseases. Development of a core set of outcome measures that incorporate clinical-, serologic-, and imaging-based assessments of disease activity has been identified as a major unmet need in LVV4. The primary objective of our study was to determine how changes in treatment affect disease activity as measured by FDG-PET in a prospective, observational cohort of patients with GCA and TA seen at scheduled 6-month intervals. The secondary objective was to compare imaging-, clinical-, and serologic-based assessments of disease activity in LVV.
MATERIALS AND METHODS
Study population and clinical assessment
Patients with GCA or TA were recruited from an ongoing prospective, observational cohort at the US National Institutes of Health (NIH). All patients fulfilled the 1990 American College of Rheumatology Classification Criteria for TA or GCA23,24 or modified criteria for GCA25. All patients provided written informed consent (NCT02257866), and the study was approved by ethics and radiation safety committees at the NIH (14-AR-0200).
All patients had at least 2 study visits at scheduled 6-month intervals (minimum of 4 mos and maximum of 12 mos). At each visit, patients underwent a detailed clinical evaluation, imaging assessment, and laboratory investigation. Clinically active disease was defined by the presence of at least 1 clinical symptom directly attributed to ongoing vasculitis by the investigative team. Abnormal acute-phase reactants alone were not considered sufficient evidence of clinical disease activity. Based on clinical assessment, patients were given a physician’s global assessment (PGA) score ranging from 0 to 10, in which a score of 0 indicates clinical remission and increasing scores indicate increased disease activity. PGA was used because there are no clinical disease activity instruments validated for both GCA and TA, and disease activity assessments developed for TA have significant limitations26,27. Clinical assessments were performed blinded to imaging data. A detailed history was obtained at each visit, focused on prior and current therapies taken, including glucocorticoids (GC) and other forms of immunosuppression [both traditional disease-modifying antirheumatic drugs (DMARD) and biologic agents]. All treatment decisions were made by local referring physicians rather than the investigative study team. ESR by Westergren method and CRP were measured at each study visit and considered elevated per institutionally defined laboratory thresholds (ESR > 42 mm/h or CRP ≥ 5 mg/l)28.
Treatment status between visits was categorized as increased, decreased, or unchanged. Treatment change was defined as change in daily prednisone dose by ≥ 5 mg at the time of the followup visit relative to the baseline visit or an addition/50% dose change of a DMARD or biologic therapy at least 3 months prior to the followup visit. Visits were excluded from analysis when there was a simultaneous decrease in GC and an increase in the dose of a DMARD and/or biologic agent between visits. Additionally, response to tocilizumab (TCZ) and tumor necrosis factor inhibitors (TNFi) was specifically studied. For these analyses, interval visits where there was a simultaneous decrease in GC with addition of TCZ or TNFi were included.
Imaging assessment
Patients underwent FDG-PET evaluation at each study visit. Details of the imaging protocol have been previously reported2,19. Briefly, all patients ≥ 18 years of age underwent a whole body FDG-PET/computed tomography (CT) scan, acquired 120 min after administration of 10 mCi FDG, with a Siemens Biograph mCT (Siemens Medical Solutions). To minimize radiation, pediatric subjects underwent whole body FDG-PET/MR imaging with a Siemens Biograph mMR after administration of 0.1 mCi/kg of FDG at 60-min uptake time.
Arterial FDG uptake was measured by qualitative assessment, in accordance with recent recommendations29 and as previously described2. Briefly, degree of arterial FDG uptake was assessed relative to the liver in 9 arterial territories. Each area was scored from 0 to 3 (0 = no FDG uptake; 1 = FDG uptake less than liver; 2 = FDG uptake equal to liver; 3 = FDG uptake more than liver). A global summary score (PET Vascular Activity Score; PETVAS) was calculated by summing the amount of arterial FDG uptake in the 9 territories, with scores ranging from 0 to 272. Changes in PETVAS were assessed over visit intervals. Studies were excluded at the discretion of the readers based on technical quality (e.g., motion artifact or suboptimal image resolution). Because PETVAS is a summary score across multiple vascular territories, a specified PETVAS threshold value was not used to define active vasculitis; scans with focal vasculitis can have low PETVAS and still be considered active2. Instead, PET activity was defined by 2 nuclear medicine physicians who independently evaluated each PET scan study blinded to clinical details and determined by consensus whether the scan was consistent with active vasculitis based upon global assessment of all available images. Excellent interrater reliability (κ = 0.84) has been previously reported by our group using this approach2.
Statistical analysis
All values are given as median and range. P values < 0.05 were considered significant. Wilcoxon signed-rank test was used to compare changes in PETVAS, PGA, ESR, and CRP in association with treatment status and with addition/increase of specific medications. Fisher’s exact test was used to compare the proportion of subjects with clinically active vasculitis and PET activity in association with treatment status.
RESULTS
A total of 52 patients with LVV (GCA = 31; TA = 21) provided data from 156 visits between October 2014 and August 2018. The median interval between visits was 6 months (range 5–12 mos). The median number of visits per patient was 3 (range 2–6). Six PET studies were excluded owing to technical quality issues. Table 1 shows the baseline demographic data of the patients. Median disease duration at the initial visit was shorter in patients with GCA (1.4 yrs) versus TA (4.8 yrs). The median age of the patients with GCA was 72 years [interquartile range (IQR) 62–76 yrs). At the initial visit, 15 patients with GCA (48%) were taking DMARD and/or biologic agents, with 13 of these patients (42%) taking methotrexate (MTX), and 21 patients (68%) were taking GC. The median daily dose of prednisone was 15 mg (range 1–60). In the TA subgroup, the median age was 30 years (IQR 20-37). Five patients < 18 years of age were included in the study. Most patients (n = 17, 81%) were taking a DMARD and/or biologic agent at the initial visit. Five of the patients (25%) were taking combination therapy with conventional DMARD and biologics, and 15 patients (71%) were taking GC treatment. The median daily dose of prednisone was 10 mg (range 2–50).
Study population characteristics at the initial visit.
Interval changes in treatment
There was an increase in treatment preceding 36 study visits in 27 patients. No change in treatment preceded 23 visit intervals in 21 patients. Decreased treatment preceded 32 visit intervals in 24 patients. Nine visit intervals were excluded from the analysis because simultaneous decrease in GC and increase in the dose of a DMARD and/or biologic agent occurred between visits. Interval treatment changes involved GC (n = 46), TCZ (n = 17), TNFi (n = 7), or another DMARD and/or biologic (n = 33).
Increased treatment
In the increased treatment group, simultaneous increase in GC and other immunosuppressive drugs occurred during 14 of 36 (39%) visit intervals. Over 4 visit intervals, there was increase in GC only, whereas over 18 visit intervals, there was increase in dosage/addition of DMARD and/or biologic agent without any significant difference in GC dose. At the baseline visit, the PET scan was interpreted as showing active vasculitis in 30 patients (83%); 25 patients (69%) had clinically active disease and 25 patients (69%) had an elevated CRP or ESR. Median PETVAS significantly improved from baseline to 6-month followup visit (23.5 vs 18; p < 0.01). Concomitantly, significant improvement in median PGA scores (2 vs 0, p < 0.01), CRP (6.2 vs 2.0, p < 0.001), and ESR (24 vs 9, p < 0.0001) was also observed (Figure 1). There was a significant decrease in the number of patients with clinically active vasculitis from baseline to 6-month followup visit [25 patients (69%) vs 14 patients (39%); p = 0.02]. However, many patients continued to have vascular FDG-PET uptake that, while improved from the baseline visit, was still interpreted as active vasculitis at the followup visit [30 patients (83%) vs 24 patients (67%); p = 0.17; Figure 2].
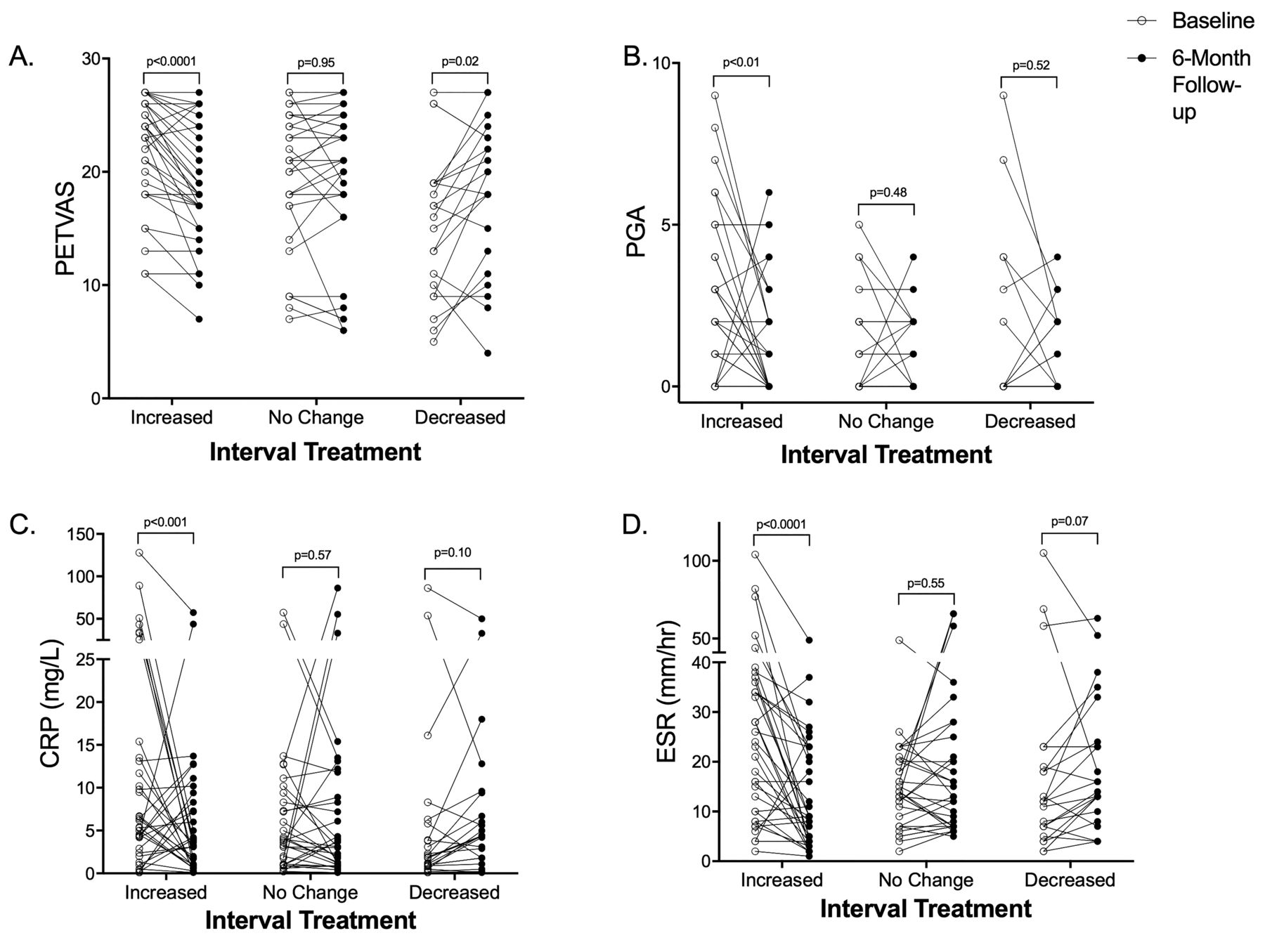
Changes in imaging, clinical, and serologic measurements of disease activity following treatment among patients with large-vessel vasculitis (giant cell arteritis or Takayasu arteritis). A. PET scan activity as measured by the PETVAS significantly improved over 6-month intervals following increased treatment, remained unchanged when there was no change in treatment, and significantly worsened following decreased treatment. B–D. Clinical disease activity, as measured by the PGA, and serologic activity, as measured by CRP and ESR, significantly improved in response to increased treatment but did not significantly change over 6-month intervals when treatment was not changed or was decreased. Note: overlapping data points from different patients may occur in this figure. PET: positron emission tomography; PETVAS: PET Vascular Activity Score; PGA: physician’s global assessment; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate.

Change in FDG-PET scan activity and clinical activity following increased treatment in large-vessel vasculitis. Of 36 instances where treatment was increased in the interval between study visits, PET activity was observed in 30 (80%) baseline assessments and clinical activity in 25 (69%) baseline assessments. Following an increase in treatment, PET activity remained present in 24 (67%) of the 6-month followup assessments and clinical activity persisted in 14 (39%) of the 6-month followup assessments. FDG-PET: 18F-fluorodeoxyglucose positron emission tomography; 6M: 6-month followup.
Unchanged treatment
Treatment status was unchanged over 32 visit intervals. FDG-PET data, available following 30 of these 32 visit intervals, did not show any change in the PETVAS score (21 vs 21, p = 0.95). Similarly, PGA (0 vs 0, p = 0.48), CRP (3.9 vs 3.4, p = 0.57), and ESR (13.5 vs 13, p = 0.55) remained stable over followup (Figure 1).
Decreased treatment
Decreased treatment was noted over 23 visit intervals. Simultaneous reduction in GC plus other immunosuppressive drugs occurred during 3 visit intervals. Decrease in daily GC dose without any change in other immunosuppressive drugs occurred during 16 visit intervals. Decrease in DMARD/biologic with no change in GC dose occurred during 4 visit intervals. PETVAS score was available following 21 visit intervals. Compared to the baseline visit, there was significant increase of PETVAS at the 6-month followup (16 vs 20, p = 0.02). In contrast to imaging assessment, there were no significant differences in PGA (0 vs 0, p = 0.52), CRP (1.9 vs 4.4, p = 0.10), or ESR (12 vs 16, p = 0.07; Figure 1).
Response to TCZ
TCZ was initiated after the initial visit in 17 patients with GCA. Most of these patients were taking prednisone (76%) and MTX (59%) at the initial visit. Every patient had active vasculitis by PET at the initial visit. PETVAS significantly improved after treatment with TCZ (25 vs 21.5; p < 0.01). There was also significant improvement in PGA (2 vs 0; p < 0.01), CRP (6.7 vs 0.3; p < 0.01), and ESR (22 vs 3, p < 0.01; Figure 3A). There was a significant decrease in the median daily dose of prednisone (7 mg to 3 mg; p < 0.01) and weekly dose of MTX (20 mg to 0 mg; p = 0.03) with addition of TCZ. PET scan activity improved in 8 out of 9 patients with GCA who started TCZ later into the disease process without a change in GC dosing between interval assessments (PETVAS 24 vs 20; p = 0.01), including 5 patients who were treated for persistent mild clinical disease activity with TCZ alone without addition of any GC therapy (PETVAS 24 vs 19.5; p = 0.03). Despite significant improvement in PETVAS, only 3 patients (18%) had normalization of PET activity after treatment with TCZ. In contrast, clinical remission after TCZ occurred in 14 of these patients (82%). Representative images of FDG-PET response to TCZ are shown in Figure 4.
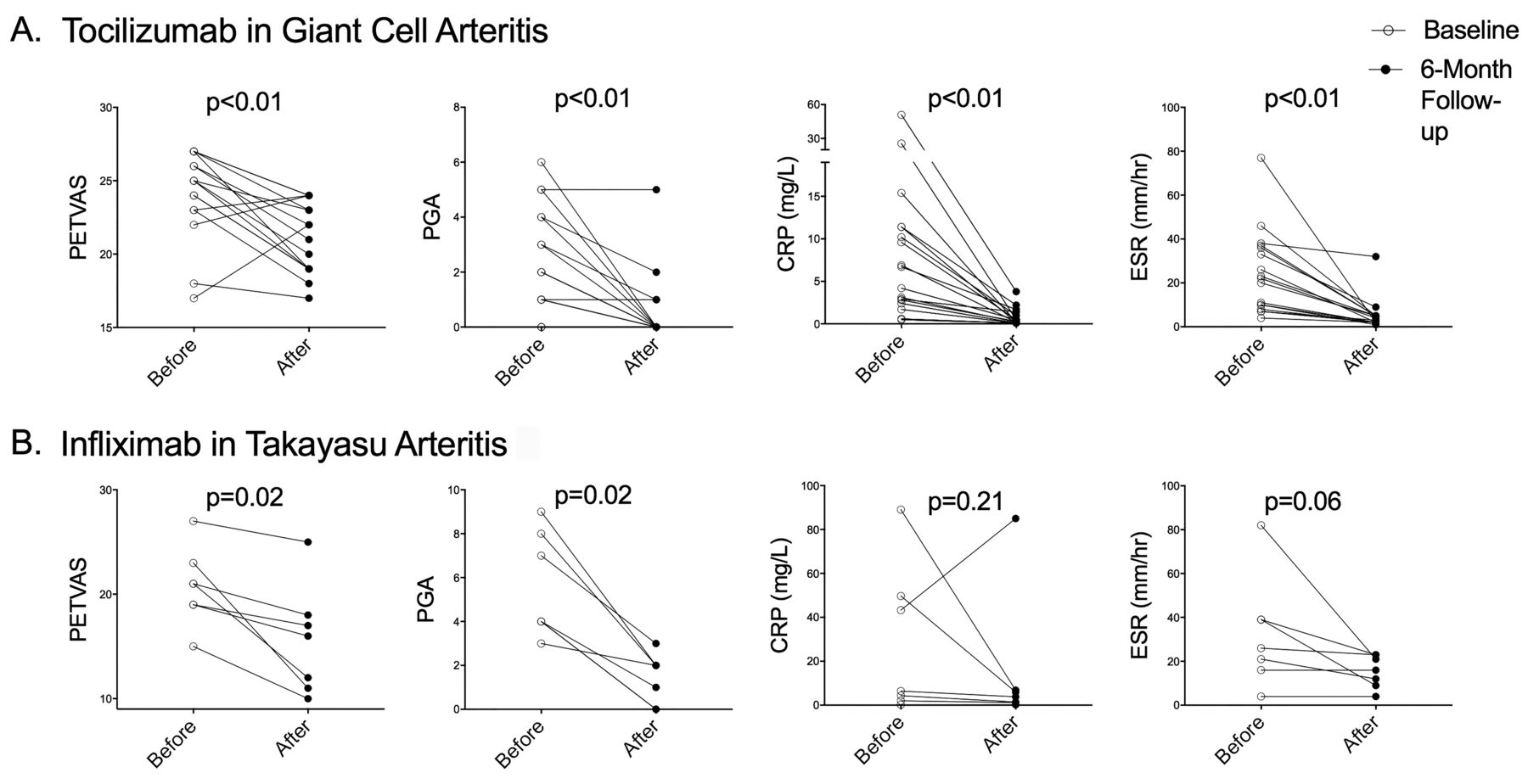
Changes in measures of disease activity in large-vessel vasculitis in response to specific treatments. A. PET activity (PETVAS), clinical activity (PGA), and serologic activity (CRP, ESR) all significantly improved in 17 patients with giant cell arteritis who were treated with tocilizumab over a 6-month interval. B. PET activity and clinical activity, but not serologic activity, significantly improved in 7 patients with Takayasu arteritis treated with infliximab. Note: overlapping data points from different patients may occur in this figure. PETVAS: PET Vascular Activity Score; PGA: physician’s global assessment; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate.
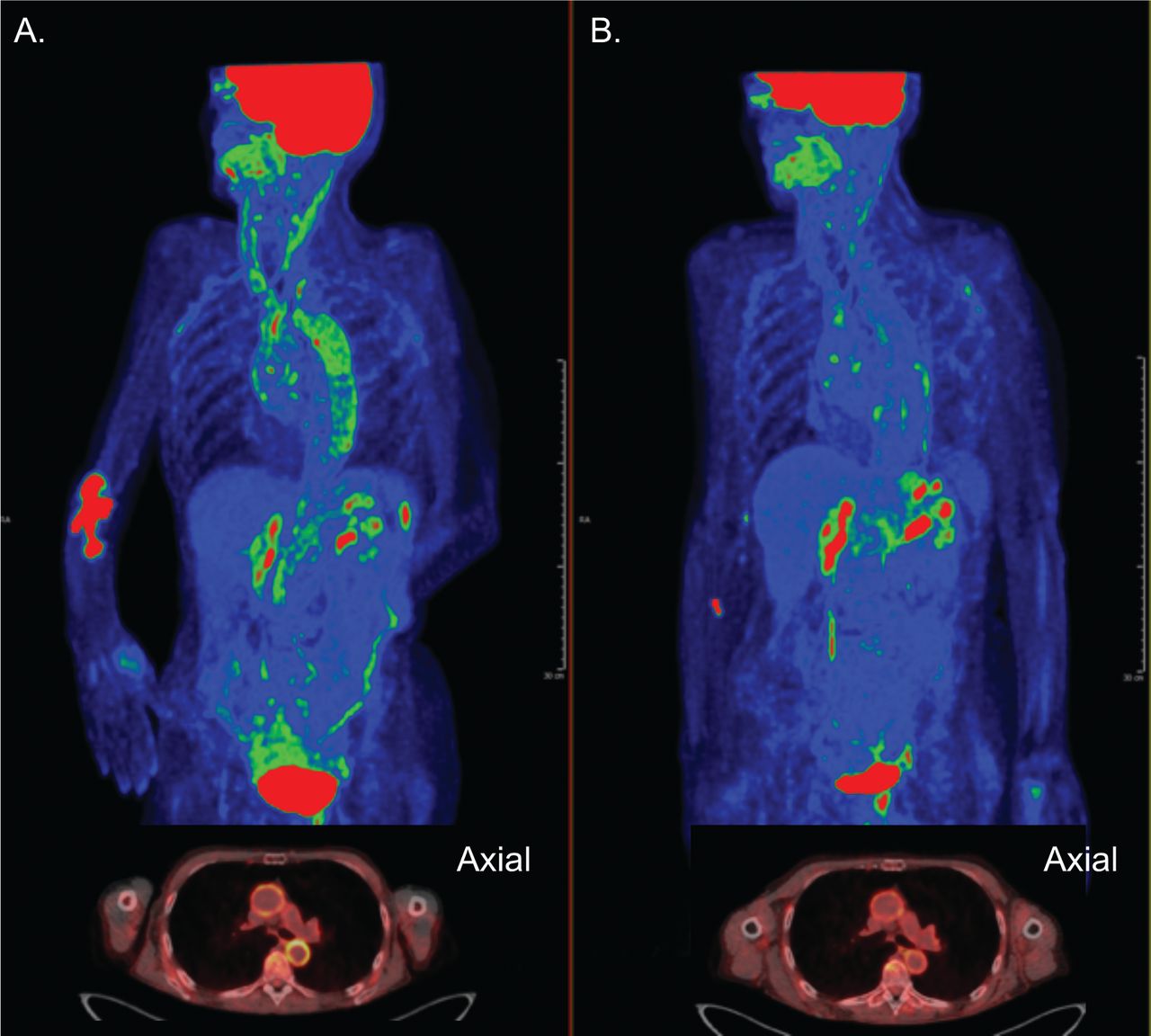
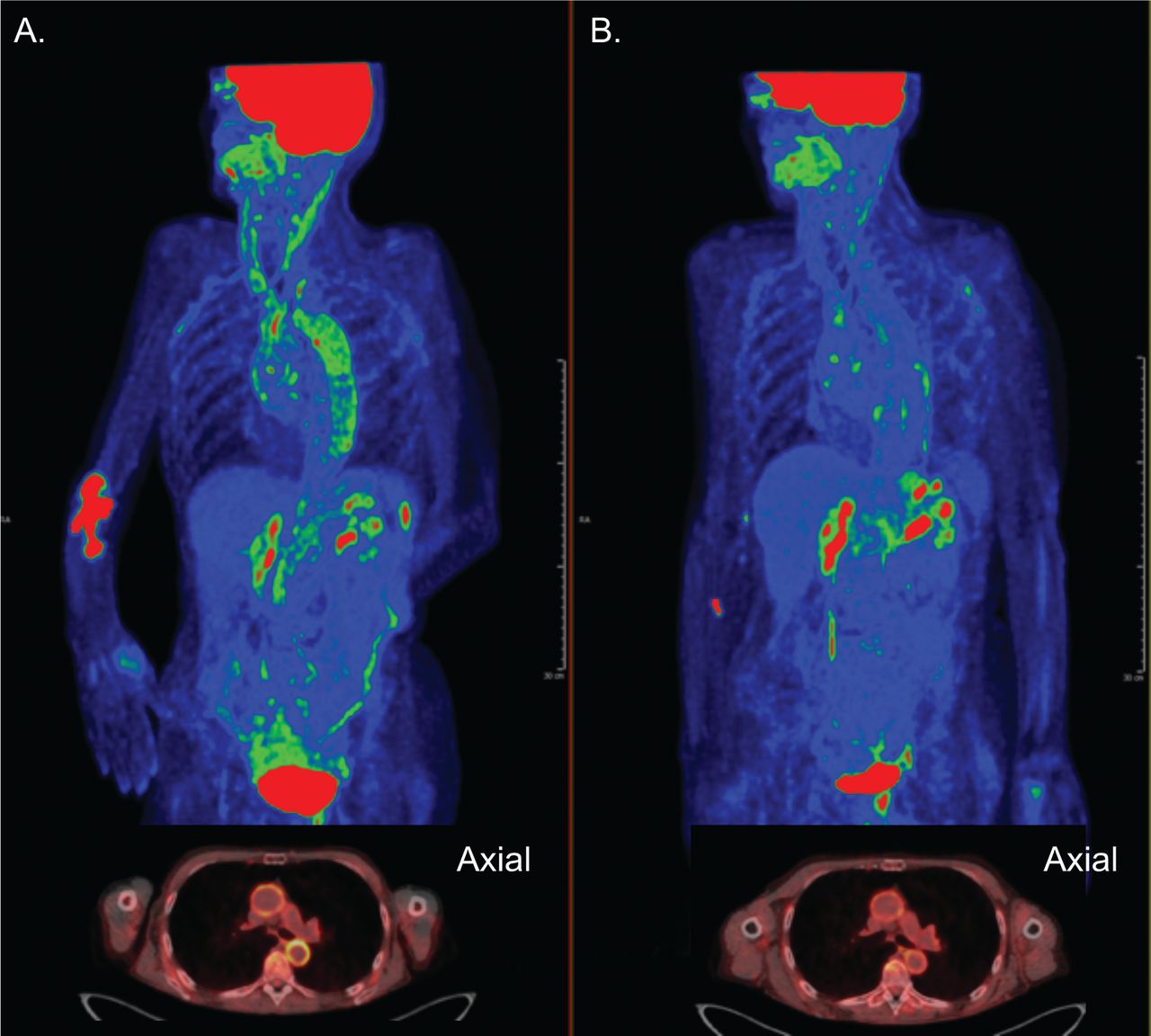
An example of a patient with giant cell arteritis with improvement in vascular inflammation as measured by FDG-PET following initiation of treatment with tocilizumab (TCZ). A 72-year-old woman with large-vessel giant cell arteritis presented for initial evaluation 2 years into disease course while taking prednisone 5 mg/day. She reported fatigue, malaise, and chronic limb claudication (PGA = 2). Levels of acute-phase reactants were normal (ESR = 8 mm/h, CRP = 0.5 mg/l). FDG-PET showed moderate/severe FDG uptake (green/red) throughout the aorta and arch vessels (PETVAS = 27). Baseline visit shows whole-body imaging with axial view inset demonstrating PET activity in the ascending and descending aorta (A). The patient was treated with TCZ 162 mg every other week and prednisone 5 mg/day was continued without a change in dose. At the followup visit 6 months later, there was substantial improvement, but not complete normalization, of arterial FDG uptake (PETVAS = 24). Followup visit shows whole-body imaging with axial view inset showing improved but persistent PET activity in the ascending and descending aorta (B). FDG-PET: 18F-fluorodeoxyglucose positron emission tomography; PETVAS: PET Vascular Activity Score; PGA: physician’s global assessment; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate.
TCZ was initiated after the baseline visit in 3 patients with TA. All patients had improvement in PETVAS and acute-phase reactants, but only 1 patient achieved clinical remission. One patient with TA taking TCZ at the baseline visit had active vasculitis by clinical and imaging assessment despite normalization of acute-phase reactants, prompting discontinuation of TCZ.
TNFi
Infliximab (IFX) was initiated after the initial visit in 7 patients with TA. All 7 patients had an improvement in PETVAS following initiation of IFX (21 vs 16; p = 0.02; Figure 3B). All patients had active vasculitis at baseline by PET, and 5 patients continued to have active vasculitis by PET at the followup visit despite treatment. Representative images are shown in Figure 5. There was significant improvement in clinical assessment of disease activity in these patients (4 vs 2; p = 0.02); however, 5 out of 7 patients (71%) continued to have clinically active disease at followup. There was no significant change in CRP (6.4 vs 3.8; p = 0.21) or ESR (26 vs 16; p = 0.06) in these patients. All patients treated with IFX were also treated with MTX, but the weekly dose of MTX was not statistically different before and after initiation of IFX. There were no significant differences in daily prednisone dose before and after IFX treatment (10 vs 12.5 mg; p = 0.78).

Example of a patient with Takayasu arteritis (TA) with improvement in vascular inflammation as measured by FDG-PET following initiation of treatment with tumor necrosis factor inhibitor and MTX. A 15-year-old girl with TA presented for initial evaluation 1 year into disease course on TCZ 162 mg every other week and prednisone 10 mg/day. She reported ongoing headaches, visual disturbance, postural lightheadedness, fatigue, malaise, and abdominal pain. The PGA = 8 and the levels of acute-phase reactants were normal (ESR = 4 mm/h, CRP = 0.2 mg/l). FDG-PET MRI showed moderate (green) to severe (red) FDG uptake with associated increased wall thickness in the abdominal aorta (A, white arrow) and carotid arteries (B, white arrows) with PETVAS score of 15. TCZ was discontinued and she was treated with IFX, MTX, and increasing doses of glucocorticoids. At the followup visit 6 months later, IFX 7.5 mg/kg every 4 weeks, MTX 20 mg weekly, and prednisone 20 mg daily, there was substantial reduction in vascular wall thickness on angiography and normalization of FDG-PET activity (PETVAS = 10) in the abdominal aorta (C, white arrows) and carotid arteries (D, white arrows). FDG-PET: 18F-fluorodeoxyglucose positron emission tomography; PETVAS: PET Vascular Activity Score; MRI: magnetic resonance imaging; PGA: physician’s global assessment; CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; MTX: methotrexate; IFX: infliximab; TCZ: tocilizumab.
TNFi were initiated after the baseline visit in 3 patients with treatment-refractory GCA (IFX = 2; adalimumab = 1). All 3 patients had evidence of large-vessel involvement, with PET activity at the baseline visit. Improvement in PET activity and clinical assessment was observed in only 1 of these patients at the 6-month followup visit.
DISCUSSION
This study details changes in disease activity, as measured by vascular FDG-PET uptake, in relation to changes in treatment over 6-month intervals in patients with LVV. The findings represent an important step to demonstrate that FDG-PET has the necessary performance characteristics of a potential treatment response biomarker in LVV. In association with increases in treatment, there were significant improvements in clinical-, serologic-, and imaging-based measures of disease activity. When there was no significant interval change in treatment status, disease activity as measured by clinical-, serologic-, and imaging-based markers remained similarly unchanged. Intriguingly, when treatment was reduced, vascular activity by FDG-PET significantly worsened while clinical and serologic markers of activity did not significantly change, suggesting FDG-PET may be more sensitive in detecting early-stage worsening of disease activity. Subgroup analysis in GCA and TA also showed similar changes in PETVAS (data not shown).
While vascular activity by FDG-PET consistently improved in response to increases in therapy, vascular PET abnormalities rarely normalized. Many studies have reported a decrease in arterial FDG uptake with corresponding improvement in clinical and serological variables with addition of treatment (Supplementary Table 1, available with the online version of this article)11,16,17,18,30–37. However, most of these studies were case reports with retrospective study designs, relatively short followup intervals between imaging assessments, and exclusive focus on the effect of GC monotherapy. Using a prospective study design and a novel metric of global vascular disease activity (PETVAS), significant reduction of PET activity in the aorta and primary branches was demonstrated in response to different treatments in GCA and TA. On average, PETVAS decreased by 5.5 in response to increased treatment. A recent study demonstrated that a decrease in PETVAS by 1 point on average corresponded with significant clinical improvement in response to treatment with an IFX biosimilar therapy38. While PET scan findings improved in most patients who had clinical responses to increased treatment, the followup PET scan normalized in response to treatment in the minority of patients. Longer duration of followup with repeat imaging may be useful to see whether the FDG-PET uptake continues to improve with treatment; however, histology and autopsy data also demonstrate persistent vascular disease activity in LVV during established clinical remission2,39,40,41.
This study offers an opportunity to assess prospectively the effect of specific medications on imaging-based assessment of disease activity. More recently, 2 randomized clinical trials demonstrated efficacy of TCZ in GCA in relation to clinical and serologic outcome measures42,43. Because imaging data were not systematically studied as outcome measures in either trial, the effect of TCZ on vascular disease activity is currently unknown. In our current study, there was significant improvement in clinical, serologic, and imaging assessments over a 6-month interval in 17 patients with GCA treated with TCZ. Although 14 out of 17 patients achieved clinical remission on TCZ, PET scan findings normalized in only 3 of these patients. These results are consistent with a small study of 9 patients with GCA treated with TCZ that showed persistent vessel wall enhancement in 33% of patients on MR angiography up to 1 year after initiation of treatment44. Our current study also demonstrates a beneficial effect of TCZ on PET activity that is independent of potential concomitant GC use, because PET activity significantly improved in a subset of patients with GCA who were treated for mild active disease with TCZ alone without any GC. Among the few patients with TA treated with TCZ, subsequent change in PET activity was variable. Results from a recent randomized trial of TCZ in TA have not demonstrated convincing efficacy45.
Observational cohort data suggest that TNFi are effective at improving clinical disease activity and reducing angiographic progression of disease in TA, but sustained remission is rare and accrual of vascular damage is still common46,47. All 7 patients with TA in our study treated with TNFi experienced significant improvement in clinical and vascular disease activity; however, acute-phase reactants did not significantly improve, only 2 patients achieved clinical remission, and PET normalized in only 2 patients. Clinical trial data have demonstrated that TNFi are not effective to treat GCA48. In our current study, 3 patients with treatment-refractory GCA were treated with TNFi, with clinical and imaging improvement seen in only 1 patient.
Vascular PET activity significantly increased in association with reduction in immunosuppressive treatment for LVV, without corresponding significant worsening in clinical or serologic disease activity. There are several potential explanations for this observation. FDG-PET may be especially sensitive to detect subclinical recurrence of vascular inflammation. Alternatively, increase in PET activity with reduction in treatment could be related to increased metabolic activity from vascular repair or a secondary cause such as worsening atherosclerosis49. Novel PET ligands that target specific immune cell populations may improve accuracy to detect vascular inflammation; however, FDG is rapidly cleared from the blood pool and distributed into the arterial wall, making it the best radiotracer currently available to study metabolic activity in the large arteries. Previous work has demonstrated the amount of vascular PET activity during clinical remission predicts clinical relapse2. One limitation of the current study is the lack of longitudinal followup data to determine whether change in PET activity over time in relationship to treatment status predicts clinical relapse or angiographic progression of disease.
There are several other study limitations to consider. This study was not an inception cohort, and most of the patients had established disease and were taking treatment at the baseline visit. A recent study demonstrated rapid reduction in vascular PET uptake after initiation of high doses of prednisone in patients with newly diagnosed GCA22. By including many patients at later stages of disease, the average prednisone dose at the baseline visit in this study was modest and unlikely to have affected serial measurements. Given the observational study design, selection bias could influence patient recruitment and treatment decisions. However, all treatment decisions for patients in our study were made by local, referring physicians rather than the study investigators. The referring physicians had access to all test results including the FDG-PET scans, which could have influenced treatment decisions; however, treatment based on PET findings alone in absence of corresponding clinical symptoms or angiographic progression of disease is not considered standard of care. Qualitative rather than semiquantitative metrics were used to monitor PET activity because semiquantitative assessment of FDG-PET has not been standardized in LVV.
This study identified, in relationship to changes in treatment, concordant and discordant changes in disease activity measured by FDG-PET compared to conventional approaches (clinical and serological assessments). These findings support a need to study FDG-PET as a potential outcome measure of vascular activity in clinical trials in LVV and to evaluate imaging findings in relation to longterm clinical outcomes in observational cohorts of patients with LVV.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
KAQ received funding from a Vasculitis Clinical Research Consortium (VCRC)/Vasculitis Foundation Fellowship. The VCRC is part of the Rare Diseases Clinical Research Network, an initiative of the Office of Rare Diseases Research, National Center for Advancing Translational Science (NCATS). The VCRC is funded through collaboration between NCATS and NIAMS (U54 AR057319).
This work was supported by the Intramural Research Program at NIAMS.
- Accepted for publication February 15, 2019.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}