

Abstract
Objective. Biologic agents with different mechanisms of action [inhibitors of tumor necrosis factor-α (TNF-α), interleukin (IL)-12/23, and IL-17] showed efficacy in randomized controlled trials (RCT) in the treatment of psoriatic arthritis. We conducted a pooled metaanalysis of these agents for treatment of dactylitis and enthesitis and compared results with the American College of Rheumatology 20 (ACR20) response and Health Assessment Questionnaire–Disability Index (HAQ-DI) scores.
Methods. A systematic literature search was performed and a pooled metaanalysis of RCT with anti-TNF-α (infliximab, golimumab, adalimumab), anti–IL-12/23 (ustekinumab), and anti–IL-17 (secu kinumab, ixekizumab) was conducted using the random-effects model. Bias was assessed using the Cochrane risk-of-bias tool.
Results. Eighteen RCT were included in the pooled analysis (n = 6981). Both TNF-α inhibitors and novel biologics (ustekinumab, secukinumab, ixekizumab) demonstrated significant resolution of dactylitis at Week 24 with pooled risk ratios (RR) versus placebo of 2.57 (95% CI 1.36–4.84) and 1.88 (95% CI 1.33–2.65), respectively. For resolution of enthesitis at Week 24, RR for TNF-α inhibitors was 1.93 (95% CI 1.33–2.79) versus 1.95 (95% CI 1.60–2.38) for novel biologics. Both biologic categories showed overlapping ranges of ACR20 responses (TNF-α inhibitors: RR = 2.23, 95% CI 1.60–3.11; pooled IL-12/23 and −17: RR = 2.30, 95% CI 1.94–2.72) and similar quality of life improvement scores with mean HAQ-DI score changes of −0.29 (95% CI −0.39 to −0.19) and −0.26 (95% CI −0.31 to −0.22), respectively.
Conclusion. The pooled analysis demonstrated that anti–TNF-α agents have the same efficacy as novel agents (ustekinumab, secukinumab, and ixekizumab) in dactylitis and enthesitis.
Psoriatic arthritis (PsA) is a chronic condition comprising inflammation within the joint (synovitis) and in the periarticular soft tissue (dactylitis and enthesitis)1,2,3,4,5. Both dactylitis and enthesitis impair joint function and reduce the patient’s quality of life. Dactylitis (“sausage digit”) is thought to result from flexor tenosynovitis, whereas enthesitis is defined by inflammation of the attachment site of tendons, ligaments, or joint capsules to bone6,7,8. The presence of dactylitis correlates with PsA severity and increases the risk of erosive damage of the joints1,9.
Both anti-tumor necrosis factor (TNF)-α and the cytokines of the TH17 pathway [interleukin 23 (IL-23), IL-17A, and IL-17F] have been identified as important elements in the pathogenesis of PsA, including dactylitis and enthesitis10,11,12,13. However, the primary endpoint in randomized controlled trials (RCT) in PsA was the American College of Rheumatology 20% (ACR20) response, which identifies mainly intraarticular joint manifestations. Extraarticular manifestations were included only as secondary endpoints and partially identified by various outcome measures and by Health Assessment Questionnaire–Disability Index (HAQ-DI) scores14. Thus, despite the widespread use of biologics to treat extraarticular manifestations of PsA, supportive evidence is inferior to that for psoriatic synovitis10,12,13,15.
We conducted a systematic literature review and metaanalysis on the evidence available on dactylitis and enthesitis using clinical disease resolution as an endpoint. Moreover, we created a pooled analysis for ACR20 and HAQ-DI to contextualize improvement in dactylitis and enthesitis in PsA and PsA-related disability.
MATERIALS AND METHODS
Study eligibility
This study included RCT investigating the biologic treatment outcomes of dactylitis resolution, enthesitis resolution, efficacy, and health-related quality of life. The primary outcome of interest was resolution of dactylitis and enthesitis, and secondary outcomes were ACR20 response rates and change in Health Assessment Questionnaire (HAQ) score from baseline at Weeks 12–16 and Week 24. Studies were excluded for the following reasons: unclear reporting of data, lack of randomization or control group, patient age < 18 years, or if they were abstracts, conference proceedings, letters to the editor, review papers or case reports. All studies were published in English.
Search strategy
A literature search was conducted (by author A. Mourad) using Medline (PubMed), the Cochrane Library, EMBASE (Ovid), Scopus, and Web of Science. The search string used in this systematic review (using MeSH terminology) was “psori* AND biologic AND arth* AND dactylitis AND enthesitis AND HAQ AND ACR.” The date of the last search was February 12, 2018. Additional studies were searched manually and identified from the reference lists of the included studies.
Study screening
Both authors screened titles and abstracts of the articles for inclusion using the inclusion criteria. Both authors reviewed full texts independently and in an unblinded fashion.
Data extraction
Data were extracted from papers and presented in tables, which were triple-checked for accuracy. The study characteristics extracted were the study title (author and year), treatment versus control, patient number (treatment), patient number (control), study duration (weeks), study week (week), age (yrs), dactylitis (n), enthesitis (n), ACR20 response, and HAQ score change from baseline and Week 24 of treatment, and where available, for weeks 12–16. Bias was assessed using the Cochrane risk-of-bias assessment tool. We recorded the assessment for selection bias, detection bias, attrition bias, reporting bias, and other bias.
Statistical analysis
Numbers of patients with resolution of dactylitis and enthesitis were calculated from data reported on the numbers of patients with dactylitis and enthesitis at baseline and at weeks 12–16 and Week 24 followup. A metaanalysis of the included studies was performed for resolution of dactylitis and enthesitis, ACR20 response, and change of HAQ score from baseline for biologics versus placebo. Supplementary metaanalyses were also generated for the biologics that performed “best-in-class” and were directly compared. A random-effects model was used to generate forest plots. Statistical analysis was completed using Review Manager version 5.3 (RevMan; computer program. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
The study was conducted in accord with the Preferred Items for the Reporting of Systematic reviews and Meta-analysis (PRISMA) guidelines16.
RESULTS
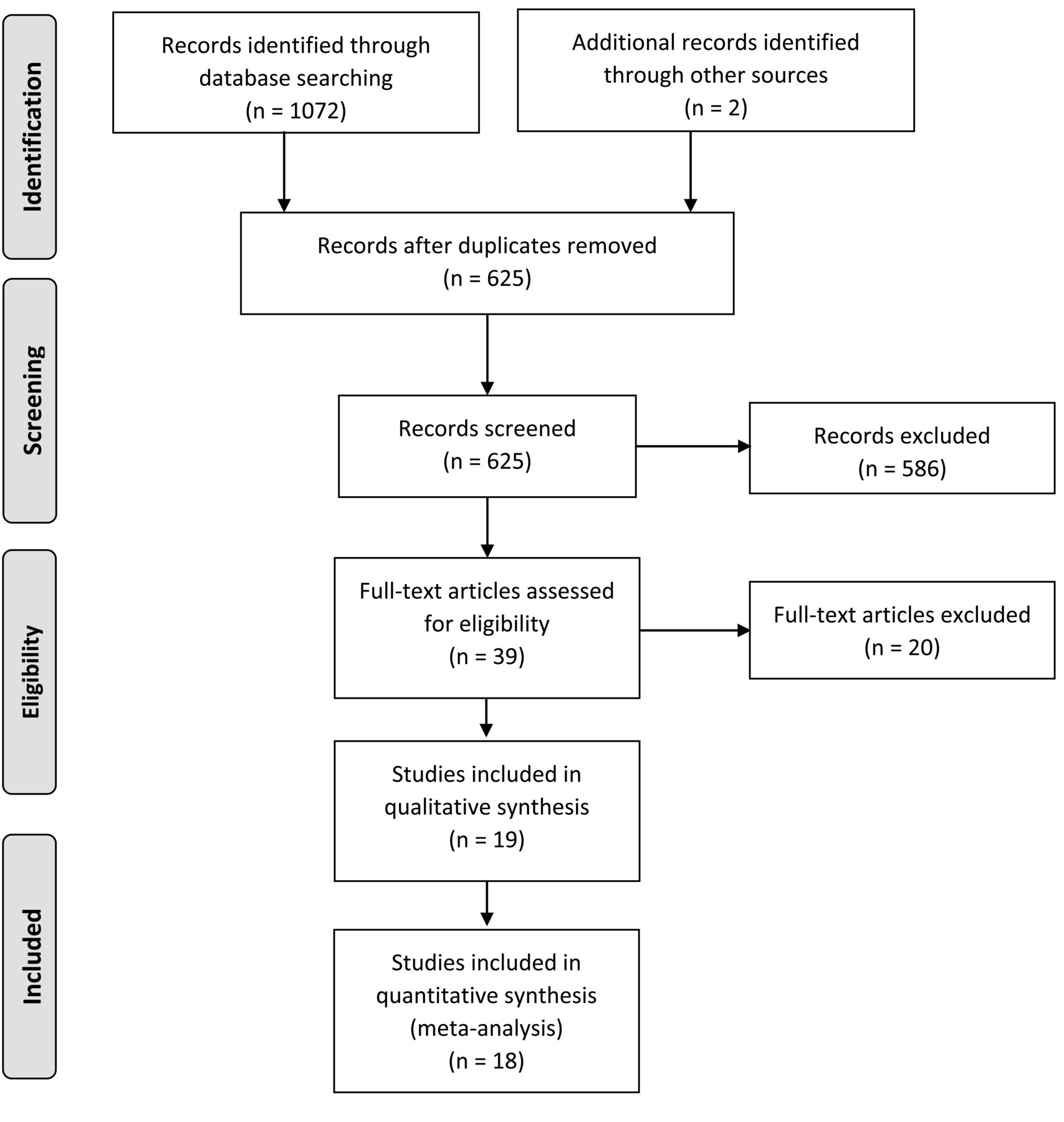
The included studies were RCT investigating the biologic treatment resolution of dactylitis and enthesitis, ACR20 response, and quality of life measured with the HAQ. After removal of duplicates, the systematic search identified 625 studies. Thirty-nine were considered potentially relevant and were read as full texts. After this step we finally included 19 articles comprising 7254 patients (Figure 1). All studies contained at least 24-week efficacy data for at least 1 efficacy endpoint: 8 studies for dactylitis resolution (treatment n = 546, placebo n = 138)17,18,19,20,21,22,23,24, 7 studies for enthesitis resolution (treatment n = 516, placebo n = 123)18,19,20,21,22,24,25, 10 studies for ACR20 response (treatment n = 1402, placebo n = 440)17,18,19,21,22,24,25,26,27,28, and 9 studies for HAQ-DI response (treatment n = 1826, placebo n = 1388)18,19,20,21,22,24,25,27,29 (Supplementary Table 1, available with the online version of this article).

Study selection process in accord with PRISMA guidelines (Preferred Items for the Reporting of Systematic reviews and Meta-analysis).
To increase the power of the analysis we stratified the treatment groups into the TNF-α inhibitor group (adalimumab, etanercept, infliximab, certolizumab, and golimumab) and the novel biologic group (ustekinumab, secukinumab, brodalumab, and ixekizumab), which all target cytokines from the TH17 pathway (IL-23, IL-17A, IL-17F, and IL-17 receptor).
Risk of bias
The Cochrane risk-of-bias assessment was conducted and revealed a low overall risk of bias for selection bias, detection bias, attrition bias, reporting bias and other bias for the studies included (Supplementary Figure 1, available with the online version of this article).
Dactylitis resolution
At weeks 12–14 the dactylitis resolution pooled risk ratio (RR) for TNF-α inhibitors was 1.53 (95% CI 1.01–2.31), and the pooled RR for novel biologics was 1.39 (95% CI 1.06–1.81). This corresponded to pooled RR for all biologics combined of 1.42 (95% CI 1.13–1.80; Supplementary Figure 2, available with the online version of this article). At Week 24, the pooled RR for all biologics combined was 2.07 (95% CI 1.54–2.80; Figure 2). Pooled RR for TNF-α inhibitors and novel biologics were 2.57 (95% CI 1.36–4.84) and 1.88 (95% CI 1.33–2.65, respectively; Figure 2).

Forest plot of dactylitis resolution for TNF-α inhibitors and novel biologics at Week 24. The square sizes represent the statistical weight for each study. Black horizontal bars represent 95% CI. Diamond values indicate pooled effect estimates. TNF-α: tumor necrosis factor-α; M-H: Mantel-Haenszel test.
Enthesitis resolution
At weeks 12–14 the enthesitis resolution pooled RR for TNF-α inhibitors was 1.75 (95% CI 0.96–3.21), and the pooled RR for novel biologics was 1.87 (95% CI 0.77–4.54). This corresponded to pooled RR for all biologics combined of 1.72 (95% CI 1.14–2.59; Supplementary Figure 3, available with the online version of this article). Pooled RR for enthesitis resolution for biologics combined was 1.95 (95% CI 1.63–2.32). Enthesitis resolution yielded RR of 1.93 (95% CI 1.33–2.79) and 1.95 (95% CI 1.60–2.38) for TNF-α inhibitors and novel biologics, respectively (Figure 3).

Forest plot of enthesitis resolution for TNF-α inhibitors and novel biologics at Week 24. The square sizes represent the statistical weight for each study. Black horizontal bars represent 95% CI. Diamond values indicate pooled effect estimates. TNF-α: tumor necrosis factor-α; M-H: Mantel-Haenszel test.
ACR20 response and change in HAQ-DI scores from baseline
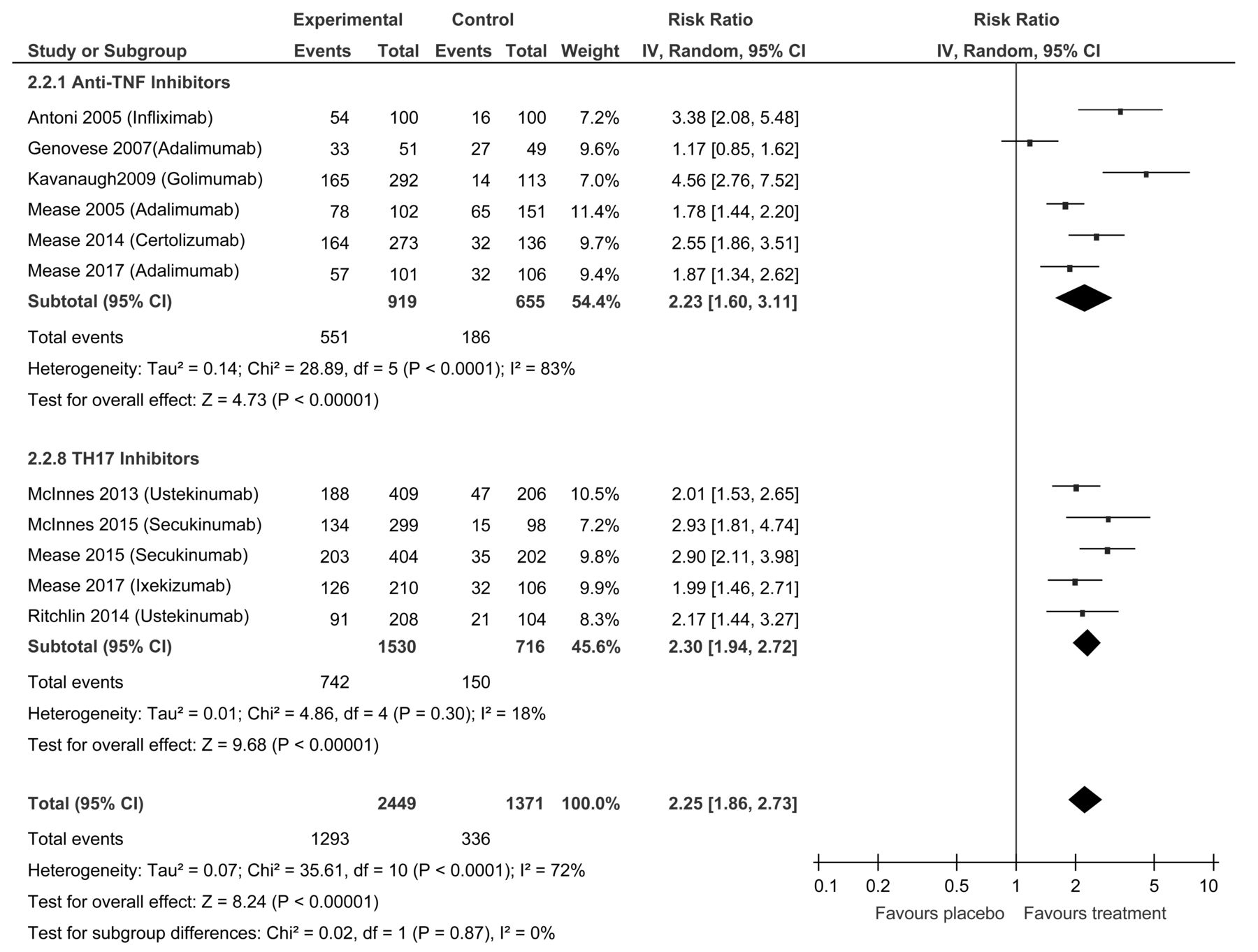
At weeks 12–16 the ACR20 response pooled RR for TNF-α inhibitors was 3.47 (95% CI 2.45–4.92), and the pooled RR for novel biologics was 2.04 (95% CI 1.79–2.33). This corresponded to pooled RR for all biologics combined of 2.62 (95% CI 2.17–3.18; Supplementary Figure 4, available with the online version of this article). The pooled RR for ACR20 response for all biologics at 24 weeks was 2.25 (95% CI 1.86–2.73). TNF-α inhibitors and novel biologics showed pooled RR of 2.23 (95% CI 1.60–3.11) and 2.30 (95% CI 1.94–2.72), respectively (Figure 4). The pooled mean change in HAQ scores at weeks 12–14 was −0.24 (95% CI −0.28 to −0.20) for TNF-α inhibitors and −0.34 (95% CI −0.35 to −0.33) for novel biologics, corresponding to a pooled mean change for all biologics of −0.27 (95% CI −0.35 to −0.20; Supplementary Figure 5). At Week 24, the mean change in HAQ scores from baseline gave a pooled value of −0.27 (95% CI −0.31 to −0.23) for all biologics, −0.29 (95% CI −0.39 to −0.19) for TNF-α inhibitors, and −0.26 (95% CI −0.31 to −0.22) for novel biologics (Figure 5).

Forest plot of ACR20 responses for TNF-α inhibitors and novel biologics at 24 weeks. The square sizes represent the statistical weight for each study. Black horizontal bars represent 95% CI. Diamond values indicate pooled effect estimates. ACR20: American College of Rheumatology 20% response; TNF-α: tumor necrosis factor-α.

Forest plot of mean change in HAQ-DI scores at 24 weeks compared to baseline for TNF-α inhibitors and novel biologics. The square sizes represent the statistical weight for each study. Black horizontal bars represent 95% CI. Diamond values indicate pooled effect estimates. HAQ-DI: Health Assessment Questionnaire-Disability Index; TNF-α: tumor necrosis factor-α.
Comparing best-in-class biologics
A supplementary metaanalysis compared the biologics that performed the best for each respective outcome. Secukinumab performed best in the 4 outcomes and was compared to the best TNF-α inhibitor in each outcome (Supplementary Figure 6, available with the online version of this article). There was no difference between infliximab (RR 4.10, 95% CI 2.03–8.29) and secukinumab (pooled RR 3.19, 95% CI 2.16–4.72) for resolution of dactylitis. Golimumab (RR 2.06, 95% CI 1.28–3.31) and secukinumab (pooled RR 2.28, 95% CI 1.55–3.36) were the best-in-class for resolution of enthesitis; and there was no significant statistical difference between each biologic in the metaanalysis. Moreover, there was no difference between infliximab (pooled RR 3.38, 95% CI 2.08–5.48) and secukinumab (pooled RR 2.91, 95% CI 2.23–3.79) in the ACR20 response. Metaanalysis for HAQ-DI improvement showed no difference between adalimumab (pooled mean difference −0.25, 95% CI −0.34 to −0.16) and secukinumab (pooled mean difference −0.24, 95% CI −0.25 to −0.23).
DISCUSSION
To our knowledge, this is the first study analyzing the pooled effect of biologics on resolution of dactylitis and enthesitis in patients with PsA. The pooled random-effects analysis demonstrated significantly higher rates for resolution of dactylitis and enthesitis with biologic treatment compared to placebo at both weeks 12–14 and Week 24. Interestingly, we did not detect an appreciable difference between the previous generation TNF-α inhibitors and novel biologics targeting IL-23 and IL-17.
A previous systematic review on dactylitis treatment showed that ustekinumab, certolizumab, infliximab, and golimumab were promising candidates for treatment of dactylitis7. A metaanalysis was not possible at that time because of limited data. The current pooled analysis showed that treatments with TNF-α inhibitors and novel biologics were respectively 2.57 times and 1.88 times more likely to cause resolution of dactylitis at Week 24 than placebo, with no significant difference between these classes. Testing for subgroup differences at Week 24 also showed no significant difference between TNF-α and novel biologics due to heterogeneity (Figure 2).
A systematic review in 2014 showed that the TNF-α inhibitors golimumab, certolizumab, and infliximab were effective in treating enthesitis30. At the time, evidence for adalimumab and etanercept was inconclusive, and remains sparse to date. One RCT reported resolution of enthesitis for adalimumab and showed modest rates with a calculated ratio of 1.24 (95% CI 0.76–2.05) and 1.74 (95% CI 1.33–2.79) at weeks 12 and 24, respectively19. More robust evidence regarding enthesitis treatment is available for biologics that target the TH17 pathway. Six RCT were included in the current metaanalysis, which showed that ustekinumab, secukinumab, and ixekizumab treatment effectively resolved enthesitis compared to placebo, corresponding to an overall pooled RR for these trials of 1.95 (95% CI 1.60–2.38; Figure 3). According to the pooled analysis, there is no significant difference in enthesitis resolution rates for TNF-α inhibitors and the novel biologics. Moreover, testing for subgroup differences revealed no significant difference between the 2 biologic subgroups owing to heterogeneity (Figure 3). Our data support the role of the TH17 pathway in the pathogenesis of enthesitis, which was initially proposed based on the beneficial effect of the IL-12/23 inhibitor ustekinumab30,31.
Analyses of ACR20 and HAQ responses for biologics in PsA were conducted previously, but to our knowledge there is no metaanalysis comparing anti-TNF-α with novel biologics targeting the TH17 pathway26. Analogously to the comparable efficacy in dactylitis and enthesitis, we saw no significant differences between these 2 biologic classes in either ACR20 responses (Figure 4; Supplementary Figure 4, available with the online version of this article) or HAQ scores at Week 24 (Figure 5; Supplementary Figure 5). This result indicates that, in contrast to efficacy in psoriatic skin lesions, where novel biologics are superior to TNF-α blockers, the level of clinical and functional improvement in relation to PsA is comparable with any class of biologic drugs.
Methodologies including head-to-head comparative studies between biologics are important in revealing differences in effectiveness for the relative biologics. Previous matched comparison studies revealed discrepant results for the ACR comparison between secukinumab and adalimumab. One study32 described that patients treated with secukinumab had significantly higher ACR response compared to adalimumab, whereas another study33 showed that adalimumab was superior regarding ACR response. Metaanalysis of the ACR20 data for secukinumab versus adalimumab in our current study demonstrated no difference in ACR20 response at weeks 12–16 (Supplementary Figure 7A, available with the online version of this article). At Week 24, secukinumab had had a superior ACR20 response (pooled RR 2.91, 95% CI 2.23–3.79) compared to adalimumab (pooled RR 1.59, 95% CI 1.22–2.08; Supplementary Figure 7B). Moreover, a further metaanalysis was conducted with the biologics that performed best for the 4 outcomes of interest in our study. Secukinumab, which was superior to the other biologics in its class, was compared to the best TNF-α inhibitor. This supplementary metaanalysis revealed no statistically significant difference between the best TNF-α inhibitor versus secukinumab, with the limitation of a small sample size and a low number of studies analyzed.
A key strength of our study is the inclusion of RCT with high-quality evidence and low risk of bias. One limitation of the study is that RCT data were limited beyond 24 weeks and metaanalysis beyond this period was not possible. It is difficult to extrapolate Week 24 data to longterm outcomes, because biologics may lose efficacy at different rates during longterm treatment. Another limitation of our study includes the differences in the placebo groups between the different RCT, which contributed to an inherent source of heterogeneity for the pooled analysis. A further limitation of the studies we included is their consideration of dosing of biologics. Studies in which dose increases were allowed showed improvements in the efficacy of biologics regarding the 4 measures, suggesting that these biologics may not be dose-optimized. Further studies are required to elucidate this. As the scope of our study was to compare the 2 overall classes of biologics (anti-TNF vs novel biologics), a pairwise metaanalysis was conducted. A future study could conduct a network metaanalysis to estimate direct and indirect comparisons between the individual biologics.
Our pooled analysis demonstrated that the drugs targeting TNF-α and IL-17 and IL-12/23 effectively resolved dactylitis and enthesitis, with no significant difference between the 2 classes of biologic treatment.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Footnotes
Medical student research funding was provided by the Dorothy Jean Usher Memorial Summer Research Award. Dr. Gniadecki has received speaker’s honoraria from Janssen and AbbVie, and is on the advisory board for Janssen, AbbVie, Eli Lily, Sanofi, Novartis, and Leo Pharma.
- Accepted for publication December 11, 2018.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}