

Abstract
Objective. International recommendations for the management of axial spondyloarthritis including ankylosing spondylitis (AS) recommend a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) level of disease activity of ≥ 4 to initiate treatment with biologics. We aimed to evaluate the level of disease activity used to initiate tumor necrosis factor inhibitor (TNFi) treatment and the level of responses to treatment based on different BASDAI cutoffs.
Methods. This is a posthoc analysis of the noninterventional, prospective, GO-NICE study in the subgroup of biologic-naive AS treated with golimumab (GOL) 50 mg subcutaneously once monthly.
Results. Of the 244 biologic-naive AS patients at baseline, 70.5% had a BASDAI ≥ 4 (Group 1), 14.3% had 2.8 to < 4 (Group 2), and 15.2% had even < 2.8 (Group 3). A total of 134 patients (54.9%) completed the 24-month observational period. The mean BASDAI in Groups 1, 2, and 3 was initially 5.9 ± 1.3, 3.4 ± 0.4, and 2.0 ± 0.8, decreased to 2.2 ± 2.0, 1.9 ± 1.2, and 1.0 ± 1.2 within 3 months (all p < 0.0001 vs baseline), and decreased significantly to 2.2 ± 1.7, 1.9 ± 1.7, and 1.4 ± 1.0 at Month 24 (all p < 0.005), respectively. BASDAI 50% improvement was noted in 68.8%, 44.8%, and 45.2% of patients at Month 3, and in 84.9%, 61.9%, and 55.0% at Month 24.
Conclusion. TNFi treatment was initiated in almost a third of AS patients with lower disease activity states as assessed by BASDAI cutoff of ≥ 4. Patients with a BASDAI between 2.8 and < 4 appeared to benefit significantly from GOL treatment, while patients with BASDAI < 2.8 did not. This finding should lead to a reevaluation of the established BASDAI cutoff of ≥ 4.
Ankylosing spondylitis (AS), the “radiographic” part of the spectrum of axial spondyloarthritides, is a chronic inflammatory rheumatic disease with predominant involvement of the axial skeleton by both inflammation and new bone formation1. Treatment with TNFi is effective, as shown in a recent systematic review and a Bayesian network meta-analysis comprising 20 trials of 6 tumor necrosis factor-α inhibitors (TNFi) and 3220 participants2.
Ever since the first publication on the success of therapy with TNFi in patients with active AS3, the Bath Ankylosing Spondylitis Disease Index (BASDAI)4 cutoff of 4 and above has been used5, and published evidence from various sources support this approach6,7,8. Correspondingly, this cutoff value ≥ 4 has been recommended for use in all major international guidelines9,10,11. The current Assessment of Spondyloarthritis international Society/European League Against Rheumatism (ASAS/EULAR) recommendations for patients with axial spondyloarthritis (axSpA) define active disease by Ankylosing Spondylitis Disease Activity Score (ASDAS) ≥ 2.1 or BASDAI ≥ 4. Historically, active disease has been defined by a BASDAI level of at least 4, while ASDAS is the preferred measure today11.
However, the BASDAI threshold value has been arbitrarily set3, and has never been thoroughly evaluated. This is in contrast to the ASDAS, which has been developed on a data-driven basis12,13. Accordingly, it has remained unclear whether patients with a lower BASDAI may also benefit from therapy with biologic agents. In our personal experience, this is an issue because young male patients, especially, tend to dissimulate and report low BASDAI scores, even though they may have high C-reactive protein (CRP) levels or strong evidence of axial inflammation by magnetic resonance imaging (MRI)14.
The assessment of disease activity in AS is based on clinical variables such as inflammatory spinal pain, laboratory variables such as CRP15, and MRI. Conversely, the predictive value of baseline (BL) CRP levels on clinical and radiographic outcomes in patients with AS has been documented in many studies16,17,18.
In the GO-RAISE study with golimumab (GOL) 50 mg once monthly19,20,21, the drug was shown to be safe and effective in adult patients with AS. In that study, in AS patients treated with GOL, elevated CRP at BL or Week 14/Week 24 weakly predicted subsequent radiographic progression and modestly predicted residual spinal inflammation22.
We were interested in learning about the level of disease activity used in daily routine to start TNFi therapy, taking advantage of data obtained in the observational phase IV study GO-NICE performed in Germany, in which unselected patients with AS were treated with GOL 50 mg once monthly and observed up to 24 months23,24. In GO-NICE, clinical effectiveness was assessed in 501 patients with AS according to the German standard of care using the 10-point BASDAI to quantify disease activity4,25.
We performed a subgroup analysis of patients with AS who were categorized into 3 BASDAI groups and described regarding characteristics, treatment, and outcomes. In addition, we studied the influence of BL CRP values on clinical outcome variables in a real-world setting.
MATERIALS AND METHODS
This is a posthoc analysis of the noninterventional, multicenter, prospective, study GO-NICE (Non-Interventional Clinical Evaluation with GOlimumab) that was performed between 2010 and 2015 in a real-life setting by rheumatologists in 158 sites in all parts of Germany23,24. Patients were observed from BL up to 24 months through 8 visits performed every 3 months. Safety data were also collected, and have been reported previously23. GOL was prescribed by the treating physicians based on patients’ need for the therapy and in accordance with the recommendations of the Summary of Product Characteristics26. The treatment decision had to be made independently of data documentation and prior to the inclusion of the patients in this study.
We limited the analysis of the GO-NICE data to those with the diagnosis of established AS and who were biologic-naive, and we recorded the initial BASDAI values before the start of therapy with GOL 50 mg subcutaneously once monthly. Patients were categorized into 3 groups: patients with BASDAI ≥ 4 (Group 1); the third of patients with a BASDAI < 4 was divided into 2 equal groups: BASDAI between 2.8 and < 4 (Group 2), and BASDAI < 2.8 (Group 3). Within each group, patients were split into those with elevated CRP value (above upper limit of normal, defined as > 5 mg/l) versus non-elevated CRP. No radiographic data were collected in this observational study.
RESULTS
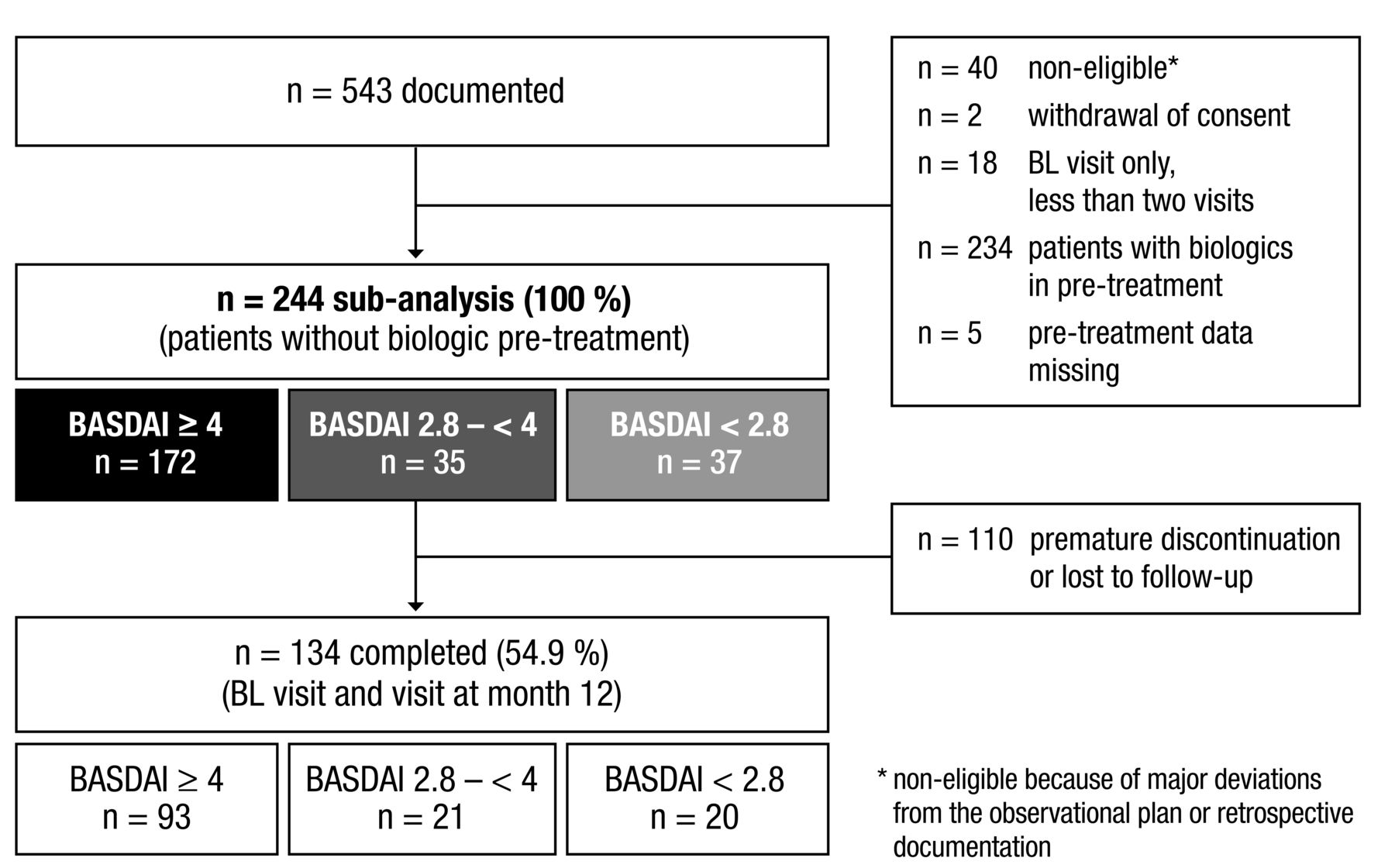
Patient disposition and flow is shown in Figure 1. Out of 543 patients with AS, 244 had not received any biologic medications for pretreatment and at least 1 documented followup visit after BL assessment and were thus eligible for analysis. Of these, 134 patients (54.9%) completed the 24-month observational period (BL until visit at Month 24).
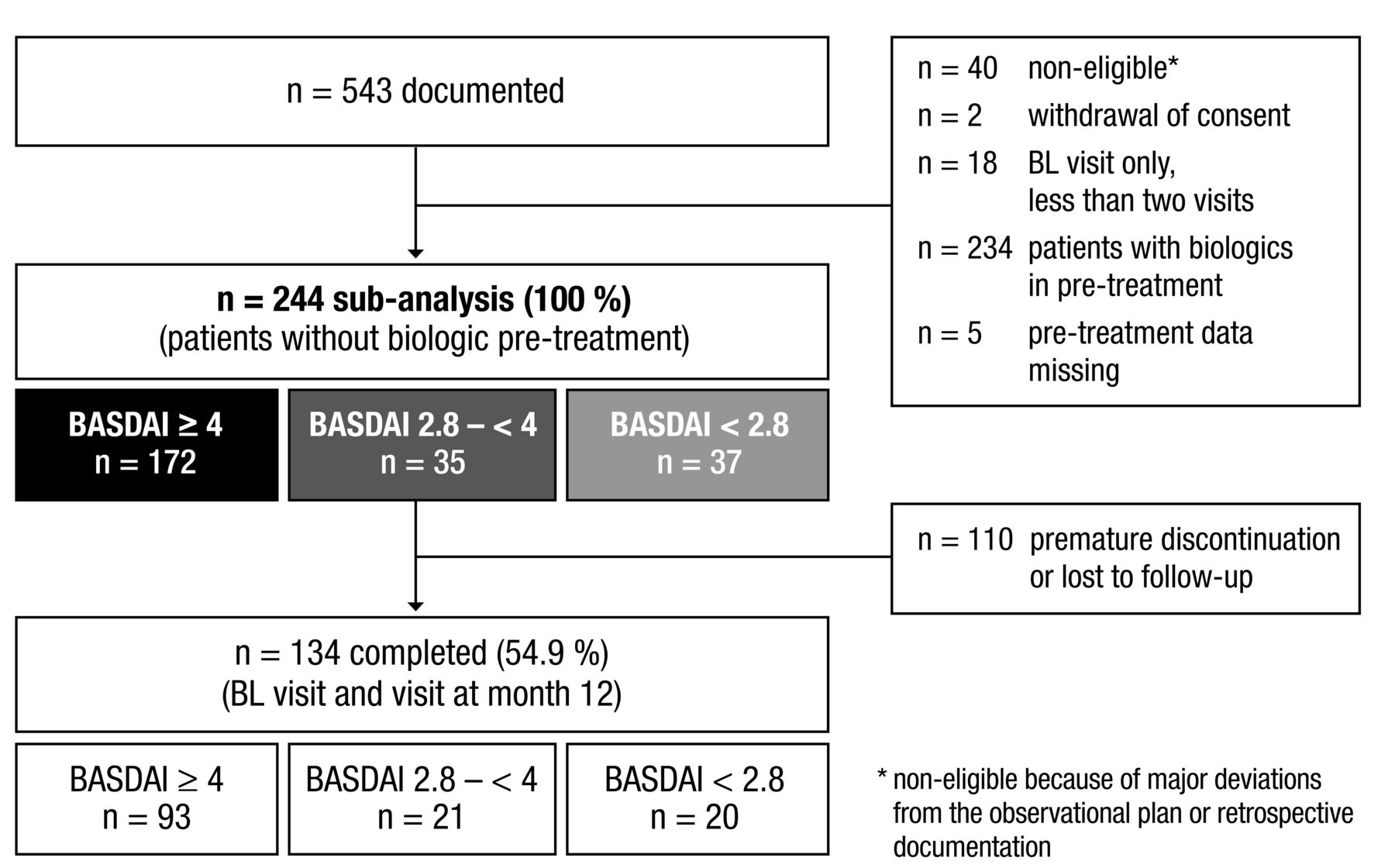
Patient disposition and flow. BL: baseline; BASDAI: Bath Ankylosing Spondylitis Disease Activity Index.
Male patients accounted for more than two-thirds in the sample (70.9%). Mean time since diagnosis was 9.0 ± 9.5 years. Mean CRP values were significantly elevated (19.7 ± 52.7 mg/l), with substantial variety across patients.
At treatment initiation, the majority of patients (70.5%) had BASDAI ≥ 4 (Group 1), 14.3% had BASDAI of 2.8 to < 4 (Group 2), and 15.2% had a BASDAI < 2.8 (Group 3).
Patient demographics did not differ much between groups; the proportion of males was numerically lower in Group 1. Of note, the proportion of patients with an elevated CRP at BL was highest in Group 2 (Table 1).
Baseline characteristics of patients eligible for posthoc analysis.
Course of BASDAI over time
The mean BASDAI in Groups 1, 2, and 3 was initially 5.9 ± 1.3, 3.4 ± 0.4, and 2.0 ± 0.8, decreased to 2.2 ± 2.0, 1.9 ± 1.2, and 1.0 ± 1.2 within 3 months (all p < 0.0001 vs BL), and decreased significantly to 2.2 ± 1.7, 1.9 ± 1.7, and 1.4 ± 1.0 at Month 24 (all p < 0.005), respectively (Figure 2).

BASDAI course by subgroup. BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; BL: baseline; M3: Month 3; ns: not significant.
In patients with a BASDAI < 2.8 at BL (Group 3), the mean score was initially 2.0 ± 0.8 and further scores ranged from 0.7 to 1.9, although some of the changes were not significant versus BL.
BASDAI 50% improvement was noted in 68.8%, 44.8%, and 45.2% of patients at Month 3, and in 84.9%, 61.9%, and 55.0% at Month 24, respectively.
Influence of CRP levels
CRP levels did not have an influence on BASDAI levels (Figures 3 and 4).
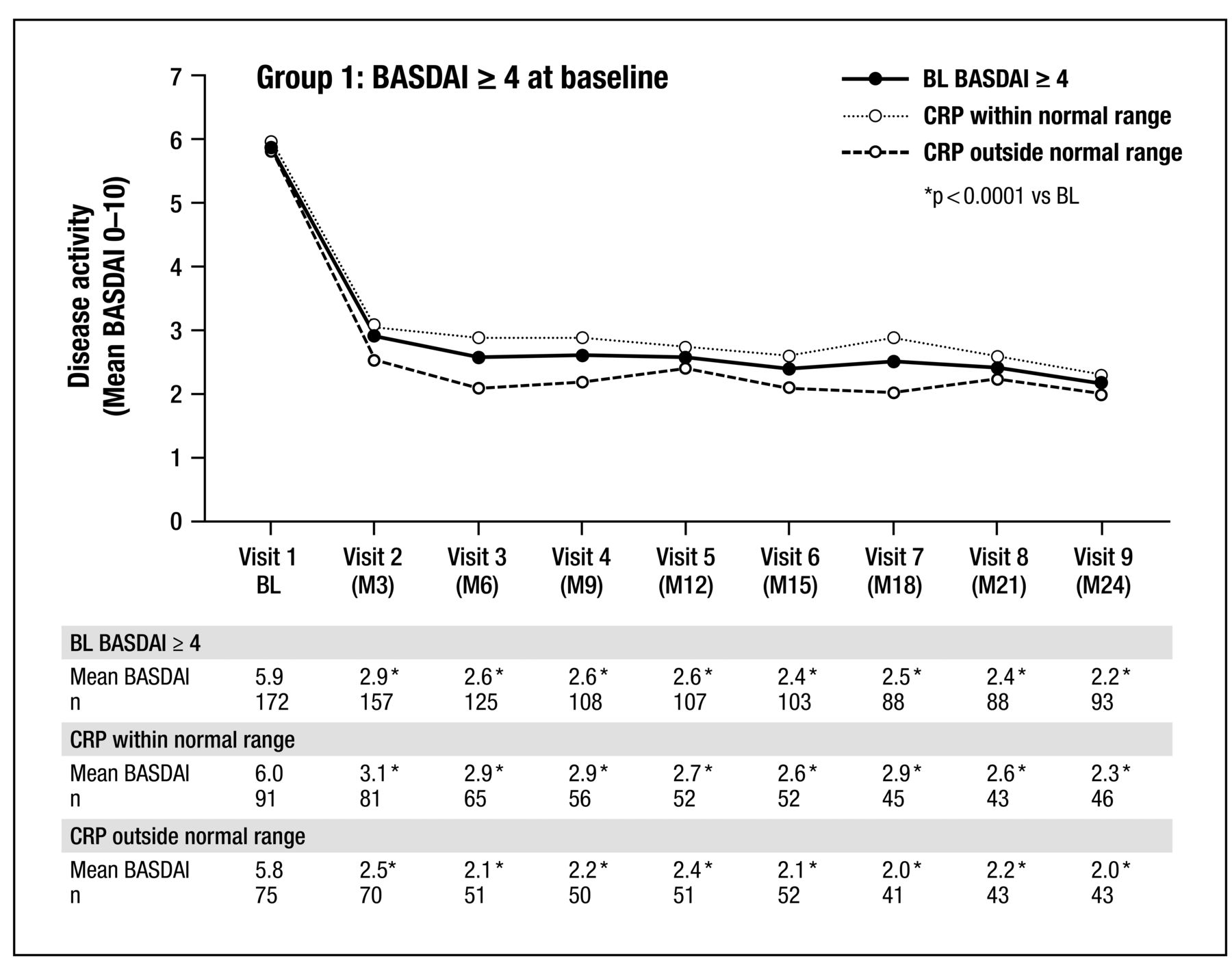
BASDAI course by Group 1 (subgroup BASDAI ≥ 4 at BL) over time and C-reactive protein (CRP). BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; BL: baseline; M3: Month 3.
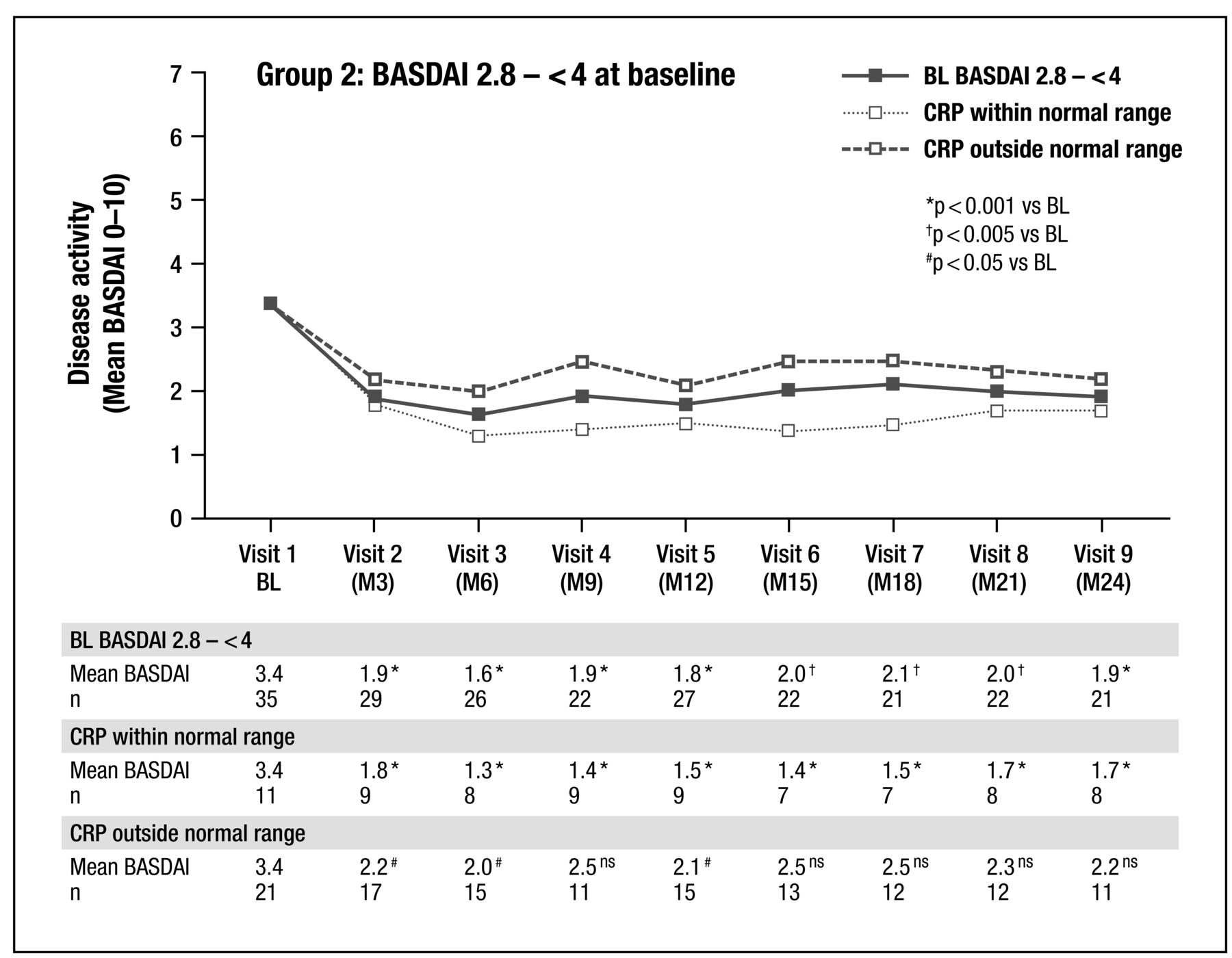
BASDAI course by Group 2 (subgroup BASDAI 2.8 to < 4 at BL) over time and C-reactive protein (CRP). BASDAI: Bath Ankylosing Spondylitis Disease Activity Index; BL: baseline; M3: Month 3; ns: not significant.
DISCUSSION
In this real-world study with unselected patients with AS who were biologic-naive and started TNFi GOL therapy, almost one-third of patients had BASDAI levels at BL that were below the recommended threshold of ≥ 4. Thus, based on the current ASAS/EULAR recommendations, those patients would not have been eligible for such therapy. If correctly documented, this result suggests that rheumatologists recognize patients who, based on the level of inflammation present as evidenced by CRP levels or MRI findings, are in need of TNFi therapy but who judge themselves lower when ticking BASDAI boxes. This well-established questionnaire is an outcome variable that is solely based on subjective clinical symptoms. This is in contrast to the ASDAS, in which subjective variables are combined with CRP as an objective variable12,13. However, patient’s global assessment (PtGA) and ASDAS were not assessed in this study because it was performed under clinical practice conditions, starting in 2010.
CRP levels in this study were higher in the groups with a low BASDAI (Groups 2 and 3). This suggests that rheumatologists sometimes weighted the presence of objective signs of inflammation higher than the subjective grading of clinical symptoms. This view is consistent with the treat-to-target concept27,28 and also with the results of recent cohort studies. Thus, these data may lead to a critical reevaluation of the current BASDAI cutoff of ≥ 4, because the burden of inflammation may, at least in some cases, be more important than the degree of clinical symptoms. This could be especially important for patients with high CRP and low BASDAI levels.
The other important observation of this study was that patients with relatively low BASDAI levels (between 2.8 and 4) still had a clear treatment response to TNFi. Absolute and relative treatment effects in patients with higher compared to lower initial BASDAI values were substantially stronger. This may be a real effect but could also represent an effect of regression to the mean29.
Because male sex30 and CRP16,17 may be associated with a better response to TNFi therapy, it seems possible that the high proportion of male patients and high CRP levels in the BASDAI 2.8–4 group has contributed to the significant treatment response in this group.
Our results are in line with a cross-sectional study performed between 2001 and 2003 in an experienced center in the UK. In that study, also about one-third of patients (36%) did not meet the criteria for TNFi therapy according to recommendations at that time6. In a representative cohort of 1023 Belgian patients with AS evaluated by 89 rheumatologists in 2004/2005, about 60% did not commence TNFi therapy31. Although the recommendations for the treatment of patients with AS made an earlier start of TNFi treatment in the disease course possible, the BASDAI criterion (≥ 4) for treatment has remained unchanged for almost 2 decades. The high proportion of patients with low disease activity receiving TNFi in this posthoc analysis of the GO-NICE study suggests that German rheumatologists are currently initiating biologic therapy differently.
Why rheumatologists decided to treat patients with lower BASDAI scores cannot be completely clarified. It seems possible that some patients who used to have higher scores in recent history had lower scores at BL assessment. Further, previous interventions prior to the BL assessment may have lowered BASDAI scores, for example, an intensive physiotherapy course32. Natural variation of symptoms and patient-reported outcome measures has been reported for patients with AS33.
Observed daily changes of BASDAI need to be interpreted with caution, however34. Patients with BASDAI < 2.8 were not considered in detail in our analysis, because the BASDAI value shows considerable intrapatient week-to-week variability; thus, repeat evaluations may be needed before starting or stopping TNFi35,36.
Our findings cannot be readily generalized, especially if a group has small patient numbers. That patients in this real-world study were treated with only 1 TNFi does not exclude that they may have responded differently to other TNFi.
Differentiation within the BASDAI categories into normal versus high CRP did not change our overall findings. Patients with elevated versus not elevated CRP at BL in a cohort of 289 patients with AS had better responses to TNFi therapy according to all response measures, but patients without elevated CRP also responded37. This is consistent with the current approval situation for TNFi in patients with active AS.
Our study has some limitations, because it was noninterventional and thus was not randomized and had no control arm. The treating physicians may have selected patients to receive GOL as compared to other treatment options. This could lead to channeling bias and confounding by indication. The relatively high lost-to-followup rate, although well comparable with other studies, may also imply some statistical uncertainty. As described above, PtGA of the disease activity was not performed and thus ASDAS could not be calculated.
The decision to start TNFi therapy always involves a combination of individualized risk, benefit, current signs and symptoms of the disease, patient characteristics, and costs. In our study, the primary reason to initiate therapy was not documented. Thus our data should be considered hypothesis-generating, and different BASDAI cutoff values should be evaluated in prospective studies.
The most interesting observation of this posthoc analysis of a real-world study is that almost one-third of the patients included in this study were not documented as having reached the internationally recommended BASDAI cutoff of ≥ 4. Further, the data show that the patients with a BASDAI 2.8 to < 4 seem to have significant benefit of TNFi therapy, while this was not the case in patients with a BASDAI < 2.8. This finding may lead to a reevaluation of the established BASDAI cutoff of ≥ 4. Finally, CRP levels seem to have had no major influence on response rates.
Acknowledgment
We thank all the investigators and patients who participated in the GO-NICE study, and all members of the study team.
Footnotes
Full Release Article. For details see Reprints and Permissions at jrheum.org
The work was supported by MSD Haar. MSD had a role in the study design and in the collection, analysis, and interpretation of the data, the writing of the manuscript, and the decision to submit the manuscript for publication.
- Accepted for publication February 13, 2019.
Free online via JRheum Full Release option








{kind=link}
{kind=link}
{kind=link}
{kind=link}